Tiger Woods Wins His 5th Masters Title, Marking A Career Comeback

Tiger Woods won his fifth Masters title at Augusta National Golf Club on Sunday, nearly 11 years after his last major win.
Kevin C. Cox/Getty Images
hide caption
toggle caption
Kevin C. Cox/Getty Images
Tiger Woods won his fifth Masters title on Sunday, marking an incredible comeback from injury and personal hardship that ended a nearly 11-year-long championship drought.
Woods finished the final round of his 22nd Masters appearance 13 under par, winning the tournament by a single stroke over Xander Schauffele, Dustin Johnson and Brooks Koepka, who were tied for second place.
Sunday’s win at Augusta National — where Woods won his first major in 1997 — was his 15th time winning a major. Prior to Sunday, Woods hadn’t won a major championship since his victory at the U.S. open in 2008.
With five Masters titles, he is now just one victory away from tying the record for most Masters wins held by American Jack Nicklaus, who has six. The victory also brought Woods closer to tying Nicklaus’ record of 18 major championships.
“THE RETURN TO GLORY!”
Tiger Woods wins the Masters for the 5th time. pic.twitter.com/u3cNdQm6MG
— CBS Sports (@CBSSports) April 14, 2019
The win capped a stunning professional comeback for Woods, who has faced crippling back and leg injuries that led to multiple surgeries and nearly ended his professional golf career. In 2017, he underwent a spinal fusion, his fourth back surgery, with hopes of alleviating the pain.
It was also his first victory at a major since a series of personal troubles that began in 2009 pushed Woods to take a break from the sport.
As the final round of the tournament got off to an early start Sunday morning due to bad weather, it wasn’t clear that Woods would come back from two strokes behind, but he did.
“I was just trying to plod my way along the golf course all day, then all of a sudden I had a lead,” Woods said after his victory. “Coming up to 18, it was just trying to make a five. When I tapped the putt in — I don’t know what I did. I know I screamed.”
As the ball went in, the crowd erupted into applause and chants of “TIGER! TIGER!”
Orioles’ Chris Davis Ends Hitless Streak

Chris Davis of the Baltimore Orioles on Saturday succeeded breaking out of his 0-for-54 hitless streak.
SACHA PFEIFFER, HOST:
Yesterday afternoon, Baltimore Orioles first baseman Chris Davis ended a Major League Baseball record-breaking streak – a streak no baseball player ever wants to be part of. When he stepped to the plate in the first inning at Fenway Park in Boston, Davis had gone 0 for 54. He hadn’t gotten a hit since last September. Then with a count of one ball and no strikes, Red Sox pitcher Rick Porcello offered him up something – a thigh-high fastball on the inside corner of the plate.
(SOUNDBITE OF ARCHIVED RECORDING)
UNIDENTIFIED ANNOUNCER: Porcello out of the full windup – Davis is going to get one. Base hit into right field. Mancini will score. Smith will score. RBIs – one and two. And for Chris Davis, it’s over, baby.
PFEIFFER: Even though Davis was playing in a hostile territory of Fenway, the crowd joined the announcers in the excitement of seeing his burden finally lifted. And then, kind of as a joke or maybe not, Davis did what most major leaguers do when they’ve reached a milestone. He asked for the ball.
(SOUNDBITE OF MUSIC)
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
How Philadelphia Mandated Vaccinations In 1991
NPR’s Sacha Pfeiffer speaks with Dr. Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, about the last time the U.S. mandated measles vaccinations.
SACHA PFEIFFER, HOST:
Mandatory measles vaccinations have been ordered for people living in parts of Brooklyn, N.Y. That’s the order of New York City Mayor Bill de Blasio. And it was prompted by a measles outbreak in some ultra-Orthodox Jewish communities there. Vaccination rates are low in those communities, and an anti-vaccination movement is spreading there. Requiring vaccines is a rare public health move, but there is a precedent. During a 1991 outbreak in Philadelphia, city officials mandated vaccinations for children against their parents’ will. Dr. Paul Offit treated children during that outbreak. He’s director of the Vaccine Education Center at Children’s Hospital of Philadelphia. And he joins us to talk about the experience.
Dr. Offit, welcome.
PAUL OFFIT: Thank you.
PFEIFFER: In New York, Mayor de Blasio has said anyone who doesn’t comply will be fined. But he hasn’t said that people will be forced to get an injection or take a pill. In Philadelphia, was anyone actually forced to be vaccinated?
OFFIT: Yes. There’s a distinction between mandatory vaccination and compulsory vaccination. What de Blasio is asking for is mandatory vaccination, which is to say, get a vaccine. If you don’t get it, then you’ll pay some sort of societal price. You may have to pay a fine or something like that. Here in Philadelphia, we had compulsory vaccination, which is to say, your child got a vaccine whether you wanted your child to get a vaccine or not. It was a court order.
PFEIFFER: And how did Philadelphia get to that point?
OFFIT: Well, we – in that several-month period in early 1991, we had 1,400 cases of measles and nine deaths. It was a major epidemic. I mean, parents were scared to death in this city. The city became a feared destination. It was a nightmare.
PFEIFFER: You were treating children who came to the hospital with measles. What condition were those kids in?
OFFIT: Well, typically, when you’re hospitalized with measles it’s because you have severe pneumonia caused by the virus or you have a bacterial superinfection that was set up by the virus when it infected your lungs or you have severe dehydration. Those were generally the reasons children came into the hospital.
PFEIFFER: So they were – they – these kids were in tough shape.
OFFIT: Yes. And this was at the point where, actually, they were compelled to come in. This epidemic centered on two fundamentalist churches – Faith Tabernacle and First Century Gospel, which were faith-healing churches. So it wasn’t just that they didn’t immunize. They also didn’t choose medical care. And so they often let their children get very sick before, frankly, they were compelled by law to bring them to the hospital.
PFEIFFER: What did their parents tell you about why they hadn’t vaccinated their children?
OFFIT: They were profoundly of the belief that Jesus would protect their children. And they said Jesus was our doctor.
PFEIFFER: And did they also believe that vaccines could cause their kids harm? Were they skeptical about them in other ways?
OFFIT: I think they were just skeptical of modern medicine, period. They saw modern medicine as an act of man. They saw Jesus as someone who could protect their child, independent of whether or not man intervened.
PFEIFFER: In Philadelphia, when those mandatory vaccines were ordered, were there any legal challenges to them?
OFFIT: Yes. The pastor of the Faith Tabernacle Church actually did challenge that because, frankly, what he was doing was perfectly legal. We had had a religious exemption to vaccinations on the book for 10 years. There was nothing he was doing that was illegal. And so he asked the American Civil Liberties Union to represent him, but the ACLU was unwilling to take the case. They said, basically, while they believe that you are at liberty to martyr yourself to your religion, you’re not at liberty to martyr your child to your religion. So they didn’t take the case.
PFEIFFER: Given the fears that many people out there have about vaccines, do you have any qualms or concerns about mandatory vaccinations?
OFFIT: No. I think that were those fears well-founded, sure, I could understand it. I mean, if vaccines cause what they fear vaccines cause, like chronic diseases like autism or diabetes or multiple sclerosis or attention deficit disorder or hyperactivity disorder, sure. But vaccines don’t cause that, so they’re making bad decisions based on bad information that’s putting their children and other children at risk. I mean, at some point, somebody has to stand up for these children.
PFEIFFER: To take us back to present day, is there anything you think was learned from the Philadelphia experience that could be applied to New York City today?
OFFIT: Only just how bad it can get. I guess I just think we invariably fail to learn from history, which is why, occasionally, we’re condemned to repeat it. I mean, do we really need to learn that measles is a potentially fatal infection? Do we need to learn that? Before there was a measles vaccine, 500 people died every year in this country, and most of them were children. Forty-eight thousand people were hospitalized. Do we really need to keep learning that lesson? You know, we eliminated measles from this country in the year 2000. And I think not only did we largely eliminate that virus, I think we eliminated the memory of that virus. People don’t remember how sick it could make you. And that’s why, I think, they can be so cavalier about these kinds of choices.
PFEIFFER: Dr. Paul Offit is director of the Vaccine Education Center at Children’s Hospital of Philadelphia. And he treated children during a measles outbreak in Philly in 1991. Dr. Offit, thanks for talking with us.
OFFIT: Thank you.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Dervish Finds New Ways To Celebrate Tradition With ‘The Great Irish Songbook’

Dervish’s latest album Irish Songbook is out now.
Colin Gillen/Courtesy of the artist
hide caption
toggle caption
Colin Gillen/Courtesy of the artist
For the past three decades, Dervish has been at the forefront of reinventing traditional Irish folk songs. The Sligo-based band is “breathing new life” into the beloved music of its homeland with The Great Irish Songbook, an album pulling from an eclectic range of genres and the voices of over a dozen featured artists.
Collaborators on the album include Steve Earle, David Gray and Rhiannon Giddens and this project encompasses everything from traditional dance music to love ballads, including a W.B. Yeats-penned serenade “Down by the Sally Gardens” and the classic “The Rocky Road to Dublin.”
The Great Irish Songbook is out now. Founding Dervish member Shane Mitchell and longtime vocalist Cathy Jordan spoke with NPR’s Scott Simon about the band’s unlikely beginnings, the soul of Irish music and the making of The Great Irish Songbook. Hear the radio version of their conversation in the audio link and read on for interview highlights.
Interview Highlights
On the origin of Dervish
Mitchell: We basically were a group of friends that were growing up together. We were asked to make a recording of local music one time and we had to come up with a title for the album pretty quickly. And we were just called The Boys of Sligo.
Jordan: I wrecked it. [Laughs] They couldn’t be The Boys of Sligo anymore!
It was about ’91 when when I joined. I was, at that time, making cakes and making pastries in County Longford and singing on the weekends. I had known the guys for quite some time and they decided that it was time to get a singer and I decided that I was fed up making cakes. I hitchhiked down to Sligo with my rucksack on my back and never came back.
On why the Irish excel at songs about heartbreak
Jordan: The heartbreak, I guess, comes in many forms. It can come in immigration, leaving loved ones behind, of course, the affairs of the heart. We have far more songs about love unrequited than songs with happy endings, which I found [out] one time when I was asked to sing as somebody’s wedding. They wanted a lovely traditional Irish ballad with a happy ending and I couldn’t find one. There’s usually somebody dead by the third verse and betrayed by the fourth or whatever. So, I’m not quite sure, there could be many reasons for it, but we have a few happy endings songs, you’ll be delighted to know on The Great Irish Songbook.
On how beloved Irish music is around the globe
Mitchell: We continue to be surprised by how loved Irish music is. I suppose when we started this project nearly two years ago, the idea was to try and find people who had a love for Irish music from different genres of music. We found a lot of closet Irish folk music fans. In fact, we have enough to make three albums, somebody said at one stage.
I am so proud of our music, that there’s so much love and people get emotionally attached to us. It’s a very positive genre of music and this was one of the reasons why we looked at this project. These are iconic songs that we all grew up with. You know, Irish pub music, people come together and it was a great sense of camaraderie when people would sing together. We just think that this was a great way to approach an album — breathe new life into these wonderful old songs.
Examining Sanders’ Medicare-For-All Proposal
Julie Rovner, chief Washington correspondent for Kaiser Health News, describes the latest Medicare-for-all bill by Sen. Bernie Sanders and the options for single-payer coverage proposed by lawmakers.
SCOTT SIMON, HOST:
Bernie Sanders has introduced a new version of his “Medicare for All” bill that was a cornerstone of his 2016 presidential campaign. He’s one of several Democratic candidates for president who support some form of national single-payer coverage. But is that easier said than done? Julie Rovner, chief Washington correspondent for Kaiser Health News joins us. Julie, thanks for being with us.
JULIE ROVNER: Thanks for having me.
SIMON: And what’s Senator Sanders proposing this year?
ROVNER: Well, he’s proposing similar to what he’s been proposing since the 1990s, which is basically to make Medicare, the program that now serves 50-some million elderly and disabled Americans, available to everyone and basically get rid of private health insurance at the same time. So everyone would be on Medicare – might not be the same Medicare that we know now, but they would be on a federal government-run program called Medicare that would provide much more robust benefits than most people have now either on Medicare or on their private insurance.
SIMON: More robust benefits, but would that also mean more robust taxes?
ROVNER: Yes, it almost certainly would because there would be no more private health insurance premiums, according to the – at least the proposal that we have. People wouldn’t have to pay copays or coinsurance or deductibles or, you know, the money that now gets paid out of pocket. So taxes would presumably go up to make up for that.
SIMON: A lot of Democratic candidates are running on a policy of Medicare for All. What are some of the features of the plans that we might find worth knowing about?
ROVNER: Well, the Medicare for All plans would basically get rid of private insurance, and this is of some concern for those who are worried about the political prospects. There’s 150 million people who get their insurance from a family member’s employer. That would basically go away. The entire private insurance industry would go away.
There are some other proposals that would either maintain a role for private insurance – maybe they could cover some things. That’s how some countries do it. And then there are others that make the whole thing optional. The people who wanted to go into a public plan could go into a public plan, but those who wanted to keep their private coverage could do that. That’s one of the big debates that’s going to have to happen before anybody settles on any particular plan.
SIMON: And everybody seems to want to bring down health care costs, but there’s a big but, isn’t there?
ROVNER: There is a big but. You know, we are still a free country. If they bring them down too much, you might have providers who wouldn’t want to participate, or you might have hospitals closing their doors.
I mean, at some point, yes, health care is expensive. It doesn’t have to be as expensive as it is in the United States. We pay way more for things than other countries do, but there is going to be some kind of a limit on how low you can push those prices. But remember, however much you pay for the health care, that’s how much is going to have to be then raised in federal taxes to pay for this.
SIMON: Any chance of Republican support for any of these plans?
ROVNER: It seems highly unlikely, at least at this point. This is mostly a Democratic debate about, what do Democrats think the nation’s health care should look like in the coming years and probably decades? Republicans are still kind of figuring out exactly what they would like to propose. Everybody seems to support more coverage, and they know that the status quo isn’t working. People are paying too much, and even middle-class people often can’t afford their health care. But Republicans are – seem, at the moment, happy to call this socialism and leave it at that.
SIMON: If there is an overhaul of health care, but it’s not bipartisan, does that just mean that American health care is going to go back and forth, depending on which party’s in power?
ROVNER: Well, that is the big concern. And there are a lot of Republicans who are saying, you know, we really should work together. And there is some bipartisanship going on now on issues like prescription drug prices and surprise medical bills – that people get unexpected out-of-network bills. But even those are proving difficult to find bipartisan consensus on – at least enough consensus to pass a law. So I think both sides know it would be better if they got together. They just haven’t figured out how yet.
SIMON: Julie Rovner, chief Washington correspondent for Kaiser Health News. Thanks so much.
ROVNER: Thank you.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Saturday Sports: NBA Playoffs, Baseball Season Begins
ESPN’s Howard Bryant talks with Scott Simon about the start of the NBA playoffs and some of the story lines from the early days of baseball season.
SCOTT SIMON, HOST:
Politics, policies, yada, yada. Time for sports.
(SOUNDBITE OF MUSIC)
SIMON: Two weeks into the baseball season, the standings look upside-down. And the NBA says so long to a couple of legends. Playoffs begin today with – what? – without LeBron. Howard Bryant of ESPN joins us. Hi, Howard.
HOWARD BRYANT, BYLINE: Good morning, Scott. How are you?
SIMON: I’m fine, thanks. But for the first time since 2005, LeBron James is not leading a team into the playoffs. Notice how I managed to make him the lead anyway?
BRYANT: He’s still the news. But the real news in the NBA, of course, is the same question we’ve been asking for about – what? – four years now.
SIMON: Yeah.
BRYANT: Can anybody beat the Golden State Warriors four times? I’m still unconvinced. I know that the Cleveland Cavaliers did it once, but I think the answer is no. I think they’re going to win their third straight championship. However, that does not mean that there’s not a lot of intrigue in here. I like the Milwaukee Bucks, as well. They had the best record in the NBA…
SIMON: Howard…
BRYANT: …Won 60 games.
SIMON: Howard…
BRYANT: Fear the deer.
SIMON: Fear the deer.
BRYANT: (Laughter) I knew that was coming.
SIMON: I love that. Yes, exactly.
BRYANT: We also want to know if the Boston Celtics can turn their disastrous season on – I mean, I know winning 49 games is not really disastrous, but still. They were supposed to be in Milwaukee, in the Warriors’ class, but they weren’t. I think it’s going to be interesting, also, to see what the Philadelphia 76ers do and also those Toronto Raptors, who were flustered by LeBron all those years. But now they’ve got Kawhi Leonard, and LeBron’s not here. So I think that the postseason’s going to be really interesting.
SIMON: Two great players and classy guys – Dwyane Wade of the Miami Heat, Dirk Nowitzki of the Dallas Mavericks – have played their last game. How should we remember their careers?
BRYANT: Great, great players, and I think that this is – I’m an ’80s guy, of course. And I think when you look at the number of Hall of Famers that came out of that decade, I think that the numbers still show it was a pretty amazing decade. But this is a golden age, as well. I think that looking at Dirk and Dwyane Wade – met for a championship twice – in 2006, with the Heat winning that one, although I think Dallas should’ve won that one; and then, of course, in 2011 when – LeBron’s first year in Miami – Dallas winning that one when, of course, people thought Miami should’ve won that one.
So two phenomenal players – lovely that Dirk played 21 years with one team, which you don’t really see anymore. And I think that both of these guys are going to be remembered as the icons for their cities that they were – and also, Dirk, especially, in terms of growing the international game – coming in from Germany; changing the perception, in a lot of ways, of what European players could be; and also, really immersing himself in the culture in Dallas. He’s the greatest player they’ve had.
SIMON: Come into the studio this morning – Stu Rushfield, our technical director, has a scrap of west – wastepaper on our…
BRYANT: (Laughter).
SIMON: …On my reading stand showing the New York – and can’t – Mets – thought they played basketball – in first place. The Cubs – well, not doing well, although they beat the Angels last night. What’s going on? The standings seem upside-down.
BRYANT: Yeah, what’s up with your ball club, Scott Simon? The Cubs are a really interesting team because I think when they won it in 2016, I think people were expecting a long run of success. And now Joe Maddon didn’t get his extension, so you’re starting to wonder what is – what his future’s going to be.
I think when you’re looking at the Mets, obviously, they’re 9-4. They’re in first place and ahead of the Phillies by a game. I think the Red Sox, the defending world champions in the crazy American League East – there’s only one team in that division that has a winning record, and it is the Tampa Bay Rays. The Yankees don’t have any players right now.
I think it’s fascinating. It’s – and it’s good. This is one of the things that makes baseball different. It’s a sprint up – it’s not a sprint. It’s a marathon. It’s going to take a long time. You’re starting to wonder, do these teams have what it takes to just be there? Even at the All-Star break, what are they built for? But when you start the season, it is kind of interesting that the San Diego Padres are in first place. It’s not what we’re used to.
SIMON: Howard Bryant, thanks so much.
BRYANT: Thank you.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
For Some Quidditch Players, The Magic Wears Off As Injury Risks Grow Clearer

Quidditch is a fast-paced, co-ed, full-contact combination of dodgeball, rugby and basketball. Above, John Sheridan tries to score points by throwing a quaffle ball through the other team’s hoop.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
It happened in a split second, and Vanessa Barker doesn’t remember any of it. She doesn’t remember dropping to the field, nor does she remember how she got hit.
When she came to, she was sitting on the sidelines with an EMT, being evaluated for what turned out to be her first concussion. Over the next two years, she’d suffer another two more while out on the field — hardly what she expected when she decided to start playing quidditch.
Before 2005, quidditch existed only as a creation from the fictional world of Harry Potter — a pastime for witches and wizards on flying broomsticks. But charmed by the game’s allure, students at Middlebury College in Vermont held the first real-life quidditch match, a fast-paced, co-ed, full-contact combination of dodgeball, rugby and basketball.

Vanessa Barker of the University of Maryland has suffered three concussions while playing quidditch.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
Nearly a decade-and-a-half later, participation has grown dramatically, with teams sprouting up in communities and college campuses across the country. The sport has its own governing body, U.S. Quidditch, with 134 teams already registered this season and another five to 10 more added each year.
But as teams gather in Texas this weekend for U.S. Quidditch Cup championship, players, coaches and officials are increasingly grappling with how to minimize risk in a game where the potential for injury has become more and more apparent. Many have come to realize it’s not just scrapes and bruises — it’s also broken bones, and for players like Vanessa Barker, repeat concussions.
“If I ever have any others, I’ll have to stop playing,” she said.
The rules of quidditch
The real life game of quidditch is similar to the fictional sport, sans the flying broomsticks. To make up for that, players run with a piece of PVC pipe between their legs, sprinting up and down the field with as many as five balls in play at a time.
There are seven players to a team. Three “chasers” try to score a volleyball through hoops on both sides of the field, each set defended by the opposing team’s “keeper.”
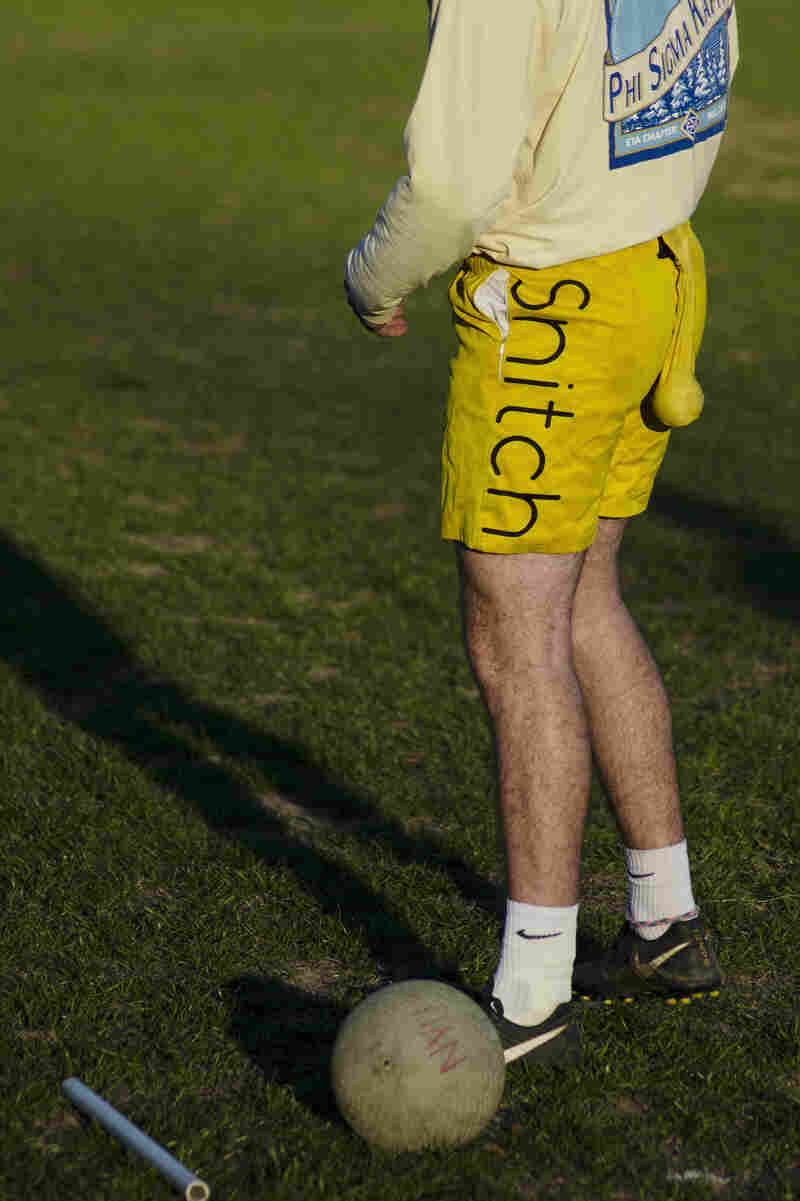
Just as with the rules of quidditch from the Harry Potter series, in real-life quidditch, once a seeker catches the snitch, the match is over.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
While the chasers focus on scoring, two “beaters” try to stop them by either tackling them or throwing dodgeballs at them. Meanwhile, a seventh player, the “seeker,” goes after the ultimate prize: the snitch. Once a seeker catches the snitch, the match is over.
Matches can be intense. Players run at full-speed without any required protective equipment other than a mouthguard. And because the game is co-ed, players of all gender are tackling each other.
Barker is a beater on the University of Maryland quidditch team. This means she often competes against other beaters to get the dodgeballs, or “bludgers,” that they use to heave at chasers. At 5 feet, 2 inches tall, she’s the shortest person on her team. Male players sometimes tower a foot over her.
“I’ve gotten egregiously tackled many times, where they tackle me too hard for no reason,” she said.
Barker said her second concussion happened when she was tackled by a 200-pound male during tryouts. She got another when a male beater hit her in the head with the bludger, but without letting the ball go, essentially punching her in the head.
On the field, Barker has seen a range of other injuries. During her freshman year, she said the president of her team broke his collarbone twice.
“I’ve seen broken thumbs, broken noses, broken collarbones,” Barker said.
Studying injuries
Amelia Gurley, a former quidditch player, has seen these types of injuries too — particularly as the sport has grown more competitive. A medical student at Brown University, Gurley is now trying to answer a fundamental question: how dangerous is quidditch really? In February, she began work on what she hopes to be the first international quidditch injury survey.

John Sheridan (left) lunges to steal the ball from Dan Reise.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
“I worry,” she said. “We’re a new sport. No one’s really even looking into this.”
To date, the most comprehensive data comes from a 2017 study by researchers at the University of Edinburgh who surveyed roughly 50 percent of all quidditch players in the United Kingdom.
The study revealed a mixed picture. While overall injury rates were no higher than in other recreational sports, concussions accounted for more than 20 percent of all injuries. That made concussions the second most common injury overall, according to Ashley Cooper, one of the study’s authors. Sprains were the most common injury, at roughly 26 percent. Lacerations, at about 18 percent, were the third most common injury type.
The authors called the study’s concussion numbers “relatively high when compared to other full contact sports.” For comparison, the study noted that the concussion rate in professional rugby was between 3 percent and 10 percent of all injuries.

Caleb McConnon rubs his neck during practice. According to a study by researchers at the University of Edinburgh, concussions account for more than 20 percent of all injuries in quidditch. Above, players stretch during a quidditch practice at the University of Maryland.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
Men and women are injured at roughly the same rate, according to the study, but women experienced concussions at nearly double the rate as men.
There are still no studies of injuries in U.S. Quidditch, making it difficult to tell how safety compares in the U.S., where thousands play the game, and the U.K., where the number of players is estimated in the hundreds.
USQ declined to provide specific injury data, but Sarah Woolsey, its executive director, said the league was aware of the concussion risk and noted that medical personnel are required to be present at every official USQ game.
“Every single certified coach in our league is required to complete a concussion training webinar,” Woolsey said. “If any player is suspected of having a concussion … they’re immediately removed from play and cannot return to play unless they are cleared by a medical professional.”
Rethinking the rules
For newcomers to quidditch, the physical nature of the game can be eye-opening.
“I thought it’d be a load of super fans with scars on their heads running around the field,” said Cooper, referring to Harry Potter’s trademark scar.
A quidditch player himself, Cooper said he got “absolutely battered” playing the game. “I thought if it was contact it’d be these asthmatic nerds running around and it wasn’t.”
Now, many players are starting to think more seriously about whether the rules of quidditch need to be reevaluated
One of the biggest debates in the sport is about tackling technique. USQ rules only allow one-armed tackles, but some players have begun to wonder whether two-arms would be safer.
“When you have the broom in one hand and you’re trying to make a tackle, it makes it awkward, you have to twist or fall backwards and throw them over you,” said Mack Morgan, a co-captain of the University of Maryland quidditch team. “With a two hand tackle there’s never really going to be that twisting motion.”
Morgan said that many of the injuries he sees on the field — like torn knee ligaments, broken collarbones and concussions — come from that twisting motion.
Woolsey declined to say whether USQ was considering two-armed tackles, but pointed out that USQ players are required to sign a waiver that states that quidditch is a full contact sport.
Another topic of debate is the co-ed nature of the game and whether it’s safe for differently gendered people to be tackling one another — not only because players don’t wear protective padding, but also because of the size differences between players.
“One of the parts of the rules deals with reckless or excessive force,” Woolsey said. “Our athletes understand it might take a different amount of force to tackle somebody who is smaller versus somebody who is bigger.”
Many players say they’d be reluctant to eliminate co-ed play. Many say they were drawn to the sport because of how inclusive it is for people of all genders, including those who identify as nonbinary.
“It’s nice being able to play sports with people of all genders and all backgrounds,” Gurley said.

University of Maryland quidditch co-captain and chaser/keeper Mack Morgan catches his breath after a competitive team scrimmage.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
Rules are typically updated every year, Woolsey said, based on feedback from players and internal data about injuries gathered at every official USQ game.
She said she thinks quidditch is approaching a point where the rules are more permanent, but will still probably change a bit.
“Even sports that have been around for over a hundred years make changes,” she said.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Members of the University of Maryland quidditch team gather at the end of a recent practice. Though research is limited, some who play the game are starting to think more seriously about whether the rules of the sport need to be reevaluated.
Noah Fortson/NPR
hide caption
toggle caption
Noah Fortson/NPR
But as Gurley from Brown University pointed out, there are still many quidditch teams across the country that are not affiliated with USQ. So even if USQ were to make changes, those would not necessarily have any impact for players on non-USQ teams.
Gurley’s former team, the Providence Ashwinders, is not an official USQ team, so it doesn’t need to abide by USQ regulations. Once, she remembers a game that her team played where an EMT was not present until halfway through the tournament.
“Different people in different places are playing quidditch differently, which can be great,” Gurley said. “But it can also be dangerous when it comes to things like safety … We’re not wizards. We can’t fix that kind of stuff with a wave of our wands.”
Republican State Lawmakers Split Over Anti-Abortion Strategy

{kind=link}
In the Tennessee capitol, state Rep. Matthew Hill took heat from abortion-rights proponents last month who had gathered to protest a bill he favored that would ban abortions after about six weeks’ pregnancy. That legislation was eventually thwarted in the Tennessee senate, however, when some of his fellow Republicans voted it down, fearing the high cost of court challenges.
Sergio Martinez-Beltran/WPLN
hide caption
toggle caption
Sergio Martinez-Beltran/WPLN
The new anti-abortion tilt of the U.S. Supreme Court has inspired some states to further restrict the procedure during the first trimester of pregnancy and move to outlaw abortion entirely if Roe v. Wade ever falls. But the rush to regulate has exposed division among groups and lawmakers who consider themselves staunch abortion opponents.
On Thursday, Ohio became the latest state to ban abortions after a fetal heartbeat can be detected. For a long time, Ohio Right to Life supported a more gradual approach to restrict the procedure and deemed what’s come to be called a “heartbeat bill” too radical — until this year. Restricting abortions after a fetal heartbeat can be detected basically bans the procedure after six weeks’ gestation — before many women know they’re pregnant.
“We see the Court as being much more favorable to pro-life legislation than it has been in a generation,” spokeswoman Jamieson Gordon says. “So we figured this would be a good time to pursue the heartbeat bill as the next step in our incremental approach to end abortion-on-demand.”
The Ohio law contains no exception for pregnancies that are the result of rape or incest; it does have an exception for the life of the mother.
Some say the rush to pass these bills is about lawmakers competing to get their particular state’s law before the Supreme Court. The state that helps overturn Roe v. Wade would go down in history.
More than 250 bills restricting abortions have been filed in 41 states this year, according to the Guttmacher Institute, a reproductive rights research and advocacy group.
“After the appointment of Justice [Brett] Kavanaugh, there really is just an environment in state legislatures to roll back abortion rights. And so we’re seeing these bans just fly through,” says Elizabeth Nash, who monitors state laws at Guttmacher.
But the speed of passage of some of these laws masks divisions about strategy and commitment to the cause within the anti-abortion movement.
Tennessee infighting over ‘heartbeat bill’
In Tennessee, for instance, there’s a philosophical split between pragmatists and idealists.
A heartbeat bill in the state has had high-profile support, including from the Tennessee’s new governor. But the Republican attorney general warned such a law would be difficult to defend in court. And several Republicans, swayed by that logic, voted no for the heartbeat bill.
“This is an issue that is extremely important to me. It’s the reason I got into politics many years ago,” Republican state Rep. Bill Dunn said as the House approved the measure over his objection earlier this year. Dunn says he wants to stop abortion, but that will require strategy. He points out that no heartbeat bill has ever been enforced. And recent laws in Iowa and Kentucky have been immediately blocked in court. The same is expected for Ohio.
“Number one, it’ll probably never save a life if we go by what’s happened in the past,” Dunn argued on the Tennessee House floor.
But it’s money that ultimately stopped the heartbeat bill this year in Tennessee (It stalled in committee this week, though the state’s Senate Judiciary Committee agreed to review the bill this summer.)
Senate Speaker Randy McNally says he’s pro-life too, but has no interest in wasting tax dollars to make a point.
Even worse, in the view of Republicans who voted against the heartbeat bill, the state could end up paying the legal fees for groups that defend abortion.
“That is a big concern,” McNally says. “We don’t want to put money in their pockets.
The last time Tennessee had a case that went to the U.S. Supreme Court, it cost roughly $1.9 million. The experience was enough to give a few anti-abortion crusaders some pause. They voted this week with Democrats for a one-year delay on a heartbeat bill, vowing to study the issue over the summer.
Name-calling in Oklahoma
Even if it doesn’t result in a case that upends abortion law, heavily Republican legislatures like Oklahoma’s want to be ready.
“If Roe v. Wade ever gets overturned, we won’t be prepared,” Republican Senate Pro Tempore Greg Treat said while explaining his so-called “trigger bill” at a committee hearing in February.
Treat’s legislation, modeled after existing laws in a handful of states, would “trigger” a state ban on abortion and make it a felony if Roe were overturned. A handful of states, including Arkansas, Kentucky, Louisiana, Mississippi, North Dakota and South Dakota, already have trigger laws on the books.
Oklahoma has some of the strictest abortion laws in the nation, such as mandatory counseling and a 72-hour waiting period. But the most conservative anti-abortion activists in the state want more immediate action. So they targeted Treat and other self-described pro-life Republicans with protests, billboards and fliers, accusing them of not being anti-abortion enough.
“I’ve been called every name in the book these past few weeks,” Treat says. “I’ve had my Christianity questioned. I’ve had a member of my own caucus hold a press conference and call me a hypocrite.”
In response, Treat abandoned the trigger bill.
Now he’s trying something else — an amendment to the state constitution that would reinforce that nothing in Oklahoma law “secures or protects” the right to abortion. But that’s still not anti-abortion enough for some.
“It’s going to add on to that legacy that we have of death and just status quo pro-life policy that does nothing,” says Republican state Sen. Justin Silk.
Not far enough in Georgia
In Georgia, a heartbeat bill passed the legislature, but has paused at Gov. Brian Kemp’s desk. Supporters of abortion rights don’t want him to sign it, of course, but some anti-abortion activists aren’t happy either.
“It really just does not go far enough in the protection of innocent human life,” says Georgia Right to Life executive director Zemmie Fleck. Fleck argues that certain exceptions in his state’s bill — for abortions after rape or incest if the woman makes a police report — make it weak.
Gov. Kemp has until May 12 to sign or veto the measure.
Cost as no object in Kentucky
The American Civil Liberties Union in Kentucky sued the day after a heartbeat bill was signed into law by Gov. Matt Bevin. But even during his annual speech to the Kentucky legislature in February, Bevin acknowledged his intent to challenge Roe v. Wade.
“Some of these will go all the way to the U.S. Supreme Court. But at the end of the day, we will prevail because we stand on the side of right and we stand on the side of life,” Bevin said.
Kentucky has become accustomed to defending abortion restrictions in court. Currently, one law that makes it a felony for a doctor to perform a common abortion in the second trimester has been suspended indefinitely.
It is unclear how much it costs Kentucky to defend abortion laws that are immediately challenged. In an emailed statement, Bevin administration spokesman Woody Maglinger writes that the state is using in-house lawyers, and hasn’t hired outside counsel. He declines to provide a cost estimate on hours spent on these cases.
“It is impossible to place a price tag on human lives,” Maglinger writes.
This story is part of a reporting partnership that includes NPR, Kaiser Health News and member stations. Blake Farmer is Nashville Public Radio’s senior health care reporter, and Jackie Fortier is senior health care reporter for StateImpact Oklahoma. Marlene Harris-Taylor at WCPN in Cleveland, Lisa Gillespie at WFPL in Louisville and Alex Olgin at WFAE in Charlotte, N.C., also contributed reporting.
Watchdogs Cite Lax Medical And Mental Health Treatment Of ICE Detainees

{kind=link}
A guard escorts a detained immigrant from his “segregation cell” back into the general population at the Adelanto Detention Facility in November 2013. Today the privately run ICE facility in Adelanto, Calif., houses nearly 2,000 men and women and has come under sharp criticism by the California attorney general and other investigators for health and safety problems.
John Moore/Getty Images
hide caption
toggle caption
John Moore/Getty Images
It’s Saturday morning and the women of the Contreras family are busy in Montclair, Calif., making pupusas, tamales and tacos. They’re working to replace the income of José Contreras, who has been held since last June at Southern California’s Adelanto ICE Processing Center, a privately run immigration detention center.
José’s daughter, Giselle, drives around in an aging minivan collecting food orders. First a hospital, then a car wash, then a local bank.
Giselle’s father crossed from Guatemala more than two decades ago, without authorization to enter the U.S. He worked in construction until agents picked him up and brought him to Adelanto.
Giselle says her father languished there for three months without his diabetes medication. Now, she says, the guards give it to him at odd times during the day and night. And, she says, ICE agents took his eyeglasses so he can’t read legal documents or write letters.
“My aunt tried to take in glasses for him but they don’t allow for us to give them anything,” Giselle tells me as she steers the minivan. “They tell us that they give them everything they need.” When I ask if her father has glasses now, she says, “No, he doesn’t. He doesn’t have glasses.”

Maria Contreras, José’s sister, makes papusas and other food for sale in Southern California — to help support the family while José is in detention at the ICE Adelanto Processing Center. He has been held there for months without his glasses or requested counseling for depression, she says, and doesn’t get his diabetes medication when he needs it.
Sarah Varney/Kaiser Health News
hide caption
toggle caption
Sarah Varney/Kaiser Health News
Giselle says her father, who is 60 years old, is terrified of being deported, and she says the regimented world inside Adelanto is driving him into a deep depression. “His conversations now have become shorter,” she says. “He doesn’t talk to us and ask, ‘How’s your day? How you been?’ He’s always looking down at the ground; he doesn’t want to make eye contact for the same reason that he’s so depressed.”
José’s sister, Maria Contreras, visits her brother every Saturday. She has urged him to see a psychologist at Adelanto, but he tells her that even though he filled out a medical request, he doesn’t get any help. “No response, or anything,” Maria says.
Adelanto sits on a desolate stretch of road in the high desert about an hour north of the city of Riverside. Nearly 2,000 men and women are held here. Some arrived recently during the surge in border crossings. Others lived in the U.S. — undocumented and undetected — for years. In the visiting room, where detainees are brought in wearing blue, orange or red baggy pants and tops, a sign on the wall reads, “Don’t give up hope.”
José Contreras with his family, in happier times. He came to the U.S. from Guatemala without authorization more than two decades ago and worked in construction until agents picked him up and took him to Adelanto.
Sarah Varney/Kaiser Health News
hide caption
toggle caption
Sarah Varney/Kaiser Health News
The facility — run by a federal contractor, GEO Group, a for-profit company based in Boca Raton, Fla., that runs private prisons — has a troubled past. During an unannounced visit last year, federal inspectors from the Department of Homeland Security’s Office of the Inspector General found “nooses” made out of bedsheets in 15 out of 20 cells. The inspectors found that guards overlooked the nooses even though a detainee had died by suicide using a bedsheet in 2017 and several others had attempted suicide using a similar method. The government audit concluded GEO Group guards improperly handcuffed and shackled detainees, unnecessarily placed detainees in solitary confinement and failed to provide adequate medical care.
A separate investigation of Adelanto and other immigration detention facilities in California released in February by state Attorney General Xavier Becerra found similar health and safety problems and concluded that detainees were treated like prisoners, some kept in their cells for 22 hours a day, even though they have not been charged with a crime. A state law passed in 2017 directs the state to inspect and report on the treatment of immigrant detainees held in California.
The alleged cases documented in the most recent report by Disability Rights California, a watchdog group with legal oversight to protect people with disabilities in the Golden State, are grim: detainees slitting their wrists; discontinued medication for depression; and ignored requests for wheelchairs and walkers. At least one detainee said that guards pepper-sprayed him when he did not stand up and a second time while he tried to hang himself.
In a written statement, GEO Group says it “strongly disputes the claims” in the report and that the remedies recommended by Disability Rights California “were already in place.”
“We are deeply committed,” the company says, “to delivering high-quality, culturally responsive services in safe and humane environments.” An ICE spokesperson says, in an emailed statement, that GEO Group’s Adelanto facility is in “full compliance with the Americans with Disabilities Act.”
But Mario, who was inside Adelanto for six months in 2018, says the report describes his own experiences there. “What’s happening is all those claims that have been made against GEO and the staff in the medical department are finally being backed up by reports,” Mario says.
He asked us not to use his last name since he is out on bond and still fighting deportation. Mario is now 32; he crossed the border with his parents without documentation when he was 5.
In 2017, he was convicted of a misdemeanor and ICE agents picked him up at his home in Ontario, Calif. At the time, Mario was seeing a therapist for depression and taking medication. It took three weeks to get back on antidepressants, he says, and the sessions with the psychologists at Adelanto were only cursory.
“They keep their actual sessions to five to 10 minutes,” he says. “It’s basically like a quick check-in. They just ask you, ‘How are you? Do you have any suicidal thoughts? When is your next court date?’ It’s one of those things that I feel is basically done just to say, ‘All right, we did it.’ “
Mario is gay and lived in a room with three other men, including a gay man from Mexico who was seeking asylum. The two men became close friends.
“He was persecuted in Mexico because of being gay,” Mario says. Months of detention “and not getting any mental health care really took a toll on him. And that’s when he cut himself. He cut his wrist with a razor blade that we get to shave. And after that he was placed in solitary confinement for about a week.”
Mario says when his friend came back to their room, he was taking some sort of medication. “After that, all he did was sleep,” Mario says. “When the food was ready I’d go call him: ‘OK, it’s time to eat.’ “
Other detainees and immigration lawyers described a similar pattern, of GEO psychiatrists prescribing antipsychotic medications that make people sleep much of the time. It’s one of the reasons people were reluctant to seek help, Mario says. But also, like other detainees, he was worried about being labeled as depressed.
“I couldn’t express whenever I was extremely feeling sad or depressed or anxious because I was afraid that would be used against me in court,” he explains.
Judges cannot use mental health conditions to deny legal status to a detainee, according to immigration attorneys.
Last month, long after GEO Group says the company addressed any problems detailed in the Disability Rights California report, detainees in Adelanto staged a hunger strike. The detainees gave an attorney a handwritten note, which was released by the Inland Coalition for Immigrant Justice, an advocacy group.
Chief among their demands was speedier access to good medical care.
Sarah Varney is a senior national correspondent at Kaiser Health News, a nonprofit health newsroom that is an editorially independent part of the Kaiser Family Foundation.
The Issue Of Medicare For All Is Dominating The 2020 Democratic Field
Several 2020 Democratic candidates support Medicare for All, but what would that proposal look like in action?