State Border Splits Neighbors Into Medicaid Haves And Have-Nots

Missouri resident Patricia Powers had no health insurance when she was diagnosed with cancer a few years ago; she and her disabled husband were struggling to get by on, at most, $1,500 a month. If they’d lived across the river in Illinois, she’d have been eligible for Medicaid.
Laura Ungar/Kaiser Health News
hide caption
toggle caption
Laura Ungar/Kaiser Health News
Patricia Powers went a few years without health insurance and was unable to afford regular doctor visits. So the Missouri resident, who lives near St. Louis, had no idea cancerous tumors were silently growing in both of her breasts.
If Powers lived just across the Mississippi River in neighboring Illinois, she would have qualified for Medicaid, the federal-state health insurance program for low-income residents that 36 states and the District of Columbia decided to expand under the Affordable Care Act. But Missouri politicians chose not to expand it — a decision some groups are trying to reverse by getting signatures to put the option on the 2020 ballot.
Powers’ predicament reflects an odd twist in the way the health care law has played out: State borders have become arbitrary dividing lines between Medicaid’s haves and have-nots, with Americans in similar financial straits facing vastly different health care fortunes. This affects everything from whether diseases are caught early to whether people can stay well enough to work.
It wasn’t supposed to be this way. The ACA, passed in 2010, called for extending Medicaid to all Americans earning up to 138% of the federal poverty level, around $17,000 annually for an individual. But the U.S. Supreme Court in 2012 let states choose whether to expand Medicaid. Illinois did, bringing an additional 650,000-plus people onto its rolls. Missouri did not, and today about 200,000 of its residents are like Powers, stuck in this geographic gap.
Powers, who was in her early 60s when diagnosed with cancer, had briefly thought about moving to another state, just to be able to get Medicaid. “You ask yourself: Where do you go? What do you do?” says Powers. “Do I look at what’s happening in Illinois, right across the river?”
A recent University of Michigan study found Medicaid expansion substantially reduced mortality rates from 2014 to 2017. The researchers said Illinois averted 345 deaths annually while Missouri had 194 additional deaths each year. The same trends held for other side-by-side states such as Kentucky (did expand) and Tennessee (did not), New Mexico (did) and Texas (did not).
Dr. Karen Joynt Maddox, co-director of the Center for Health Economics and Policy at Washington University in St. Louis, says health care providers in her border city see how the coverage differences affect people. When treating Medicaid patients from Illinois, she says, doctors know procedures, equipment and medicines will likely be covered. With uninsured Missourians, they must consider whether patients can afford even follow-up medications after heart attacks.
Nonetheless, Medicaid expansion faces significant opposition in Missouri, which is a red state — led by a Republican governor with GOP supermajorities in both legislative chambers.
Patrick Ishmael, director of government accountability for the Show-Me Institute, a Missouri free-market think tank, says offering Medicaid to people with incomes above the poverty level would drain resources from the state’s underserved poor and push up taxpayer costs. Though the federal government pays 90% of the cost of the expansion coverage, he says, Missourians contribute to that through their federal taxes. Medicaid already accounts for about a third of the state’s budget, which he says puts pressure on other priorities, like education.
“Missouri and other states need to think about whether they are a government that provides health care or a health care provider that sometimes governs,” he says.
A Missouri story
Powers, a minister in the St. Louis County suburb of Hazelwood, used to get health insurance through her husband’s job selling lumber and hardware. After he was disabled in 2009, their coverage continued on and off for a while, and her husband eventually received Medicare, the federal insurance program for people who are 65 and older or who have disabilities. But Powers had no insurance starting in 2012 as the couple struggled on, at most, $1,500 a month.
Medicaid wasn’t an option for her. Missouri could have opened the program to more adults as early as 2010, in preparation for the health care law’s expanded coverage taking effect in 2014. Without the ACA’s expansion, adults who aren’t 65-or-older or disabled don’t qualify, no matter how low their income. Missouri’s program generally covers only pregnant women and children from low-income families, and people who are poor and elderly, blind or disabled.
Powers and her husband earned too little for her to qualify for subsidies on the federal ACA marketplace, so she couldn’t afford to buy her own plan. And without insurance, Powers never saw doctors for routine health visits or screenings. She stopped taking her prescribed medications for high blood pressure and anxiety — until she could no longer do without the anti-anxiety medicine, Lexapro.
In early 2016, she discovered a place to get help when she gave her friend a ride to a St. Louis clinic for the uninsured called Casa de Salud, where health services cost less than $30.
Powers figured she’d ask about getting back onto Lexapro there. She got a thorough checkup. The doctor found a walnut-sized lump in her right breast, and a mammogram found a tumor the size of a grain of rice in her left.
A clinic caseworker helped Powers sign up for a Medicaid program for breast cancer patients. She underwent surgery in April 2016, then had 35 radiation treatments and took follow-up medications.
Powers kept thinking she could have found the cancer earlier, if only she had insurance. That would have meant less treatment and lower costs for taxpayers, who ended up footing the bill anyway. Research shows breast cancer in its earliest stage can cost half as much to treat as in later stages.
“Even if you didn’t care about the human cost, you should care about the economic cost,” says Jorge Riopedre, president and CEO of Casa de Salud. “Treating a disease at its first stage is always going to be much cheaper than treating it at its advanced stage.”
An Illinois story
In neighboring Illinois, getting Medicaid through the expansion helped Matt Bednarowicz avoid debilitating medical debt after a motorcycle crash.
The wreck crushed his left foot, requiring doctors to insert pins in it. Without Medicaid, he would have faced thousands of dollars in medical bills.
“The debt would have been greater than I could comprehend overcoming,” says Bednarowicz, who is now 29.
His Medicaid kicked in “just in the nick of time” to cover the surgery, Bednarowicz says. It also allowed him to get psychiatric help for depression. More than a year later, he’s able to get around well — even jog — and works as a caregiver for an elderly man.
Having insurance helps people like Bednarowicz stay productive, says Riopedre.
“The person who gets sick can’t work, can’t support his or her family, can’t be a consumer and buy goods. If they’re not working, they can’t pay taxes,” Riopedre says. “It just is a tidal wave of downstream effects that if we can’t get it right — it’s going to have repercussions across the nation.”
Amid controversy, future uncertain for Missouri
As the ballot measure push continues, Missouri Gov. Mike Parson, a Republican, recently created a task force to look into expanding Medicaid through a waiver allowing states to skip some federal requirements. His office referred questions to the state’s Department of Health and Senior Services, which in turn referred them to the Department of Social Services. Rebecca Woelfel, a spokeswoman for that agency, says the department doesn’t typically comment on potential ballot issues.
Ishmael, of the Show-Me Institute, says he hopes the push for expansion doesn’t get that far. He says the Medicaid system overall is wasteful, with outcomes often not fully justifying the expense. The cost of an expansion would depend on how it’s structured, he says, but “it could be a real budget-buster.”
The impact of an expansion on Missouri’s budget remains unclear. A February analysis by researchers at Washington University estimated it would be “approximately revenue-neutral.” But their estimates range widely for the first year depending on enrollment and other factors, from up to $95 million in savings for Missouri’s Medicaid program to costing $42 million more than not expanding.
Powers, whose husband died last year, says she fully supports Medicaid expansion.
But whatever happens, especially now that she’s suffering from heart failure, she’s grateful she won’t have to worry about being uninsured again. At 66, she’s now old enough for Medicare.
Kaiser Health News is a nonprofit, editorially independent program of the Kaiser Family Foundation. KHN is not affiliated with Kaiser Permanente.
College Athletes In California Can Now Be Paid Under Fair Pay To Play Act

A new California law allows college athletes to get paid in certain scenarios. That’s setting up a clash with the NCAA, the governing body of college sports.
NFL Suspends Oakland Raider Vontaze Burfict For Rest Of Season Over Head-To-Head Hit

The NFL is suspending Oakland Raiders linebacker Vontaze Burfict for the rest of the season, following a dangerous play on Sunday. Burfict, who has a history of unnecessary roughness penalties, is seen here leaving the field in Indianapolis after his most recent ejection.
Justin Casterline/Getty Images
hide caption
toggle caption
Justin Casterline/Getty Images
The NFL is suspending Oakland Raiders linebacker Vontaze Burfict without pay for the rest of the 2019 season, after Burfict lowered his head to make helmet-to-helmet contact during a tackle this weekend.
“The discipline marks the longest punishment ever handed down for an on-field act in NFL history,” NFL.com says in regard to Burfict, who has repeatedly violated the league’s unnecessary roughness rules.
Burfict was ejected Sunday after his hit on Indianapolis Colts tight end Jack Doyle, who had just caught a pass in the middle of the field and was partly on the ground when the linebacker lowered the crown of his helmet and plowed into Doyle’s head. A suspension seemed certain — but on Monday, the NFL said it has seen enough of Burfict this year.
YouTube
“There were no mitigating circumstances on this play,” Jon Runyan, NFL vice president of football operations, said in a letter to Burfict. “Your contact was unnecessary, flagrant and should have been avoided.”
Runyan — who had a 14-year NFL career as an offensive tackle before moving into politics and then back to the NFL — noted that he and other officials have repeatedly warned Burfict that he would face increasingly stiff punishments if he continued to break the game’s rules.
“However, you have continued to flagrantly abuse rules designated to protect yourself and your opponents from unnecessary risk,” Runyan said in his letter.
Under the league’s labor agreement, players have the right to appeal a suspension within three days; Burfict plans to appeal the punishment, according to NFL.com. The league’s site also notes that Burfict has been either suspended or fined 13 times over the course of his more than seven pro seasons.
This is Burfict’s first season with the Oakland Raiders, having signed a one-year contract to join the team after seven tumultuous years with the Cincinnati Bengals.
Burfict was at the center of an infamous incident in 2016, when he launched himself into the head of then-Pittsburgh Steelers wide receiver Antonio Brown — a vicious hit that helped to end the Bengals’ playoff run, in a wildcard game they had been close to winning.
Brown, who is now without an NFL team after accusations of sexual assault, was briefly Burfict’s teammate in Oakland this year.
Burfict’s penchant for breaking his sport’s rules dates back to his college career at Arizona State University: He once collected three personal fouls in just one half of a football game.
A Biopsy Came With An Unexpected $2,170 ‘Cover Charge’ For The Hospital

An unexpected charge related to a biopsy threatened the financial security of Brianna Snitchler and her partner.
Callie Richmond for Kaiser Health News
hide caption
toggle caption
Callie Richmond for Kaiser Health News
Brianna Snitchler was just figuring out the art of adulting when she scheduled a biopsy at Henry Ford Hospital in Detroit.
Snitchler, 27, was on top of her finances: Her student loan balance was down and her credit score was up.
“I had been working for the past three years trying to improve my credit and, you know, just become a functioning adult human being,” Snitchler said.
For the first time in her adult life, she had health insurance through her job and a primary care doctor she liked. Together they were working on Snitchler’s concerns about her mental and physical health.
One concern was a cyst on her abdomen. The growth was about the size of a quarter, and it didn’t hurt or particularly worry Snitchler. But it did make her self-conscious whenever she went for a swim.
“People would always call it out and be alarmed by it,” she recalled.
Share Your Story And Bill With Us
If you’ve had a medical-billing experience that you think we should investigate, you can share the bill and describe what happened here.
Before having the cyst removed, Snitchler’s doctor wanted to check the growth for cancer. After a first round of screening tests, Snitchler had an ultrasound-guided needle biopsy at the Henry Ford Health System’s main hospital.
The procedure was “uneventful,” with no complications reported, according to results faxed to her primary care doctor after the procedure. The growth was indeed benign, and Snitchler thought her next step would be getting the cyst removed.
Then the bill came.
The patient: Brianna Snitchler, 27, a user-experience designer living in Detroit at the time. As a contractor for Ford Motor Co., she had a UnitedHealth Group insurance plan.
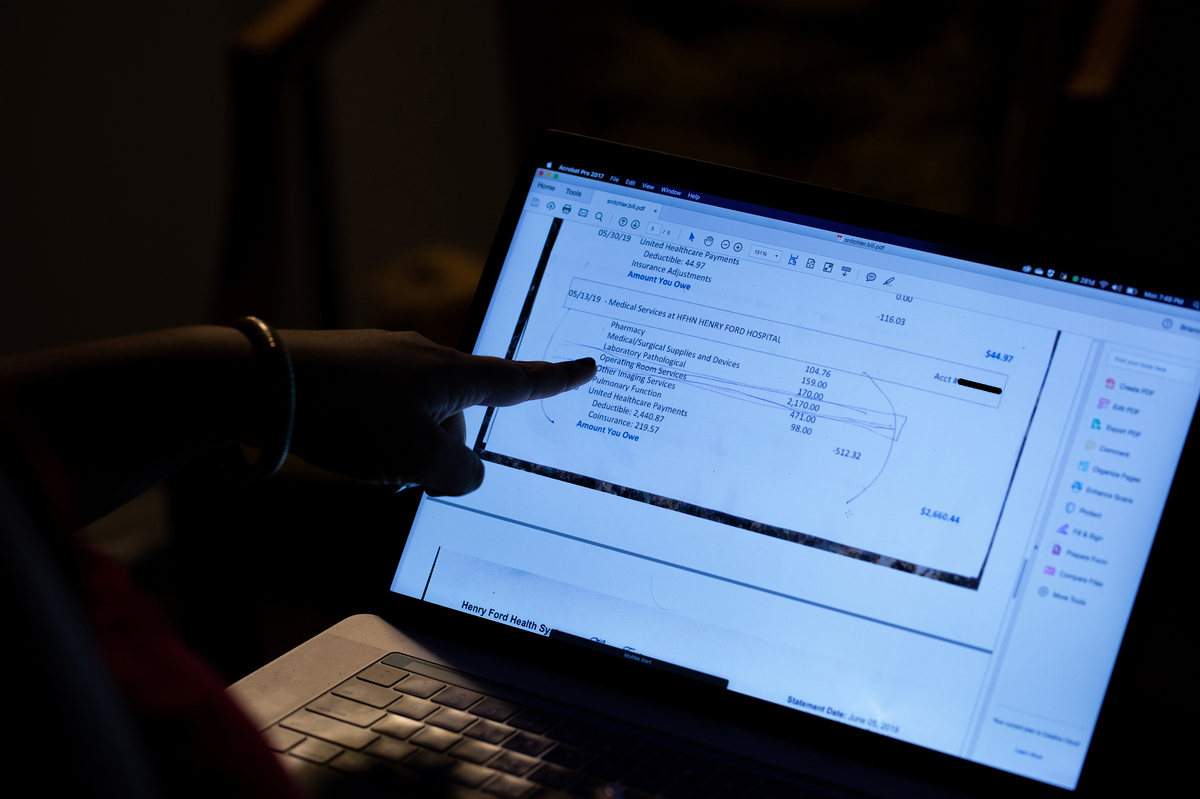
Total bill: $3,357.52, including a $2,170 facility fee listed as “operating room services.” The balance included a biopsy, ultrasound, physician charges and lab tests.
Service provider: Henry Ford Health System in Detroit.
Medical procedure: Ultrasound-guided needle biopsy of a cyst.
What gives: When Snitchler scheduled the biopsy, no one told her that Henry Ford Health System would also charge her a $2,170 facility fee.
Snitchler said the bill turned out to be far more than what she had budgeted for. Her insurance plan from UnitedHealth had a high deductible of $3,250, plus she would owe coinsurance. All told, her bills for the care she received related to the biopsy left her on the hook for $3,357.52, with her insurance paying $974.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
When Brianna Snitchler scheduled the biopsy for a cyst on her abdomen, no one told her that the Henry Ford Health System would charge a $2,170 facility fee, listed on her bill as “operating room services.” (Note: This photo has been edited to redact private information.)
Callie Richmond for Kaiser Health News
hide caption
toggle caption
Callie Richmond for Kaiser Health News
“She shrugged it off,” Snitchler’s partner, Emi Aguilar, recalled. “But I could see that she was upset in her eyes.”
Snitchler panicked when she realized the bill threatened the couple’s financial security. Snitchler had already spent down her savings for a recent cross-country move to Austin, Texas.
In an email, Henry Ford spokesman David Olejarz said the “procedure was performed in the Interventional Radiology procedure room, where the imaging allows the biopsy to be much more precise.”
“We perform procedures in the most appropriate venue to ensure the highest standards of patient quality and safety,” Olejarz wrote.
The initial bill from Henry Ford referred to “operating room services.” The hospital later sent an itemized bill that referred to the charge for a treatment room in the radiology department. Both descriptions boil down to a facility fee, a common charge that has become controversial as hospitals search for additional streams of income, and as more patients complain they’ve been blindsided by these fees.
Hospital officials argue that medical centers need the boosted income to provide the expensive care sick patients require, 24 hours a day, 365 days a year.
But the way hospitals calculate facility fees is “a black box,” said Ted Doolittle, with the Office of the Healthcare Advocate for Connecticut, a state that has put a spotlight on the issue.
“It’s somewhat akin to a cover charge” at a club, said Doolittle, who previously served as deputy director of the federal Center for Program Integrity at the Centers for Medicare & Medicaid Services.
Hospitals in Connecticut billed more than $1 billion in facility fees in 2015 and 2016, according to state records. In 2015, Connecticut lawmakers approved a bill that forces all hospitals and medical providers to disclose facility fees upfront. Now patients in Connecticut “should never be charged a facility fee without being shown in burning scarlet letters that they are going to get charged this fee,” Doolittle said.
In Michigan, there’s no law requiring hospitals and other providers of health care services to inform patients of facility fees ahead of time.
Snitchler’s procedure took place on campus at Henry Ford’s main hospital site. When she got her bill, with its mention of “operating room services,” she was baffled. Snitchler said the room had “crazy medical equipment,” but she was still in her street clothes as a nurse numbed her cyst, and she was sent home in a matter of minutes.
With Snitchler’s permission, Kaiser Health News shared her itemized bill, biopsy results and explanation of benefits with Mark Weiss, a radiologist who leads MediCrew, a company in Flint, Mich., that helps patients navigate the health system.
Weiss said it probably wasn’t medically necessary for Snitchler to go to the hospital to receive good care. “Not all surgical procedures have to be done at a surgical center,” he said, noting that biopsies often can be done in an office-based treatment center.
Resolution: Hoping for a reasonable explanation — or even the discovery of a mistake — Snitchler called her insurance company and the hospital.
A representative at Henry Ford told her on the phone that the hospital isn’t “legally required” to inform patients of fees ahead of time.
In an email, Henry Ford spokesman Olejarz apologized for that response: “We’ll use it as a teachable moment for our staff. We are committed to being transparent with our patients about what we charge.”
He pointed to an initiative launched in 2018 that helps patients anticipate out-of-pocket expenses. The program targets the most common elective radiology and gastroenterology tests that often have high price tags for patients.
Asked if Snitchler’s ultrasound-guided needle biopsy will be included in the price transparency initiative, Olejarz replied, “Can’t say at this point.”
In addition to the pilot program to inform patients of fees, Olejarz said, the hospital also plans to roll out an online cost-estimator tool.
For now, Snitchler has decided not to get the cyst removed, and she plans to try to negotiate on her bill. She has not yet paid any portion of it.
“You should always negotiate; you should always try,” Doolittle said. “Doesn’t mean it’s going to work, but it can work. People should not be shy about it.”
“We are happy to work out a flexible payment plan that best meets her needs,” Olejarz wrote when Kaiser Health News first inquired about Snitchler’s bill.
The takeaway: When your doctor recommends an outpatient test or procedure like a biopsy, be aware that the hospital may be the most expensive place you can have it done. Ask your physician for recommendations of where else you might have the procedure, and then call each facility to try to get an estimate of the costs you’d face.
Also, be wary of places that may look like independent doctor’s offices but are owned by a hospital. These practices also can tack hefty facility fees onto your bill.
If you get a bill that seems inflated, call your hospital and insurer and try to negotiate it down.
Bill of the Month is a crowdsourced investigation by Kaiser Health News and NPR that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it!
California Governor Signs Bill Allowing College Athletes To Profit From Endorsements

{kind=link}
UCLA players celebrate during a game against the Arizona Wildcats at the Rose Bowl last year in Pasadena, Calif. Gov. Gavin Newsom has signed a bill paving the way for college athletes in the state to hire agents and sign endorsement deals.
Victor Decolongon/Getty Images
hide caption
toggle caption
Victor Decolongon/Getty Images
Updated at 12:17 p.m. ET
In a move that puts California on a collision course with the NCAA, Gov. Gavin Newsom has signed a bill effectively allowing college athletes in the state to earn compensation for the use of their likeness, sign endorsement deals and hire agents to represent them.
The governor signed the measure in a segment released Monday by Uninterrupted, a sports programming company co-founded by LeBron James.
Newsom proclaimed the move as “the beginning of a national movement — one that transcends geographic and partisan lines.”
“Collegiate student athletes put everything on the line — their physical health, future career prospects and years of their lives to compete. Colleges reap billions from these student athletes’ sacrifices and success but, in the same breath, block them from earning a single dollar,” he said in a statement. “That’s a bankrupt model — one that puts institutions ahead of the students they are supposed to serve. It needs to be disrupted.”
Colleges reap billions from student athletes but block them from earning a single dollar. That’s a bankrupt model.
I just signed the Fair Play to Pay Act with @KingJames — making CA the first state to allow student athletes to profit off their name, image, and likeness. pic.twitter.com/aWE9OL9r1v
— Gavin Newsom (@GavinNewsom) September 30, 2019
California is the first state to pass such a law, which is to take effect on Jan. 1, 2023.
That marks a significant shift from the current policies enforced by the NCAA, collegiate sports’ national governing body, which generally renders student-athletes ineligible to accept compensation for “the use of his or her name or picture to advertise, recommend or promote directly the sale or use of a commercial product or service of any kind.”
And the NCAA Board of Governors pushed back hard against the bill at the time of its passage in the Legislature, saying that it would leave the playing field for universities of different sizes radically uneven.
“Right now, nearly half a million student-athletes in all 50 states compete under the same rules,” the 22-member panel composed mostly of university presidents and athletic directors said in a letter to Newsom on Sept. 11. “This bill would remove that essential element of fairness and equal treatment that forms the bedrock of college sports.”
On Monday, shortly after Newsom’s announcement, the NCAA released another, slightly more conciliatory statement — one acknowledging that “changes are needed to continue to support student-athletes” but also warning that “this new law already is creating confusion for current and future student-athletes, coaches, administrators and campuses, and not just in California.”
“We will consider next steps in California,” the group added, “while our members move forward with ongoing efforts to make adjustments to NCAA name, image and likeness rules that are both realistic in modern society and tied to higher education.”
NCAA statement on Gov. Newsom signing SB 206: https://t.co/laV4aT1Cpo pic.twitter.com/sCOOYZEkJd
— NCAA (@NCAA) September 30, 2019
The financial stakes of the dispute are massive.
Between TV rights, marketing fees and other avenues — particularly for its major cash cow, the NCAA Division I men’s basketball tournament — the organization has reported annual revenues cresting $1 billion.
The NCAA maintains that it converts much of that intake into crucial opportunities for student-athletes, saying it has “provided billions of dollars in scholarships and the opportunity for millions across 24 sports to earn undergraduate and graduate degrees.”
That hasn’t silenced critics, who have grown louder in recent years amid a recent spate of high-profile investigations — including efforts by the FBI — looking into alleged corrupt recruiting practices in NCAA men’s basketball. The hefty punishments levied against schools and players by the national governing body has focused a spotlight on why the competitors featured in such a lucrative industry are left out of its profits.
Michael Sokolove, who wrote of the massive scandal at the University of Louisville’s basketball program in The Last Temptation Of Rick Pitino, talked to Fresh Air last year about one notable discrepancy.
“If you look at a program like Louisville, which is a program that I focused on, they generate about $45 million a year in revenue. They give out 13 scholarships. That adds up to about $400,000 a year. The rest of it gets spread out to the coach, who makes $8 million a year, to the assistant coaches, who make as much as a half-million dollars a year,” Sokolove said.
“All throughout the athletic department, people are making six-figure salaries. It does not go to the players, what I call the unpaid workforce.”
Pushback also has come from a number of prominent athletes, including James, who opted to skip college basketball entirely to head straight to the NBA — before the pro league implemented a minimum age requirement in 2006, barring others from following James’ path.
“Part of the reason I went to the NBA is to get my mom out of the situation that she was in,” James said in the informal signing ceremony with Newsom that was held on a barbershop set. “I couldn’t have done that if I would have stepped on a college campus.”
Others, such as NFL cornerback Richard Sherman, have rejected the notion put forward by the NCAA and others that a free college education is recompense enough for the amount of work these athletes put in. Sherman told Sports Illustrated in 2015 that he would “love for a regular student to have a student-athlete’s schedule during the season for just one quarter or one semester and show me how you balance that.”
“People think, ‘Oh, you’re on scholarship.’ They pay for your room and board, they pay for your education, but to their knowledge, you’re there to play football,” said Sherman, who got his degree from Stanford University. “You’re not on scholarship for school and it sounds crazy when a student-athlete says that, but those are the things coaches tell them every day: ‘You’re not on scholarship for school.’ “
Saturday Sports: Minnesota Twins, Santa Anita Horse Deaths
We have a recap on stories from the week in sports.
SCOTT SIMON, HOST:
I look forward all week to saying it’s time for sports.
(SOUNDBITE OF MUSIC)
SIMON: Homers a-poppin’ (ph) this baseball season. And for the first time, four teams have reached 100 wins. Yeah, guess who wasn’t one of those four. Meanwhile, racing resumes in Santa Anita after more than 30 horses died there last season. NPR’s Tom Goldman joins us. Good morning, Tom.
TOM GOLDMAN, BYLINE: Hi, Scott.
SIMON: And I was astonished to discover this week that apparently baseball season is going on for some clubs. I mean, I thought after that Cubs-Cardinals series, they would just call the rest of the season off. But…
GOLDMAN: Let it go. Let it go.
SIMON: There – (singing) let it go. There’s been a record number of homers this season. The Minnesota Twins became the first team to hit 300 in a season. Yankees overtook them last night. Is the ball juiced, or is just everybody taking that supplement Frank Thomas advertises?
GOLDMAN: (Laughter) And he looks great, doesn’t he?
SIMON: He does look great, yeah.
GOLDMAN: He really does.
You know, not too long ago, we would be wondering about supplements and more powerful substances, but we’re told the so-called steroids era in Major League Baseball is over. Testing is rigorous. Science and a lot of pitchers, Scott, say it’s the ball’s fault – not enough drag on the balls, so they’re flying out. And there’s growing concern that all these home runs are bad for the game – less action on the field when guys are doing a home run trot around the bases while everyone else on the field watches.
There’s speculation change is coming. The balls may be altered, perhaps adding more drag.
SIMON: I wonder – I shouldn’t ask you without – I wonder if anybody stole home this year. I don’t remember seeing it. Do you?
GOLDMAN: I don’t remember seeing it, but I did not see every game.
SIMON: Yeah, all right.
And all the talk about the Astros, Dodgers and Yankees. What a season for the Twins. My gosh. They beat Kansas City last night for their 100th win, 6-2. And this is a small-payroll team in a modest but wonderful market.
GOLDMAN: It is. And the only other time the Twins did this was in 1965. And this time, it’s history. First time there have been four teams with at least a hundred wins in a season. Now, at the same time, way at the other end of things, there were four teams that lost at least a hundred games, and that ties a record of most teams in the season with at least a hundred losses. That was back in 2002.
So you have this situation of haves and have-nots causing more fretting in baseball, which prides itself on parity in recent years.
SIMON: Yeah.
GOLDMAN: The baseball rulers don’t seem too worried. They say these kinds of extremes are cyclical, and they work themselves out.
SIMON: Santa Anita Park is up and running again after an array of reforms designed to make racing safer. A 23-day autumn meet is underway now. Track officials say that they’ve made changes for the safety of the athletes, who happen to be horses. What kind of changes?
GOLDMAN: Well, here are a few. All racing entries have to have a pre-race form signed by a veterinarian saying there are no known problems with a horse that should keep it from racing. Veterinarians are also expecting – inspecting all horses scheduled for training. Santa Anita track has a new drainage system that’s supposed to help with the track surface – making it safer for horses.
There’s a lot of scrutiny as this fall meet opens, Scott. Santa Anita can’t afford to have another spate of horse deaths like before. And there’s a lot of optimism that the troubles are behind. But we should note just 10 days ago, a horse had to be euthanized…
SIMON: Yeah.
GOLDMAN: …After a training injury, making it 31 fatalities since last December.
SIMON: Oh, my word. Well, NPR’s Tom Goldman, thanks so much.
GOLDMAN: You’re welcome.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
The Health Benefits At The Center Of The United Auto Workers Strike
A key issue in the contract dispute between General Motors and the United Auto Workers is health benefits. Workers have had famously great health plans, paying just 3% of costs.
SCOTT SIMON, HOST:
The United Auto Workers strike of about 50,000 General Motors workers is about to enter its third week. A key issue in the contract dispute is health benefits. The company argues that it cannot shoulder rising health costs. Union members want to hang onto their famously great health plans. Workers mostly pay no premiums, $25 for a doctor’s visit and just a few dollars for prescriptions. NPR’s Selena Simmons-Duffin wondered how’d they get those plans.
SELENA SIMMONS-DUFFIN, BYLINE: To answer that question, let’s go back to 1950. The country had just made it through the Depression, two world wars…
ERIK LOOMIS: By 1950, the economy is pretty much booming.
SIMMONS-DUFFIN: Erik Loomis is a history professor at the University of Rhode Island.
LOOMIS: It creates a massive consumer market for a lot of products in the United States, very much including automobiles.
(SOUNDBITE OF ARCHIVED RECORDING)
UNIDENTIFIED PERSON #1: More and more people are driving this car and buying this car.
SIMMONS-DUFFIN: Automakers were scrambling to meet the demand, but they had to bargain with the unionized workforce. The UAW was well-organized, had connections in high places. And what it wanted to get with this leverage was a role in automakers decisions – how many workers to hire, what kind of cars to make, whether to keep factories open.
LOOMIS: And the companies totally resisted this.
SIMMONS-DUFFIN: So the UAW called lots of strikes, which were costly. Finally in 1950, a historic agreement.
LOOMIS: The Treaty of Detroit. And that is a compromise between the UAW and the Big Three automakers that basically says that the UAW will give up its demands to open company books and have control over production decisions. In exchange for that, the workers themselves will get massive wage increases and significant benefit packages.
SIMMONS-DUFFIN: One of those benefits, health insurance, which was kind of a new-fangled idea. Medical care was just starting to be something that might cure you and cost you. Insurers were cropping up saying, hey, why not pay a little at a time instead of all at once.
(SOUNDBITE OF ARCHIVED RECORDING)
UNIDENTIFIED PERSON #2: What I don’t worry about is our health care. We’ve joined Cigna Health Plan.
SIMMONS-DUFFIN: These benefits were actually a good deal for employers. There were tax advantages. More and more companies began to offer health plans to their employees. And union autoworkers, with their benefits, got back to building cars.
(SOUNDBITE OF ARCHIVED RECORDING)
UNIDENTIFIED PERSON #3: Modern assembly is timing and teamwork as well as organization.
SIMMONS-DUFFIN: Loomis says back in the 1960s, the idea of a company covering the full cost of health benefits wasn’t that unusual.
LOOMIS: You don’t really see workers have to begin to cover large chunks of their health care until the 1980s.
SIMMONS-DUFFIN: The incredible thing is that the UAW hung on to their low-cost benefits as the rest of us began to pay more and more. Today, workers on employee plans pay about 30% of their health care costs. UAW workers pay about 3%. Not that it’s been easy for the unions, says Kristin Dziczek. She’s vice president of the Center for Automotive Research.
Is it a struggle in every contract negotiation or is it…
KRISTIN DZICZEK: Yes, absolutely. Every time this is a big struggle.
SIMMONS-DUFFIN: Especially as health care costs have gone up for everyone. Dziczek says today GM and other automakers argue the cost of these health benefits is unsustainable. GM told NPR it cost $900 million in 2018.
DZICZEK: The impression is that the employer is paying. But in reality, the employees, the union is paying here as well because the increasing costs of medical care and benefits is eating into their ability to get wage or other benefit gains. It eats up a bigger and bigger share of the amount of money that’s on the table.
SIMMONS-DUFFIN: Even if this time the union manages to preserve their enviable health benefits, next time the contract is up, they’ll have to fight to keep them once again. Selena Simmons-Duffin, NPR News.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
U.S. Justice Department Charges 35 People In Fraudulent Genetic Testing Scheme

{kind=link}
In the alleged scheme, Medicare beneficiaries were offered, at no cost to them, genetic testing to estimate their cancer risk.
Al Drago/Bloomberg/Getty Images
hide caption
toggle caption
Al Drago/Bloomberg/Getty Images
In announcing a crackdown Friday on companies it says were involved in fraudulent genetic testing, the U.S. Department of Justice brought charges against 35 individuals associated with dozens of telemarketing companies and testing labs.
The federal investigation, called Operation Double Helix, went after schemes that allegedly targeted people 65 and older. According to the charges, the schemes involved laboratories paying illegal kickbacks and bribes to medical professionals who were working with fraudulent telemarketers, in exchange for the referral of Medicare beneficiaries.
DOJ officials say the schemes cost the Medicare program more than $2 billion in unnecessary charges.
Among those charged were 10 medical professionals, including nine doctors.
“The elderly and disabled are being preyed upon,” says Joe Beemsterboer, senior deputy chief of the fraud section in the criminal division of the DOJ.
It was one of the largest health care fraud schemes in U.S. history, Beemsterboer, says, and it worked on many levels, involving many players — from “those collecting patient information, to those selling it, to those doctors corruptly prescribing these genetic tests, to the labs corruptly billing the Medicare program.”
According to Shimon Richmond, assistant Inspector General for investigations with the U.S. Department of Health and Human Services, this is how the alleged scheme worked: First, telemarketing companies trolled elderly Medicare beneficiaries online, or called them on the phone or even sent people to approach beneficiaries face-to-face at health fairs, senior centers, low-income housing areas or religious institutions like churches and synagogues.
Seniors were offered, at no cost to them, genetic testing to estimate their cancer risk or determine how well certain drugs would work for them. All they had to do, the elderly people were told, was provide their Medicare information, a copy of their driver’s license and a bit of DNA collected from a swab of saliva from inside their cheek.
The sales pitch also included lots of aggressive scare tactics, Richmond says, such as telling patients that if they didn’t have the testing done they could end up suffering from a variety of possibly fatal conditions.
Once recruiters got the information they wanted, they would try to get the patient’s own health care provider to write a prescription for the test. If that didn’t work, the recruiters asked one of their own cadre of doctors to write prescriptions for patients they didn’t know.
“And these doctors, in many cases, have zero contact with the patient and no knowledge of their health care situation or needs,” Richmond says.
The genetic test may have been offered free to the patients, but there was money to be made from Medicare reimbursement. Typically that payment – anywhere from $10,000 to $18,000 or more, Richmond says — would be split between the worker who recruited the patient, the doctor writing the prescription, the lab that did the test and the telemarketing company that organized the alleged scheme.
Often, the labs didn’t even send results to patients, Richmond says. And when they did there was no counseling or help interpreting the findings.
“So patients were left with a report that’s meaningless to them, and is certainly not providing them with any benefit in terms of their health care,” says Richmond.
The testing could also financially harm the patient down the road, he adds. For example, if, in the future, the patient’s legitimate doctor determines that the patient actually needs a genetic test for a certain condition, Medicare likely won’t cover it, citing an earlier payment.
The U.S. Department of Health and Human Services Office of Inspector General has previously issued a fraud alert for consumers in an effort to educate the public about such schemes.
Richmond says people who believe they may have been victimized by the schemes can call 1-800-HHS-TIPS, or they can file a complaint online.
If convicted, the defendants arrested Friday could face decades in prison, Beemsterboer says.
CDC Zeroing In On THC-Based Vaping Products As A Major Source Of Lung Injuries
Health officials say people with vaping-related illness have used more than 200 products sold under 87 brands. That’s complicating efforts to identify the substances contributing to lung damage.
Justice Department Charges 35 People With Defrauding Medicare Of More Than $2 Billion
The Justice Department has charged 35 individuals with defrauding Medicare of more than $2 billion. The scheme allegedly involved bribes and kickbacks for genetic tests to predict cancer.