No Mercy: How A Kansas Town Is Grappling With Its Hospital’s Closure

Fort Scott, Kan., fills up on weekday afternoons as locals grab pizza, visit a coffeehouse or browse antique shops and a bookstore. Like other rural communities, the commercial areas also include empty storefronts.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
A slight drizzle had begun in the gray December sky outside Community Christian Church as Reta Baker, president of the local hospital, stepped through the doors to join a weekly morning coffee organized by Fort Scott, Kan.’s chamber of commerce.
The town manager was there, along with the franchisee of the local McDonald’s, an insurance agency owner and the receptionist from the big auto sales lot. Baker, who grew up on a farm south of town, knew them all.
Still, she paused in the doorway with her chin up to take in the scene.
Just a few months before, Baker and the hospital’s owner, St. Louis-based Mercy health system, publicly announced that the 132-year-old hospital would close.
“Nobody talked to me after the announcement,” she said.
Baker, who says she has “taken a lot of heat” for how she broke the news, had carefully orchestrated face-to-face meetings with doctors and nurses in the final days of September. On Oct. 1, she met in person with the Mercy Hospital Fort Scott staff and then key community leaders before sending notices to the local newspaper and radio stations.
But for the 7,800 people of Fort Scott, about 90 miles south of Kansas City, Kan., the hospital’s closure was a loss they never imagined possible.
“Babies are going to be dying,” said longtime resident Darlene Doherty, who was at the coffee gathering. “This is a disaster.”
Bourbon County Sheriff Bill Martin stopped on his way out of the morning coffee to say the closure has “a dark side.” And Dusty Drake, the lead minister at Community Christian Church, diplomatically said people have “lots of questions,” adding that members of his congregation will lose their jobs.

Reta Baker, president of Mercy Hospital in Fort Scott, Kan., began as a staff nurse in 1981 and “has been here ever since.” The hospital closed at the end of 2018.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
Yet, even as this town deals with the trauma of losing a beloved institution, deeper national questions underlie the struggle: Do small communities like Fort Scott need a traditional hospital at all? And if not, how will they get the health care they need?
Sisters of Mercy nuns opened Fort Scott’s 10-bed frontier hospital in 1886 — a time when traveling 30 miles to see a doctor was unfathomable and when most medical treatments were so primitive they could be dispensed almost anywhere.
Now, driving the four-lane highway north to Kansas City, Kan., or crossing the state line to Joplin, Mo., and back is a day trip that includes shopping and a stop at a favorite restaurant. The bigger hospitals there offer the latest sophisticated treatments and equipment.
And when patients here get sick, many simply go elsewhere. An average of nine patients a day stayed in Mercy Hospital Fort Scott’s more than 40 beds from July 2017 through June 2018. And these low occupancy numbers are common: Forty-five Kansas hospitals report an average daily census of fewer than two patients.
James Cosgrove, who directed a U.S. Government Accountability Office study about rural hospital closures, said the nation needs a better understanding of what the closures mean to the health of people in rural America, where the burden of disease — from diabetes to cancer — is often greater than in urban areas.

Source: countyhealthrankings.org, the County Health Rankings & Roadmaps collaboration of the Robert Wood Johnson Foundation and the University of Wisconsin Population Health Institute
What happens when a 70-year-old grandfather slips on an icy sidewalk and must choose between staying home and driving to the closest emergency department, 30 miles away? Where does the sheriff’s deputy who picks up an injured suspect take his charge for medical clearance before going to jail? And how does a young mother whose toddler fell against the coffee table and now has a gaping head wound get her treated?
There is also the question of how the hospital going out of business will affect the town’s economy, since, as is often the case in rural America, Fort Scott’s hospital has been a primary source of well-paying jobs and attracts professionals to the community.
The GAO plans to complete a follow-up study later this year on the fallout from rural hospital closures. “We want to know more,” Cosgrove said. The original report was requested in 2017 by then-Sen. Claire McCaskill, D-Mo., and Rep. Tim Walz, D-Minn., and has been picked up by Sen. Gary Peters, D-Mich.
In Fort Scott, the answers to these questions are unfolding — painfully — in real time.
At the end of December, the Mercy system closed Fort Scott’s hospital but decided to keep the building open to lease portions to house an emergency department, outpatient clinic and other services. Mercy Fort Scott joined a growing list of more than 100 rural hospitals that have closed nationwide since 2010, according to data from the University of North Carolina’s Cecil G. Sheps Center for Health Services Research. How the town copes is a window into what comes next.
‘We were naive’
Over time, the Mercy hospital in Fort Scott became so much a part of the community that parents counted on the hospital’s ambulance standing guard at the high school’s Friday night football games.
The hospital seemed to be everywhere, actively promoting population health initiatives by working with the school district to lower children’s obesity rates as well as with local employers on diabetes prevention and healthy eating programs — worthy but, often, not moneymakers for the hospital.
“You cannot take for granted that your hospital is as committed to your community as you are,” said Fort Scott City Manager Dave Martin. “We were naive.”

Mercy Hospital in Fort Scott, Kan., flew its flags at half-staff in December in honor of former President George H.W. Bush, who died Nov. 30.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
Indeed, in 2002 when Mercy decided to build a new hospital, residents raised $1 million for construction. Another $1 million was given by residents to the hospital’s foundation for upgrading and replacing the hospital’s equipment.
“Nobody donated to Mercy just for it to be Mercy’s,” said Bill Brittain, a former city and county commissioner. The point was to have a hospital for Fort Scott, county seat of Bourbon Country.
But today Mercy is a major health care conglomerate, with more than 40 acute care and specialty hospitals, as well as 900 physician practices and outpatient facilities. Fort Scott’s hospital is the second one in Kansas that Mercy has closed.
The hospital’s steady decline in patients, rising expenses and insufficient reimbursement “created an unsustainable situation for the ministry,” said Tom Mathews, vice president of finance for Mercy’s southwestern Missouri and Kansas region.

Visitors to Mercy’s Fort Scott hospital would pass a tall white cross as they drove down a winding driveway before arriving at the front door. Sisters of Mercy nuns founded the hospital in 1886, and the newest building, constructed in 2002, honors that Roman Catholic faith.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
But Fort Scott is a place that needs health care: One in 4 children in Bourbon County lives in poverty. People die much younger here than the rest of the state and rates for teen births, adult smoking, unemployment and violent crime are all higher in Bourbon County than the state average, according to data collected by the Kansas Health Institute and the Robert Wood Johnson Foundation.
Ten percent of Bourbon County’s more than 14,000 residents, about half of whom live in Fort Scott, lack health insurance. Kansas is one of 14 states that have not expanded Medicaid under the Affordable Care Act and, while many factors contribute to rural hospital closures, the GAO report found states that had expanded Medicaid had fewer of them.
The GAO report also found that residents of rural areas generally have lower household incomes than their counterparts in bigger cities, and are more likely to have chronic health conditions – such as high blood pressure, diabetes or obesity – that affect their daily activities.
The county’s premature birth rate is also higher than the 9.9% nationwide, a number that worries Dr. Katrina Burke, a local family care doctor who also delivers babies. “Some of my patients don’t have cars,” she said, “or they have one car and their husband or boyfriend is out working with the car.”
By nearly any social and economic measure, southeastern Kansas is “arguably the most troubled part of the entire state,” said Dr. Gianfranco Pezzino, senior fellow at the Kansas Health Institute. While the health needs are great, it’s not clear how to pay for them.
Health care’s ‘very startling’ evolution
Reta Baker described the farm she grew up on, south of town, as “a little wide place in the road.” She applied to the Mercy school of nursing in 1974, left after getting married and came back in 1981 to take a job as staff nurse at the hospital. She has “been here ever since,” 37 years — the past decade as the hospital president.
It has been “very startling” to watch the way health care has evolved, Baker said. Patients once stayed in the hospital for weeks after surgery and now, she said, “they come in and they have their gallbladder out and go home the same day.”
With that, payments and reimbursement practices from government and health insurers changed too, valuing procedures rather than time spent in the hospital. Rural hospitals nationwide have struggled under that formula, the GAO report found.

Dr. Katrina Burke checked Randall Phillips during an exam at Mercy Hospital in Fort Scott, Kan., in December. “Up in the city, a lot of doctors don’t do everything like we do,” Burke said of the variety of patients she sees as a family practice doctor who also delivers babies.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
Acknowledging the challenge, the federal government established some programs to help hospitals that serve poorer populations survive. Through a program called 340B, some hospitals get reduced prices on expensive drugs.
Rural hospitals that qualified for a “critical access” designation because of their remote locations got higher payments for some long stays. About 3,000 hospitals nationwide get federal “disproportionate share payments” to reflect the fact that their patients tend to have poor or no insurance.
Fort Scott took part in the 340B discount drug program as well as the disproportionate share payments. But, though Baker tried, it couldn’t gain critical access status.
When Medicare reimbursement dropped 2% because of sequestration after the Budget Control Act of 2011, it proved traumatic, since the federal insurer was a major source of income and, for many rural hospitals, the best payer.
Then, in 2013, when the federal government began financially penalizing most hospitals for having too many patients returning within 30 days, hospitals like Fort Scott’s lost thousands of dollars in one year. It contributed to Fort Scott’s “financial fall,” Baker said.
Baker did her best to set things right. To reduce the number of bounce-back admissions, patients would get a call from the physician’s office within 72 hours of their hospital stay to schedule an office visit within two weeks. “We worked really, really hard,” Baker said. Five years ago, the number of patients returning to Fort Scott’s hospital was 21%; in 2018 it was 5.5%.
Meanwhile, patients were also choosing to go to Ascension Via Christi in Pittsburg, Kan., because it offered cardiology and orthopedic services, Baker said. Patients also frequently drove 90 miles north to the Kansas City area for specialty care and the children’s hospital.

An empty operating room at Mercy’s closed Fort Scott hospital.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
“Anybody who is having a big surgery done, a bowel resection or a mastectomy, they want to go where people do it all the time,” Baker said. Mercy’s Fort Scott hospital had no cardiologists and only two surgeons doing less complicated procedures, such as hernia repair or removing an appendix.
Last year, only 13% of the people in Bourbon County and the surrounding area who needed hospital care chose to stay in Fort Scott, according to industry data shared by Baker.
There were no patients in the hospital’s beds during one weekend in December, Baker said. “I look at the report every day,” she said. “It bounces between zero and seven.” The hospital employed 500 to 600 people a decade ago, but by the time closure was announced fewer than 300 were left.
That logic — and the financial need — for closing didn’t sit well with residents, and Mercy executives knew it. They knew in June they would be closing Fort Scott but waited until October to announce it to the staff and the city. City Manager Martin responded by quickly assembling a health task force the day of the announcement in October, insisting it was “critical” to send the right message about the closure.
Fort Scott, Kan., City Manager Dave Martin stands in the middle of the city’s historical main street. “We really thought that we had a relationship,” says Martin, who is angry about Mercy’s decision to close the hospital.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
Relations between Mercy and the city grew so tense that officials needed attorneys just to talk to Mercy. In all, Fort Scott had spent more than $7,500 on Mercy Closure Project legal fees by the end of 2018, according to city records.
Will Fort Scott sink without Mercy?
When Darlene Doherty graduated from Fort Scott High School in 1962, there were two things to do in town: “Work at Mercy or work at Western Insurance.” The insurance company was sold in the 1980s, and the employer disappeared, along with nearly a thousand jobs.
Yet, even as the community’s population slowly declined, Martin and other community leaders have kept Fort Scott vibrant. There’s the new Smallville CrossFit studio, which Martin attends; a new microbrewery; two new gas stations; a Sleep Inn hotel, an assisted living center; and a Dairy Queen franchise. And the McDonald’s that opened in 2012 just completed renovation.
The town’s largest employer, Peerless Architectural Windows and Doors, which provides about 400 jobs, bought 25 more acres and plans to expand. There’s state state money promised to expand local highways, and Fort Scott has applied for federal grants to expand its airport.
Baker and some of the physicians on the Mercy hospital staff have been busy trying to ensure that essential health care services survive, too.
Baker found buyers for the hospital’s hospice, home health services and primary care clinics so they could continue operating.
Burke, the family doctor, signed on to be part of the Community Health Center of Southeast Kansas, a federally qualified nonprofit that is taking over four health clinics operated by Mercy Fort Scott. She will have to deliver babies in Pittsburg, nearly 30 miles away on a mostly two-lane highway that is under construction to widen it.

Unused hospital equipment is stored for shipment to other hospitals in the Mercy health system.
Christopher Smith for Kaiser Health News
hide caption
toggle caption
Christopher Smith for Kaiser Health News
Burke said her practice is full, and she wants her patients to be taken care of: “If we don’t do it, who’s going to?”
Mercy hospital donated its ambulances and transferred emergency medical staff to the county and city.
And, in a tense, last-minute save, Baker negotiated a two-year deal with Ascension Via Christi hospital in Pittsburg to operate the Fort Scott hospital’s emergency department — which was closed for two weeks in February before reopening under the new management.
But Baker knows that too may be just a patch. If no buyer is found, the facility will close by 2021.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
States Sue Drugmakers Over Alleged Generic Price-Fixing Scheme

Jose A. Bernat Bacete/Getty Images
Connecticut Attorney General William Tong has a skin condition called rosacea, and he says he takes the antibiotic doxycycline once a day for it.
In 2013, the average market price of doxycycline rose from $20 to $1,829 a year later. That’s an increase of over 8,000%.
Tong alleges in a new lawsuit that this kind of price jump is part of an industry-wide conspiracy to fix prices.
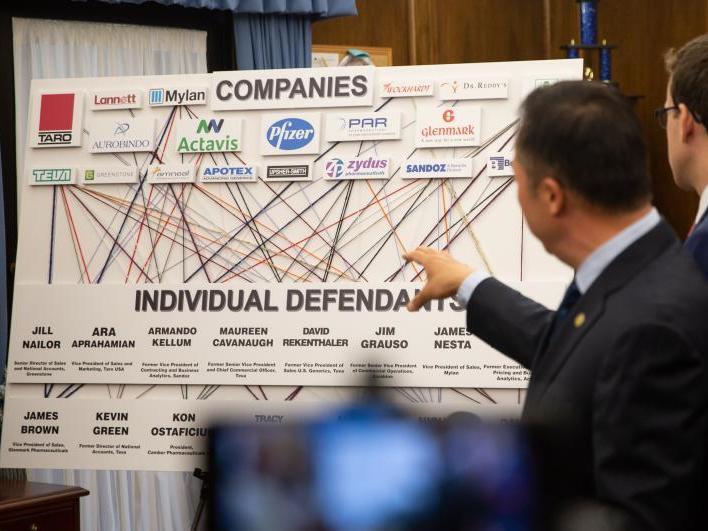
The suit is a whopper — at least 43 states are suing 20 companies and the document is over 500 pages long. It was filed Friday in the U.S. District Court in Connecticut.
The lawsuit alleges that sometimes one company would decide to raise prices on a particular drug, and other companies would follow suit. Other times, companies would agree to divide up the market, rather than competing for market share by lowering prices.
It says these kind of activities have been happening for years, and that companies would avoid creating evidence by making these agreements on golf outings or during “girls nights outs” or over text message.
In several examples, the suit cites call logs between executives at different companies, showing a flurry of phone calls right before several companies would all raise prices in lockstep.
All of this, according to the lawsuit, resulted “in many billions of dollars of harm to the national economy.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Connecticut Attorney General William Tong says the generic drug industry is profiting “in a highly illegal way” from Americans. Tong is at the forefront of a multi-state lawsuit filed May 10, which alleges companies worked together to set prices.
Frankie Grazian/Connecticut Public Radio
hide caption
toggle caption
Frankie Grazian/Connecticut Public Radio
Consumers don’t always notice when a generic drug’s price increases rapidly. People without insurance, of course, pay full price, but even people with insurance can feel the impact.
“More people than ever before are paying based on the price of the drugs,” explains Stacie Dusetzina, a professor at Vanderbilt University who studies drug pricing. Often, patients have to meet a deductible before their health plan’s coverage kicks in, so “they pay full price until they reach a certain level of spending, or they pay a percentage of the drug’s price — we call that a coinsurance.”
Surveys show more Americans are having trouble paying out-of-pocket medical costs. The average annual deductible in job-based health plans has quadrupled in the past 12 years and now averages $1,300.
But, Dusetzina says, even if you only pay a modest copay — such as $5 for every prescription you pick up — if your insurance company is paying more for prescription drugs, it can raise your health plan’s premiums the following year. “So ultimately these costs do get borne by the consumer in some way,” she says.
Dusetzina says what this lawsuit alleges is “very disappointing” — a situation in which consumers put up with the high price of branded drugs because of the implicit promise that a generic is coming some day and will eventually bring the price down.
But that outcome doesn’t happen automatically — it relies on healthy competition and market forces to work. If there’s only one generic version available, that drugmaker can set the price at pretty much the same level as the brand name.
“The higher the number of competitors, the more we see price reductions from the branded drug price,” she says. “So the magic number seems to be around four manufacturers.”
And that assumes those drugmakers aren’t talking to each other and agreeing to coordinate rather than compete.
The main drugmaker cited in the lawsuit is Teva, an Israeli company. In a statement, Kelley Dougherty, Vice President of Communications and Brand, Teva North America told NPR that the company is reviewing the allegations internally and that Teva “has not engaged in any conduct that would lead to civil or criminal liability.”
The company has also asserted that there’s nothing new here, and it’s true that the new lawsuit is similar to past lawsuits, though none of them included so many states as plaintiffs.
Connecticut Attorney General William Tong has emphasized that the investigation is ongoing, and given the amount of political appetite there is to bring drug prices down, there are certainly more lawsuits to come.
Transplants A Cheaper, Better Option For Undocumented Immigrants With Kidney Failure

{kind=link}
In most states, undocumented immigrants with kidney failure have to receive dialysis as an emergency treatment in hospital emergency rooms. Some advocates say kidney transplants for undocumented immigrants would be a cheaper way to treat the problem.
JazzIRT/Getty Images
hide caption
toggle caption
JazzIRT/Getty Images
Uninsured, undocumented immigrants often go to the emergency room for treatment. Since 1986 the federal government has required that patients in the emergency room receive care, regardless of their immigration status or ability to pay.
But caring for chronic conditions such as kidney disease or cancer in the emergency room is expensive. So some states are quietly expanding access for undocumented immigrants to obtain medical treatment beyond the ER.
One of those states is Washington, where an undocumented immigrant named Gonzalo lives with his wife, Ricarda.
Gonzalo is really sick.
“I can’t enjoy the day — go out — because I’m always unwell,” he said in an interview in Spanish.
Gonzalo moved to the U.S. from Mexico about 30 years ago. He’s 60 years old. We’re not using his last name because of his immigration status.
Ten years ago, Gonzalo’s kidneys failed. Since then, he’s gotten sicker and sicker. Five years ago, he had to quit his job as a painter.
“I used to pay the rent. I paid for everything, and we didn’t lack anything,” he said. “But I got sick and everything changed.”
Now, Gonzalo and his wife live with one of their daughters in her apartment south of Seattle.
Across the country, there are about 6,500 undocumented immigrants with kidney failure, according to the National Institutes of Health. What kind of care they get depends on where they live.
In most states, they can only get dialysis in hospital emergency rooms.
That means, every couple of weeks, they go to the hospital when so many toxins have built up in their body it’s life-threatening. Usually, they have to stay overnight so they can be dialyzed twice. That costs nearly $300,000 per person every year.
So seven states, including Washington, have a different system.
“The state of Washington has something called AEM,” said Leah Haseley, a nephrologist — a kidney doctor — in Seattle. She’s talking about Alien Emergency Medical, part of Washington’s Medicaid.
“AEM pays for two things,” she explained. “They pay for dialysis for undocumented people, and they pay for chemotherapy for cancer treatment for undocumented people as well.”
Regular dialysis costs about a quarter of what emergency dialysis does — but it’s controversial.
“The first time that you show up at a hospital with kidney failure, that’s an emergency,” said Matthew O’Brien, with the Federation for American Immigration Reform, a group that advocates for stricter immigration laws. “After that, it’s a chronic condition, and we don’t believe that it’s appropriate to reward lawbreakers with benefits at the expense of U.S. taxpayers.”
But there are others who say even regularly scheduled dialysis isn’t enough: undocumented immigrants who qualify should be given kidney transplants, because the cost of a transplant is less than the ongoing costs of regular or emergency dialysis. But, without health insurance, few undocumented immigrants can afford a transplant.
In 2015, Illinois became the first state with a system for paying for organ transplants for undocumented immigrants.
Dr. David Ansell was a prominent advocate for the change.
“In about a year and a half the cost for a transplant pays itself back,” he said, “but also people can go back to work and contribute to the state.”
So far, more than 200 undocumented immigrants in Illinois have been given access to organ transplants, with their insurance premiums paid for by a non-profit. Now, Dr. Ansell and other public health advocates hope to see a similar program at the national level.
Many who oppose this say, with limited organs available, they should be reserved for citizens and legal immigrants.
But Dr. Ansell says, in Illinois, 75 percent of kidney transplants for undocumented immigrants come from donations from their own family — a much higher rate than the rest of the population.
“If you’re undocumented in Illinois, you can get a driver’s license, and disproportionately the Latino community is signing up to donate their organs,” Dr. Ansell added. “It’s a simple matter of ethics and fairness.”
He said, since Illinois started paying for the transplants, the total number of organs available has increased, because so many more Latinos have signed up for organ donation.
Overall in the US, studies have found that undocumented immigrants donate 2 to 3% of all organs.
Back in the Seattle area, Gonzalo says all three of his daughters are willing to give him a kidney, but he has no way to pay for the transplant.
That’s why his wife, Ricarda, says she’s taken to buying lottery tickets.
She said in Spanish, “I’ve told my husband, ‘If I win the lottery, I won’t think twice. I’m going to get you a kidney.'”
Not My Job: We Quiz Baseball Great Ozzie Smith On ‘The Wizard Of Oz’

{kind=link}
St. Louis Cardinals shortstop Ozzie Smith waves to fans on Sept. 13, 1996.
Michael Caulfield/AP
hide caption
toggle caption
Michael Caulfield/AP
We recorded the show in St. Louis this week and invited former Cardinals shortstop Ozzie Smith to play our quiz. We’ll ask the Baseball Hall of Famer, known as “The Wizard” for his magical plays, to answer three questions about the 1939 movie The Wizard of Oz.
(SOUNDBITE OF MUSIC)
BILL KURTIS: From NPR and WBEZ Chicago, this is WAIT WAIT… DON’T TELL ME, the NPR news quiz.
(APPLAUSE)
KURTIS: I’m Bill Kurtis. We’re playing this week with Tom Bodett, Amy Dickinson and Brian Babylon. And here again is your host at the Fox Theatre in St. Louis, Mo…
(CHEERING)
KURTIS: …Peter Sagal.
PETER SAGAL, HOST:
Thank you, Bill. Hey, thanks, everybody. And listen, if you are just tuning in, and you’re like, oh, no, I missed it, or maybe you just want to hear it all again so you can pretend you haven’t and impress your friends by knowing all the answers, all you need to do is download the WAIT WAIT podcast. It’s the same show you love on the radio but with ads for mattress companies and stamps.
(LAUGHTER)
SAGAL: Right now, it is time to play the WAIT WAIT… DON’T TELL ME Bluff the Listener game. Call 1-888-WAIT-WAIT to play our games on the air. Hi, you are on WAIT WAIT… DON’T TELL ME.
EBEN ATWATER: Hi. I’m Eben Atwater. I’m from Lummi Bay, Wash.
SAGAL: Eben from Lummi Bay, Wash.
ATWATER: Well, the – I think they had a girl’s name figured out but not a guy’s name figured out, and I got stuck with the family name.
SAGAL: Do you know what the girl’s name was?
AMY DICKINSON: (Laughter).
ATWATER: Yeah, it was Emily.
SAGAL: Let me ask you a question – given what you’ve been through, would you have preferred to be named Emily?
(LAUGHTER)
ATWATER: I’d roll with it.
SAGAL: All right. You could go with it. Well, welcome to the show, Eben. You are here to play our game in which you must try to tell truth from fiction. Bill, what’s Eben’s topic?
KURTIS: I’m your biggest fan.
SAGAL: Celebrities have long found fans the traditional ways, like press tours and purchasing Twitter followers from a Chinese bot farm. But this week, we heard about a new way that a fan found the person or people they’re fans of. Our panelists are going to tell you about it. Pick the one who’s telling the truth – you’ll win the WAIT WAITer of your choice on your voicemail. You ready to play?
ATWATER: Let’s do it.
SAGAL: All right. First, let’s hear from Tom Bodett.
TOM BODETT: The lyrics to “A Horse With No Name” blew my mind, said Blollapalooza organizer Mason Ford (ph). Ford, who is 16 years old, discovered early ’70s soft rock bands like America and Bread when his dad erased his Spotify playlist of hip-hop favorites and replaced it with what he thought would be the genre from hell. I couldn’t stand the F words and (unintelligible) emanating from his room and earbuds another day, said the elder Ford. I wanted to punish him with some “Diamond Girl” and “Muskrat Love.”
(LAUGHTER)
BODETT: I thought he needed to understand what obnoxious feels like. Instead, he loves it. What I realized, explained Ford the younger, is that hip-hop is not chill music. All me and my friends want to do is chill and hang out. This weird sound is so chill, it almost doesn’t make sense. I mean, baby, Imma (ph) want you?
DICKINSON: (Laughter).
BODETT: Who says that?
(LAUGHTER)
BODETT: And with that googly sounding guitar thing in the background, it’s sick. I love it. After two or three songs, you can’t move.
(LAUGHTER)
BODETT: The Blollapalooza will be no Fyre Fest, promises Ford, referring to the famous concert fail of last summer. It’s more of a warming drawer fest. Surviving members of America, along with Dan Fogelberg, will headline the event to be held this August in a closed Walmart parking lot in Springfield, Iowa. Father Ford will not be attending. I lived through the ’70s once, he said. A day of this might kill me.
(LAUGHTER)
SAGAL: A young man…
(APPLAUSE)
SAGAL: …Becomes a fan of ’70s soft rock through a cruel prank from his father. Your next story of a celeb making new fans comes from Brian Babylon.
BRIAN BABYLON: UPenn volleyball player Elizabeth Watty (ph) was running late for practice in Philly. The pressure was on because she had to park her 1964 Pontiac GTO – a hand-me-down from her grandpa – into a parking space barely big enough for an enormous land yacht. I hate this car, said Watty. As soon as I land my pro beach volleyball contract, I’m buying myself a Honda Fit. She tried eight times, each time scraping or bumping the car in front of her and going up on the curb. With drivers behind her honking their horns and complaining, finally, she was ready to give up and keep driving. But then, a gentleman appeared in her window and said, may I assist? She was very angry about this implied sexism but got out and let him in.
(LAUGHTER)
BABYLON: And the most amazing display of driving happened. He hopped in. And in the most amazing display of driving she had ever seen, he whipped that 20 feet of Detroit steel into a parking space with just a few turns of the wheel. She wrote his name down to send him a nice thank-you note. And then when she showed the name to her teammate, the teammate said, Jimmie Johnson, the NASCAR driver.
(LAUGHTER)
BABYLON: No, said Elizabeth. I think he had a Toyota car of some kind. But it was No. 48 himself, seven-time NASCAR champion, who was in town for a personal appearance. Elizabeth, of course, had to watch him race and instantly became a fan. He’s just so confident, so tactical on the track, she says.
(LAUGHTER)
BABYLON: And if you think he’s good at racing, you should see him park.
(APPLAUSE)
SAGAL: A NASCAR fan is made when Jimmie Johnson, himself, steps in to park her car. Your last story of a famous person convincing someone to like them comes from Amy Dickinson.
DICKINSON: When they heard that Lyle Lovett, their favorite singer, was coming to Austin, 17 women from three generations of one big Texas family decided to call it a Girls Gone Wild Weekend. The Lovett love is mighty strong in the Walker clan. So Belinda from El Paso rallied her gal pals from all over the country – sisters, cousins, her mother and even her 85-year-old grandmother – and told them (imitating Southern accent) pack up your spangly cowboy boots and send Bota Boxes of chardonnay, ladies, because we’re going to see Lyle Lovett. Whoo (ph).
(CHEERING)
DICKINSON: The concert tickets got bought. The event was coming up when Walker sister figured out that the Lovett coming to Austin was not the Texas native and rectangle-faced, Grammy Award-winning singer Lyle Lovett. No, this Lovett was Jon Ira Lovett of Connecticut, a former Obama speechwriter, bringing his…
(LAUGHTER)
DICKINSON: …Popular progressive politics podcast “Lovett Or Leave It” to Austin for a live taping.
(LAUGHTER)
DICKINSON: The Lyle Lovett-loving ladies decided to go ahead with their Girls Gone Wild Weekend.
(LAUGHTER)
DICKINSON: It turns out having to watch a politics lecture from a guy who can’t sing and was never even briefly married to Julia Roberts…
(LAUGHTER)
DICKINSON: …Was just about right for these girls gone mild.
(LAUGHTER)
SAGAL: All right, so here are your choices. Somebody made a fan in an unusual way. Was it from Tom Bodett – ’70s soft rockers get a fan when a kid is punked by his own father who switched his playlist? Was it from Brian Babylon – Jimmie Johnson created one new NASCAR fan when he graciously parked her car for her? Or from Amy Dickinson – the political pundit and podcaster Jon Lovett got a whole bunch of Texas women to come see him because they thought he was Lyle Lovett. Which of these is the real story of an unexpected meeting of fan and idol in the news?
ATWATER: (Imitating Southern accent) Well, I’ll tell you what…
(LAUGHTER)
ATWATER: …I lived for 12 years in Texas, and there ain’t no way on God’s green Earth I’m picking any other story but that one.
DICKINSON: Oh.
SAGAL: You’re going to pick, then, Amy’s story…
(LAUGHTER)
SAGAL: …Of the 17 women who went to see Lyle Lovett and ended up hearing some interesting political comedy from Jon Lovett.
ATWATER: Got to be it.
SAGAL: All right. Well, we actually spoke to one of the fans in question.
BELINDA WALKER: One of my cousin’s looked, and it said Jon Lovett. And my sister’s like, no, no, no, I got Lyle Lovett tickets. And we’re like, oh, my God, it is the wrong one. What are we going to do? What are we going to do?
(APPLAUSE)
SAGAL: That was Belinda Walker. Practically an entire female side of the family went to see Lyle Lovett and got Jon instead. It’s OK. They like him. Congratulations. You got it right, Eben. You have won our prize by picking Amy’s story.
(CHEERING)
SAGAL: And you’ve won a prize for her. Well done, sir.
ATWATER: Hey, thanks a lot. That was great.
SAGAL: Bye-bye.
(SOUNDBITE OF MUSIC)
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Cuban Diva Omara Portuondo Feels As Strong As Ever On ‘Last Kiss’ World Tour

{kind=link}
Omara Portuondo may be on her “Last Kiss” Tour, but the Cuban music matriarch says she plans to keep performing for as long as possible.
Johann Sauty/Courtesy of the artist
hide caption
toggle caption
Johann Sauty/Courtesy of the artist
In 1996, Omara Portuondo was working on an album at Havana’s famous recording studio, Egrem. Upstairs, American musician Ry Cooder was laying down tracks for Buena Vista Social Club, a project with veteran Cuban musicians like Compay Segundo. Portuondo was invited to come up and sing a duet with him. They sang “Veinte Anos,” a song Portuondo learned as a child.
“Without rehearsal, this was a live recording. One take. It’s unbelievable,” says Cuban bandleader Juan de Marcos Gonzalez. He had scouted and rediscovered the older musicians for Buena Vista Social Club. But he says Portuondo was still a star on the island, and bringing her into the project was a dream.
“I remember that once, Mr. Ry Cooder told me, ‘Omara is the Cuban Sarah Vaughan.’ And I said to him, ‘No, Sarah Vaughan was the American Omara Portuondo,'” Gonzalez says.
NPR met up with the legend herself at a downtown Los Angeles hotel the day she began her latest world tour, deemed “The Last Kiss.” Now 88 years old, Portunodo sometimes sings answers to questions about her long career.
“Por eso, yo soy Cubana, y me muero siendo Cubana,” she sings: “I’m Cuban, and I’ll die Cuban.”
Portuondo’s first gig for her latest world tour was at LA’s Regent Theater. Even though she was sitting, she had the audience clapping, dancing and singing along.
“Omara is the most important singer of our culture,” Cuban pianist Roberto Fonseca, who performs with Portuondo on the tour, says. “She’s able to do any Afro-Cuban style, Latin jazz, jazz, boleros, traditional Cuban music, rumba. She’s magical, intense, pure, strong.The audience … the public … they are crying, smiling, dancing. All the time, she’s making jokes.”
“Yes, she’s flirting with the audience the whole time,” Alicia Adams, international program director for the John F. Kennedy Center for the Performing Arts in Washington, D.C. says. Adams brought Portuondo to the center’s Cuban Arts Festival last year, and recalls seeing the singer peak out from beneath the curtain to wave to her fans. Adams says as relations between Cuba and the U.S. have morphed over the decades, Portuondo has always been a cultural ambassador.
“She spans before the revolution and after the revolution,” Adams says. “From before, when there was much more ability to go back and forth, until later years, after the revolution, when things were not so easy in terms of that kind of travel.”
Unlike some other Cuban musicians — including her sister Haydee and her old friend, the late Celia Cruz — Portuondo chose not to defect to the U.S. She says she comes and goes from her home in Cuba as she likes, pretty much like her father, Bartolo Portuondo, did. He’d been a black professional infielder for both the Cuban League and the Negro Leagues in the U.S. Portuondo says that he was a great baseball player and that her mother, who was white, scandalized her upper-class family by marrying him.
When she was a little girl, Portuondo dreamed of being a ballet dancer. But she says in those days, you could only dance ballet if you were white. Instead, she and Haydee danced and sang at Havana’s famous Tropicana. Later, in 1945, the sisters formed a quartet with two other women, Elena Burke and Moraima Secada (the aunt of singer Jon Secada’s.) The Cuarteto D’Aida danced and sang in nightclubs and on television. The quartet even backed Nat King Cole when he performed in Havana.
Portuondo sang with the quartet for 15 years before launching a solo career in 1963. Since then, she’s sung with everyone from Pablo Milanes and Chucho Valdes to Los Van Van and reggaetoners Yomil Y el Dany. She even sang in the 2009 Spanish version of Disney’s The Princess and the Frog. For years, Portuondo was associated with Cuba’s movimiento filin — the feeling movement that celebrates singers who interpret lyrics with great emotion.
Portuondo remained a star in Cuba, but it was the Buena Vista Social Club that introduced her to an even bigger audience in the U.S. and around the world. Audiences wept for her duets with Ibrahim Ferrer, who Portuondo sang with in the 1950’s. He’d been long-forgotten until the Buena Vista Social Club. The group’s first album won a Grammy award in 1998. And an Oscar-nominated documentary by Wim Wenders chronicled the group’s journey from Cuba to an historic concert at Carnegie Hall.
Portuondo never stopped recording or performing. Gonzalez says for many years, Portuondo also sang with his band, the Afro-Cuban All Stars. As for this tour being her “last kiss”? Gonzalez says that’s just marketing ploy . “She’s going to die on the stage. That’s what she wants,” he says. “She’s the Cuban diva.”
And Portuondo agrees. “Despedida? No.” This is not goodbye, Portuondo says as she breaks into song: “Lo que me queda por vivir será en sonrisas“: “What I have left to live for is smiles,” she sings, adding “Me queda tiempo todavia,“: “I still have time.”
Which W: Walgreens Or Washington?

The logo for the Washington Nationals baseball team might look familiar even if you don’t follow the team. Especially if you shop at Walgreens.
SCOTT SIMON, HOST:
If you’ve been to Washington, D.C., you might’ve noticed people wearing what appears to be Walgreens hats. Well, not really. The city’s baseball team, the Washington Nationals, has a curly W logo that’s remarkably similar to the drugstore chain’s. And as Ally Schweitzer from member station WAMU discovered after a visit to Nationals Park, the trademark is still causing confusion 14 years after the team rolled it out.
UNIDENTIFIED PERSON: Ice cold water, $2.
ALLY SCHWEITZER, BYLINE: I’m outside the ballpark in D.C. asking game goers if they can distinguish between the Nationals logo and the Walgreens logo. I thought, if anyone could tell the difference, it would be Nationals fans. Turns out, I was wrong. I showed Northern Virginia resident Sean Barnett the logos side by side.
Can you tell what this is?
SEAN BARNETT: Washington Nationals.
SCHWEITZER: No.
BARNETT: No.
SCHWEITZER: That’s the Washington Nationals. What is this?
BARNETT: Oh, is that Walgreens?
SCHWEITZER: Yes.
BARNETT: Oh, very close.
SCHWEITZER: Most fans I spoke to correctly identified the logos, but Barnett was among several who did not. When my colleague Sasha-Ann Simons asked Washingtonian Rich Jensen which one was which, he was also stumped.
RICH JENSEN: I can tell that one is for Walgreens and one is for the Nationals, but I couldn’t tell you which is which.
SASHA-ANN SIMONS, BYLINE: And you say this as you’re wearing a Nationals cap on your head. I love this.
JENSEN: Yeah, well, can I take it off and look?
SIMONS: (Laughter).
JENSEN: No. No.
SIMONS: No, you can’t.
JENSEN: OK.
SCHWEITZER: The logo similarity has been a running joke among baseball fans ever since the team arrived in D.C. in 2005 and adopted the vintage W logo used by long-gone D.C. baseball team, the Washington Senators. Todd Radom knows this history well. He’s the guy who recast the Senators’ logo for Major League Baseball.
TODD RADOM: It is a remarkably similar curly W.
SCHWEITZER: Radom has designed thousands of sports logos during his career, but he says the one for the Nats is trickier than others out there.
RADOM: Boston Red Sox are two socks. The Philadelphia Eagles have an eagle. The word national really didn’t lend itself to easy identification.
SCHWEITZER: So the decision was made to go with a word or a letter. And the chosen letter was the Senators’ W, which happened to look a lot like the W Walgreens has used since at least the 1950s. And Walgreens never sued. That might seem surprising considering the drugstore chain filed a suit against grocer Wegmans over its W logo back in 2010. Wegmans later settled and stopped using the W. Neither Walgreens nor Major League Baseball agreed to comment for this story. So I turned to Ross Kimbarovsky. He’s a former intellectual property attorney. He said he’s not surprised Walgreens hasn’t gone after Major League Baseball for a trademark violation because Walgreens the corporation, he says, isn’t easily mistaken for a baseball team.
ROSS KIMBAROVSKY: It would be unfair at this point for them to be able to point a finger and say people are confused because what’s been happening over the many, many decades there hasn’t been any evidence of confusion.
SCHWEITZER: Kimbarovsky, who founded the logo company Crowdspring, says people probably aren’t walking into Nationals Park looking to refill prescriptions. So back outside the stadium, I asked self-identified D.C. native Tye Ali if he’s ever thought people would confuse the Nationals cap he’s currently wearing for a Walgreens cap.
TYE ALI: No. No, everybody knows this is a Nationals hat (laughter). But then I don’t know. It might be a Walgreens.
SCHWEITZER: It’s not.
ALI: (Laughter).
SCHWEITZER: For diehard fans in D.C., the Walgreens’ curly W and the Nationals’ curly W aren’t even in the same ballpark.
For NPR News, I’m Ally Schweitzer in Washington.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Saturday Sports: Red Sox At White House, NHL, NBA Playoffs
NPR’s Scott Simon and Howard Bryant of ESPN talk NBA and NHL playoffs, as well as discuss the politics of team celebrations at the White House.
SCOTT SIMON, HOST:
Abracadabra – sports.
(SOUNDBITE OF MUSIC)
SIMON: The world-champion Boston Red Sox visited the White House this week – well, half of them anyway – hockey down to its final four. And we’ve nearly reached the conference finals of the NBA playoffs. Howard Bryant of ESPN joins us. Howard, thanks for being with us.
HOWARD BRYANT, BYLINE: Good morning, Scott.
SIMON: One more week I guess I can say – if not more than one – fear the deer…
BRYANT: (Laughter).
SIMON: …Because the Milwaukee Bucks are already in the Eastern Conference finals after sweeping the Celtics under the rugs. Golden State finished off Houston last night for the – what? – fourth time in five years. And now, of course, two Game 7s scheduled for Sunday. What are we seeing that surprised you?
BRYANT: Well, the thing that surprised you is – more than anything else is the Boston Celtics come out, and they beat Milwaukee by 20 in Game 1 and then lose four straight. Milwaukee’s a great team. It’s going to be fun to see what they do. Yeah. I really think that Warriors-Bucks would be an amazing final, considering that they were the two best teams in the league this year. Of course, what Golden State did last night is incredible. You have Kevin Durant go out in Game 5. He gets hurt. You’re expecting Houston to at least get this game at home, bring it back to a Game 7. And then, of course, let’s not forget. You still have Steph Curry, two-time MVP. You have Klay Thompson, one of the greatest shooters who ever played the game.
SIMON: Yeah.
BRYANT: Steph Curry has no points and three fouls at halftime and ends up going for 33 in the second half. And it was just a demoralizing defeat for the Houston Rockets. But once again, this is a championship-level team. This is one of the – one of those teams, like the Bruce Bochy Giants or the Red Sox in the 2000s or the Joe Torre Yankees. You know, don’t – you can’t kill them. You have to actually beat them. You leave the door open. And they’re going to come back and do what they did last night – incredible, incredible performance.
SIMON: James Harden is so great. Houston is so great. They can’t beat the Warriors. Who can? Can the Bucks?
BRYANT: Yeah. I think the Bucks can. I think that it’s a believe-it-when-I-see-it thing for me, watching the Warriors. But there were moments where a tougher team could have beaten them. But once again, this is – it was like watching the Patriots in the Super Bowl where you’re looking at them going OK. This is the year where they die. This is the year where you beat them. This is the year. And then their championship players come up with performances. You have to – you know, this is what separates them. This is why we watch these guys. This is why some of these players are so special. They’ve got it. The other guys don’t when – you know, when the moments are on the line.
SIMON: Interesting storylines in the NHL. So you have the St. Louis Blues and the San Jose Sharks. And then the Bruins play the Carolina Hurricanes. Who do you see in the finals?
BRYANT: Well, I kind of like San Jose and Boston simply because I like the storyline of Joe Thornton – overall, you know, No. 1 pick for the Bruins, drafted by the Bruins, expected to be the next great Bruin, ends up going to San Jose. And to have him end his career playing for a championship against his former team is pretty good. Carolina’s a good team. And, you know, they blew Game 1 against the Bruins. They had it. And they…
SIMON: Yeah.
BRYANT: They played a really bad third period. St. Louis really, really tough team – I think that it wouldn’t be surprising any of the combinations. But I kind of like Boston and San Jose.
SIMON: About half the Boston Red Sox visited the White House this week. What did we learn from the half that went and the half that didn’t?
BRYANT: Well, I think what we learned, one, is that, you know, it’s the same sort of combination that you have across the country. You know, the half – you know, the white players went. The players of color didn’t go. The manager Alex Cora didn’t go. I think that…
SIMON: Saying specifically it was…
BRYANT: Specifically.
SIMON: …His dissatisfaction with administration policy in Puerto Rico.
BRYANT: Absolutely. And I think that David Price and Mookie Betts, the reigning MVP, said similar comments about not wanting to go. I think that the Boston Red Sox made a terrible mistake. I think they made a horrible mistake in terms of leadership by saying that there’s no racial divide on the team. Clearly, there is. There’s a racial divide in the country. And I think that people keep saying we want dialogue. We want dialogue. You had an opportunity for a dialogue here.
I don’t blame the white players for going to the White House. I don’t blame anybody for going to the White House in terms of the – how many citizens get to go to the White House by invitation? So I understand that. But I also understand that you cannot avoid what’s taken place in the country. And I think the Red Sox blew it, to be honest.
SIMON: Howard Bryant of ESPN, thanks so much for being with us. Talk to you soon.
BRYANT: Thank you.
(SOUNDBITE OF TRAVIS SCOTT SONG, “GOOSEBUMPS”)
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
3-Pointer NBA Teams Change The Game
NBA teams like the Warriors and the Rockets have made three-pointers the center of their game, forcing other teams to adapt. NPR’s Ailsa Chang discusses this shift in play with sports and culture writer Zach Kram.
Mexico’s Star Race Walker Lupita González Hit With 4-Year Ban For Doping

{kind=link}
María Guadalupe González, seen here winning the Women’s 20 km race at the IAAF World Race Walking Team Championships last May, has been banned from the sport for four years.
Yifan Ding/Getty Images for IAAF
hide caption
toggle caption
Yifan Ding/Getty Images for IAAF
An athletics tribunal has banned elite Mexican race walker María Guadalupe González from competing for four years. Officials allege that González, popularly known as Lupita, forged records to bolster her claim that she ate meat containing a metabolite of trenbolone, a powerful anabolic steroid.
González, 30, has won numerous titles, including a silver medal at the Rio Summer Olympics in 2016. She had been training recently with the intent of competing at next year’s Tokyo Games. But her chances of racing in Japan are now dashed, unless she files and wins an appeal.
The Athletics Integrity Unit, which handles integrity issues for the International Athletics Federation (IAAF), says González’s ban effectively started on Nov. 16, 2018. That’s the day the AIU provisionally suspended the athlete because she failed an out-of-competition drug test administered in Mexico City.
The doping allegations have sent deep ripples through Mexico’s community of Olympic athletes.
In early December, days after González was told her “B” urine sample had also failed doping tests, Mexican athletes voiced their support for her, representing sports from boxing and fencing to diving. And last month, the head of Mexico’s Olympic Committee said he wants González to focus on training at altitude for the Tokyo Olympics rather than worry about overturning her suspension in time for this summer’s Pan American Games.
In her defense against the doping allegation, González said she had not used any prohibited substances, and that if trenbolone was in her system, it must have come from meat she ate in the two days before the urine test. She added that the steroid is legal to use on livestock in Mexico. And she later claimed she had also been diagnosed with anemia and instructed to eat more meat.
In its response, the IAAF said the race walker’s explanation “is not sufficient on the balance of probability,” and that the concentration of trenbolone found in her sample was too high to have come from contaminated meat.
Officials also engaged a company called Pentad Security to look into González’s claims, including a hospital report she submitted as evidence of her anemia condition.
From the ruling:
“The Pentad Report considers the hospital report submitted by the Athlete to have been forged if one takes into account the incorrect data included in the report, such as the doctor’s name or telephone number, and the fact that ‘diagnosis of ferropenic microcytic hypochromic anaemia is not supported by the [Hospital Report] and is not compatible with the hematological values in the [ABP],’ as concluded by Professor D’Onofrio.” [referring to professor Giuseppe D’Onofrio, an IAAF expert witness]
The IAAF also said food receipts from restaurant and food trucks provided by González had also been fabricated. And it said that while González had initially described eating steak and pork, she later said she had also eaten liver.
“As the maximum permitted residues of trenbolone is five times higher in liver, she had an interest in having eaten liver,” the panel said in its ruling.
While it’s retroactive to last fall, the doping ban does not strip González of any medals or titles she won prior to last year’s failed test.
Opinion: Keep Limits Intact On Medical Residents’ Work Hours

{kind=link}
Just as sleep deprivation has been shown to impair cognition, so too has it been found to dampen empathy for others.
Johner Images/Getty Images
hide caption
toggle caption
Johner Images/Getty Images
Imagine yourself stuck in the hospital.
Would you rather your doctors be well-rested, with a limit on how many hours they can work? Or would you rather they work longer shifts, seeing you through the critical hours of your illness and with fewer handoffs of your care?
That’s the choice being reexamined after a study published in March in the The New England Journal of Medicine found that longer shifts for medical residents were just as safe as shorter shifts.
The results, which support an earlier study that also found no association between shift length and patient safety, have led some physicians to suggest that the issue of how long residents should work has now been “laid to rest.”
University of Pennsylvania’s Dr. David Asch, one of the study’s lead investigators, said in a statement that despite concern about lengthy shifts for residents, “they really don’t seem to have an effect on any important domains.”
Sixty-three internal medicine residency programs participated in the latest study. Half of the programs adhered to limits on how long residents could work. First-year residents were restricted to 16-hour shifts, while more senior residents could work up to 28 hours. For the other half, there was no limit on how long residents could work.
The researchers focused on patients’ mortality rates. They found that the number of patients who died within 30 days of admission to the hospital was similar between the two groups. Though the study didn’t examine medical errors directly, the implication is that the rate of medical error was also similar.
The findings are reassuring, given what we know about the effects of sleep deprivation on cognitive performance. Some studies have found that sleep deprivation can lead to a similar level of impairment as heavy drinking.
Concerns about exhausted physicians in training have been around since at least 1984, when a college freshman named Libby Zion died in a New York hospital from an error made by a sleep-deprived resident. After a high-profile investigation, New York state instituted the first limits on how long physicians in training could work — no more than 24 hours in a shift, and no more than 80 hours in a week. These limits were extended to all residency programs in 2003 and strengthened in 2011.
It seemed like a prudent change. As many have argued, we don’t let our pilots fly without adequate rest.
But some physicians challenged the limits, pointing out that we had no direct evidence to support the change. It had simply never been studied.
Shift limits could have unintended consequences. For example, shorter shifts mean more handoffs between physicians, during which important information can sometimes be lost.
Does the latest study mean that strict limits on shift length should be rolled back, since they’ve not been proven to help patients? Or is there more to the story than medical errors and patient safety?
Just as sleep deprivation has been shown to impair cognition, so too has it been found to dampen empathy for others.
Studies show that a single night of sleep deprivation interferes with our ability to perceive emotions in others and compromises our ability to empathize. Longer periods of sleep deprivation reduce measures of emotional intelligence and interpersonal functioning.
One of the darkest moments of my medical training came at the end of a 28-hour call in the ICU. Firefighters had rescued a woman from a house fire, badly burned and barely alive. She was at the threshold of death when she arrived. Her suffering must have been unbearable, but I’m ashamed to say that all I could think about was how long her death paperwork would keep me awake.
I don’t think I’m alone in finding that sleep deprivation warps my ability to provide compassionate care. In 2002, researchers at the University of Pennsylvania surveyed residents before and after their first year of training. The prevalence of chronic sleep deprivation soared from 9% to 43%. Emotional exhaustion rose from 8.5% to 68%, and measures of empathy dropped 10%-15%.
We can’t say how these changes affected patients, but it’s no stretch to imagine that they were probably harmful to the patient-physician relationship. They were certainly harmful to the residents — the prevalence of depression increased from 4.3% to nearly 30% by year’s end, and burnout leaped from 4% to 55%.
Skeptics about shift limits may point out that both groups in The New England Journal of Medicine study got a similar amount of sleep, when averaged over time. But participants in the group without shift limits were nearly 2.5 times more likely to be dissatisfied with their amount of time for rest and with their overall well-being. They were also more likely to report that patient safety and the quality of their education had suffered as a result of the longer hours.
In 2017, after the publication of an earlier study showing no association between shift length and patient safety, the governing body of graduate medical education backtracked on shift limits. Maximum shift length for first-year residents was increased from 16 to 24 hours, and more shift-to-shift variation was permitted for senior residents, as long as the 80-hour weekly cap was maintained when averaged over four weeks.
It was an important development, according to Asch and his colleagues, because it seemed that educational policy would finally be based on evidence rather than opinion.
Moving toward evidence-based policy in medical education makes sense. After all, as Asch pointed out, we would never approve a new drug without strong evidence supporting its use.
But it’s my view that using these studies to justify further loosening work-hour restrictions doesn’t make sense. This new study provides strong evidence that shorter shifts are just as safe for patients as longer shifts.
Given what we know about the effects of sleep deprivation on emotional capacity and residents’ well-being, why would we relax work limits again without proof that doing so would cause no harm?
Clayton Dalton is a resident physician at Massachusetts General Hospital in Boston.