
Dr. Carlos Gutierrez examines a young girl at a shelter in El Paso that was set up for recent migrants. The girl’s mother said her daughter’s deep cough arose while the family was in immigration custody.
Anna Maria Barry-Jester/Kaiser Health News
hide caption
toggle caption
Anna Maria Barry-Jester/Kaiser Health News
It wasn’t the rash covering Meliza’s feet and legs that worried Dr. José Manuel de la Rosa. What concerned him were the deep bruises beneath. They were a sign she could be experiencing something far more serious than an allergic reaction.
Meliza’s mom, Magdalena, told the doctor it started with one little bump. Then two. In no time, the 5-year-old’s legs were swollen and red from the knees down.
U.S. immigration officials are releasing up to 700 people a day into El Paso, Texas. Ciudad Juárez, in Mexico, can be seen in the distance.
Anna Maria Barry-Jester/Kaiser Health News
hide caption
toggle caption
Anna Maria Barry-Jester/Kaiser Health News
De la Rosa noticed a bandage-covered cotton ball in the crook of Meliza’s elbow, a remnant of having blood drawn. During their time at the Immigration and Customs Enforcement detention facility in El Paso, Meliza had been sent to a hospital, Magdalena explained, cradling the child. They had run tests, but Magdalena had no way to get the results. Through tears, she begged for help. “My daughter is my life,” she told him in Spanish.
The doctor would see nearly a dozen patients that March evening at his makeshift clinic inside a warehouse near the El Paso airport. That week, similar ad hoc community clinics would treat hundreds of people, some with routine colds and viruses, others with upper-respiratory infections or gaping wounds. Like Meliza, all were migrants, mostly from Central America, a river of families arriving each day, many frightened and exhausted after days spent in government detention.
De la Rosa, an El Paso pediatrician, is one of dozens of doctors volunteering on the U.S.-Mexico border as the flow of migrants crossing without papers and asking for asylum climbs to a six-year high. Unlike previous waves of immigration, these are not single men from Mexico looking to blend in and find work.
Most are families, fleeing gang violence, political instability or dire poverty. (Meliza and other patients are referred to by their first or middle names in this story because of their concerns that speaking to the news media could affect their asylum cases.)
President Trump has declared a national emergency on the southwestern border to free up billions of dollars in funding to construct a wall as a means of stemming the tide of asylum seekers. He is expected to make an appearance in Calexico, Calif., Friday to tour a 30-foot section of fence that was rebuilt last year.
But the federal government isn’t covering the cost of the humanitarian crisis unfolding in border communities like El Paso.
In the absence of a coordinated federal response, nonprofit organizations across the 1,900-mile stretch have stepped in to provide food, shelter and medical care.
Border cities like El Paso, McAllen, Texas, and San Diego are used to relying on local charities for some level of migrant care. But not in the massive numbers and sustained duration they’re seeing now. As the months drag on, the work is taking a financial and emotional toll. Nonprofit operators are drawing on donations, financial reserves and the generosity of medical volunteers to meet demand. Some worry this “new normal” is simply not sustainable.
“The care we are providing we could never have foreseen — or imagined spending what we are spending,” said Ana Melgoza, vice president of external affairs for San Ysidro Health, a community health system providing care for migrants crossing into San Diego. She said her clinic has spent nearly $250,000 on such care since November.
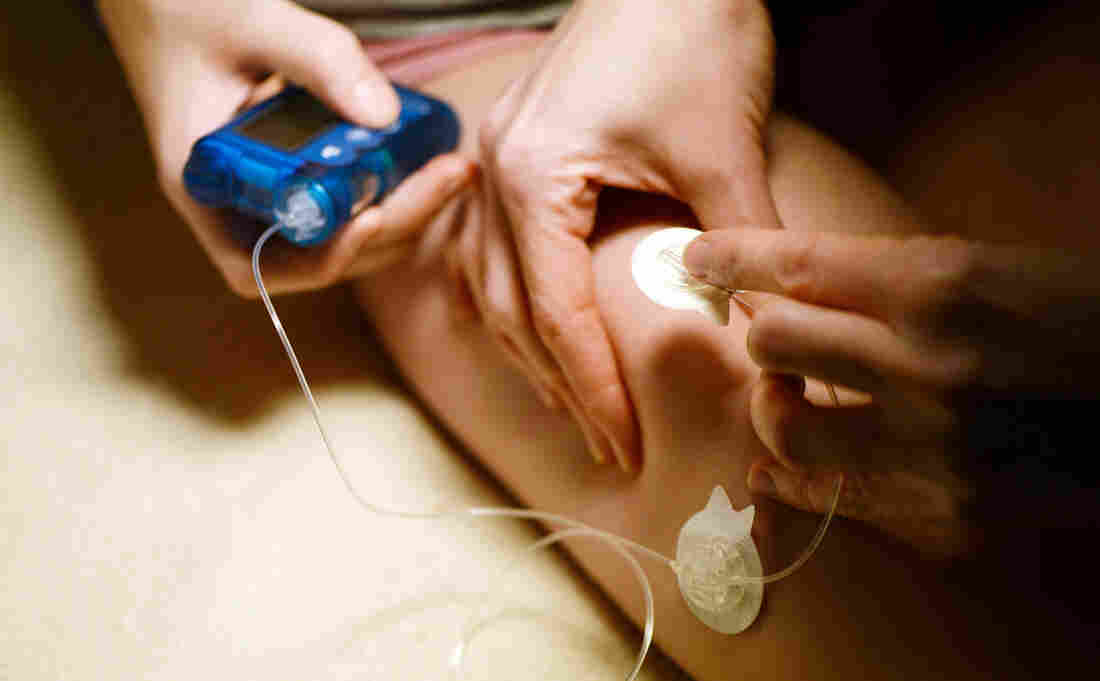
At an ad hoc clinic in an old warehouse in El Paso, Dr. José Manuel de la Rosa discusses an insulin prescription with a woman who has diabetes.
Anna Maria Barry-Jester/Kaiser Health News
hide caption
toggle caption
Anna Maria Barry-Jester/Kaiser Health News
An emotional and financial toll
In October, the U.S. Immigration and Customs Enforcement agency drastically changed how it handles migrant releases from its detention facilities. Families seeking asylum no longer would get help coordinating travel to live with relatives or sponsors while claims were processed. Since the policy shift, thousands of migrants have found themselves in border cities without money, food or a way to communicate with family. From Dec. 21 to March 21, 107,000 people were released from ICE detention to await immigration hearings.
In El Paso, which has seen a 1,689 percent increase in border apprehensions of migrants traveling with family members compared with last year, volunteer doctors are staffing a network of clinics. Kids with coughs and colds, diarrhea and vomiting are common. Some migrants have severe blisters on their feet that need cleaning, or diabetes that’s out of control because, they say, their insulin was thrown away by border patrol agents.
For de la Rosa, this is just the latest work in a career tied to border health. Born and raised in El Paso, he has served on the U.S.-Mexico Border Health Commission since President George Bush appointed him in 2003. He was founding dean of the city’s Paul L. Foster School of Medicine when it opened a decade ago as one of the few programs in the country that requires all students to take courses in “medical Spanish,” designed to bolster communication with Spanish-speaking patients.
As he entered the warehouse-turned-shelter that evening in late March, he pulled off his signature bow tie and draped a stethoscope around his neck. He thinks it’s a gift to be able to help people who would otherwise have no way to get care. “Sometimes I don’t know if I’m doing it for me or for them,” he said. “It is so fulfilling.”
But cases like Meliza’s are frustrating for the doctors, because they can’t see them through.
After passing an initial screening to claim asylum, Meliza and her mother had been taken to the warehouse, where volunteers gave them food and a bed, and helped arrange travel to South Carolina, where they could live with a family member as their asylum claim proceeds.
Meliza’s rash began while they were in detention, Magdalena told de la Rosa. And four days in, she was sent to a hospital. But they were released from custody before getting the test results. De la Rosa called the hospital, hoping the labs would offer clues as to whether the girl might have leukemia; Henoch-Schonlein purpura (a disorder that can cause kidney damage); or just an allergic reaction. The hospital asked de la Rosa for a privacy waiver from the mother, but by the time he could return to the shelter for her signature, she had boarded a bus for South Carolina. That would be the last he saw of her.
‘The best we can do’
Born and raised in El Paso, De la Rosa has served on the U.S.-Mexico Border Health Commission since President George Bush appointed him in 2003. Helping migrants get the health care they need is fulfilling he says. But many days he’s frustrated and overwhelmed by the lack of government support.
Anna Maria Barry-Jester/Kaiser Health News
hide caption
toggle caption
Anna Maria Barry-Jester/Kaiser Health News
Dr. Carlos Gutierrez, another El Paso pediatrician, is also desperate for communication with the doctors who work inside the detention facilities. When people are released with complicated health issues — like a man who recently showed up with a flesh-eating bacterial infection and a wound so big they could see his bone — the volunteer doctors often have to start from scratch, trying to determine what a patient has and what treatment they’ve been given.
For much of the past five months, Gutierrez has used the lunch break from his private pediatric clinic to see migrants. He works in one of several hotels being rented out by Annunciation House, a nonprofit that runs the area’s main shelter network.
The organization, which is funded through donations from religious organizations and individuals, has dug deep, spending more than $1 million on hotels in the past four or five months, its executive director said at a city council meeting. It struggles to accommodate everyone — Annunciation House recently scrambled to open a temporary shelter so that 150 people wouldn’t have to sleep in a city park.
On his way to the hotel, Gutierrez reviewed the day’s text message from the organization’s director outlining how many refugees would be arriving that day: 510.
The first patients treated that day in his improvised clinic — set up in a hotel room bathroom — were 9-year-old twins from Guatemala. They were traveling with their mother, Mirian, who said she fled her hometown after local men threatened to kidnap one daughter if she didn’t pay protection money to operate her tortilla stand.
Mirian and her daughters had crossed a small river to reach what she believed was New Mexico, she said, imagining that the authorities they surrendered to would be like the U.S. tourists she’d met in her hometown. “There, when the tourists arrive, they are so nice. Even doctors come to help us,” she said in Spanish.
But the welcome in the U.S. was not warm. During the six days the family spent in federal custody, one of her daughters contracted bronchitis, Mirian told Gutierrez. They were healthy when they entered, she said, but sleeping on cold concrete floors and eating skimpy ham and cheese sandwiches broke them down. “They treat you as if you’re trash,” she said.
Mirian showed Gutierrez an inhaler she was given in the detention facility and asked what it was for. Her other daughter had developed a deep cough and needed attention, she said. After examining both girls, Gutierrez explained about the inhaler, and showed Mirian how to help her daughter use it. The girls would be fine, he told her, but with their lungs as congested as they were, it might be weeks before they recovered.
“I mean, this is the best we can do,” Gutierrez said, after prescribing an antibiotic to a little girl with an ear infection. “We could be doing it better. But when they are in our care nobody is dying.”
De la Rosa examines a rash on the foot of a 5-year-old girl named Meliza. Though he believed it was likely a sign of an allergic reaction, the underlying bruising could also signal serious infection or leukemia, he worried. Before he could get the test results he needed, the family was gone.
Anna Maria Barry-Jester/Kaiser Health News
hide caption
toggle caption
Anna Maria Barry-Jester/Kaiser Health News
Necessary work
More than two dozen people have died while in immigration custody under the Trump administration, according to a calculation based on a recent NBC News analysis. The government says it added nurses and doctors to its facilities after two children died in December. Immigration authorities are now taking 60 children a day to the hospital and doing medical screens for every child under 18, U.S. Customs and Border Patrol Commissioner Kevin McAleenan said during a March news conference.
But many people still have serious needs upon release. When Gutierrez and his colleagues started these clinics, they were meant to temporarily fill a gap caused by the change in government policy. Asked if he thinks the volunteer work is sustainable, he shook his head and sighed. “I’m so tired.”
The financial model — relying on donations and volunteers — also has its limits. Asylum seekers generally don’t qualify for social services, including Medicaid, before they have been granted asylum. In California, negotiations are underway to make some of the $5 million in emergency funds the state is spending at the border available to reimburse clinics for care, according to the office of state Sen. Toni Atkins. Physicians in Texas and Arizona were not aware of similar conversations in their states.
Dr. Blanca Garcia, another El Paso pediatrician, has been volunteering a few days a week since October. Like many of the doctors, she cites a moral and financial argument for providing care to the migrants, who are in the country legally once they apply for asylum. These are vulnerable people who might not otherwise seek care, and for every diagnosis of strep throat, she is likely preventing an expensive emergency room visit, she said.
Still, there are limitations to what they can provide.
Cristian, 21, and his 5-month-old baby, Gretel, arrived at an El Paso shelter in a former assisted living facility early one afternoon. He’d never been alone this long with his daughter, he said. His wife — a minor — had been separated from them at the border, put in the custody of the Department of Health and Human Services. Cristian didn’t know when she might be released.
While in detention, he had spent several nights with Gretel on a concrete floor in a room with more than a hundred other men, he said. He asked a guard for a better sleeping situation. Instead of receiving help, he said, he was punished by being forced to sit and stare at a wall for over an hour as Gretel cried in his arms.
Still breastfeeding before she was separated from her mother, she would suck on his nose and at his shirt. He was worried that she wasn’t getting enough to eat, and that the formula he was giving her wasn’t as good for her as breastmilk. Dr. Garcia told him the baby looked healthy.
Still, Cristian was anxious, and grew increasingly distressed as he recounted their history.
“Will the baby be OK?” he asked in Spanish.
She assured the young father he was doing everything he could.
This story was produced by Kaiser Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. KHN is not affiliated with Kaiser Permanente.
Let’s block ads! (Why?)








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}