Trump Declares Opioid Crisis A Public Health Emergency

Today, President Trump declared the opioid crisis a public health emergency. What difference will that make in the effort to fight the problem?
Today, President Trump declared the opioid crisis a public health emergency. What difference will that make in the effort to fight the problem?

Nearly half of the federal funding has been cut for the navigator program that Shelli Quenga leads for South Carolina’s Palmetto Project.
Alex Olgin/WFAE
hide caption
toggle caption
Alex Olgin/WFAE
Despite all of the efforts in Congress to repeal and replace the Affordable Care Act this year, it remains the law of the land. People can start signing up for health insurance for 2018 starting Nov. 1. But the landscape for the law has changed a lot.
Take navigators, for instance. Those are specially trained people who help consumers sign up for coverage. In August, the Centers for Medicare & Medicaid Services cut funding for navigators by 41 percent.
But the effects vary. For some groups and some states, the cuts go deeper while others will have almost as much money as they did before.
South Carolina and North Carolina are cases in point. South Carolina’s navigator funding is about two-thirds less than the state received in fiscal 2017, while most of North Carolina’s funding is intact.
The Trump administration has said that it is rewarding groups that did a good job and cutting off those that didn’t. But the strategy may have the effect of hobbling navigators who have the most daunting job enrolling people.
“We are between the rock and the hard place,” says Shelli Quenga, who runs programs at the nonprofit Palmetto Project, South Carolina’s largest navigator group. “We know that people in rural areas don’t have as much Internet access. The people who need help are probably in the rural areas, but we can’t afford [to send navigators there].”
Ilia Henderson (left) is planning to sign up for a health insurance plan on the federal marketplace with help from Charlotte, N.C.-based navigator Julieanne Taylor (right) again this year.
Alex Olgin/WFAE
hide caption
toggle caption
Alex Olgin/WFAE
Instead, Quenga says, she will have to be strategic about where she plans to place navigators. “It is based on those areas that are (a) more densely populated and (b) had a higher level of ACA enrollment for 2017,” she explains.
That means about two-thirds of the state’s counties will not have a navigator. Quenga is still planning to help people in those areas by using screen-sharing technology to walk people through sign-ups. She adds that people can always call the federal call center for help. But that’s not ideal, she says.
Quenga says her employees really take the time to work through complicated cases. For example, she says, “Lots of people have family members sleeping on their couch. Do you count that person as a tax dependent or not?”
The answer is complicated. How much financial aid someone gets is based on his or her taxable income, which changes with the number of dependents, she says. “Choosing whether to include that person as a dependent can have big consequences in terms of your financial assistance,” she says. “The call center is not set up to run those scenarios for you.”
And with less help from the federal government, Quenga feels the pressure mounting to get more people signed up for coverage during this year’s shorter enrollment period. If she does, there’s a chance her navigator group will be better funded next year.
The picture is very different in North Carolina. There, navigator groups had only about 10 percent of their federal funding cut.
Jennifer Simmons, who coordinates North Carolina’s largest navigator program, the NC Navigator Consortium, says she is happy to report there will be someone available in each of the state’s 100 counties during the six weeks of open enrollment this year.
They will help people like Ilia Henderson, who is 26 and lives in Huntersville, just outside Charlotte. She is one of those young healthy people insurance companies want and she is getting ready to sign up for coverage with navigator Julieanne Taylor.
Last year, Taylor helped Henderson, a massage therapist and student, sign up for a medical and dental plan within half an hour for just over $100 a month. She looks forward to working with Taylor to find a similarly good deal for 2018. Simmons says her navigators will be in libraries, public health departments and even churches around the state.
“We are remaining really laser-focused on making sure that consumers across North Carolina are able to get info they need. There are a lot of people that need renewal services and help in making sure that the marketplace has their updated information and that the plan that they are in is still the right plan for their family,” Simmons says. “But we are also trying to reach new people.”
Last year, North Carolina had one of the highest marketplace enrollments, with more than half a million people signing up. South Carolina, with about half of North Carolina’s population, has about 183,000 people enrolled.
Sabrina Corlette, with Georgetown University’s Center on Health Insurance Reform, says sign-ups are likely to drop during this open enrollment period.
“It’s just been decision after decision,” she says. “Including this navigator funding cut that will ultimately lead not to just lower enrollment in the marketplaces but sicker enrollment in the marketplaces.”
If that happens, Corlette says, count on higher premiums in 2019 with fewer people in the insurance pool.
This story is part of a reporting partnership with NPR, WFAE and Kaiser Health News. You can follow @alexolginon Twitter.

Spencer Platt/Getty Images
President Trump could declare a national emergency to deal with the opioid epidemic Thursday, freeing up resources for treatment and to better monitor prescriptions. More than 140 Americans die every day from an opioid overdose, according to the Centers for Disease Control and Prevention.
The president first said he’d declare the opioid crisis a national emergency in August, but the proposal languished until this week.
Some in the field, like Dr. Andrew Kolodny, say it’s been frustrating to wait for the administration to respond to a crisis Trump first acknowledged on the campaign trail when he was running for president.
Kolodny, who is co-director of the Opioid Policy Research Collaboration at Brandeis University’s Heller School, says he expected immediate action after the president’s August statement. “If you’re calling something an emergency, you expect people to act urgently and respond as if it’s an emergency.”
After taking office, President Trump appointed a commission to study the opioid crisis, headed by New Jersey Gov. Chris Christie. In an interim report, the commission called on the president to declare a national emergency. Doing so would free up funds for treatment, ensure wider access to the anti-overdose drug naloxone and improve monitoring of opioid prescriptions to prevent abuse.
In August, days before the president promised to declare a national emergency, Health and Human Services Secretary Tom Price said he didn’t think one was necessary. Flash forward two months, though, and Tom Price is gone.
Dr. Keith Humphreys, a professor of psychiatry at Stanford University and a former adviser in the Obama administration says that Price was not a friend to addiction treatment programs. “When he was a congressman, he opposed the parity law which required insurers to cover addiction treatment,” Humphreys says. “He was very skeptical of methadone maintenance which is a very good treatment for heroin addiction. So having him out of the way is a potential plus.”
In a policy change this week, the director of the Food and Drug Administration told a congressional committee the agency will begin working to promote medication assisted treatment—using methadone, buprenorphine or naltrexone to help addicts in recovery. That’s significant because some states currently won’t pay for some of those treatments. Advocates will be listening for what, if anything, the president says about that.
Humphreys says he’s interested in what measures the president proposes as part of the emergency declaration. For example, he could announce he’ll use his authority to negotiate cheaper prices for drugs. Humphreys says the president could say, “In an emergency, we’re going to use our power as a big purchaser to say to naloxone manufacturers that … we want 40 percent off or whatever, to use that leverage which currently we can’t do legally.”
But, when the president speaks on the opioid epidemic Thursday, advocates say the key issue will be what he says about funding. Congress is currently spending $500 million a year on addiction treatment programs. Dr. Kolodny says to help the more that 27 million Americans abusing opioids, much more is needed. He puts the price tag at $6 billion each year. “You want that opioid addicted individual to be able to access effective outpatient treatment more easily than they can get pills, heroin, or fentanyl,” Dr. Kolody says.
Kolodny criticizes the Obama administration for being slow to acknowledge opioids, a crisis that he says that began in 1996 and which the CDC declared an epidemic in 2011. President Obama’s health secretary Kathleen Sebelius agrees. “Did we do enough? Probably not,” Sebelius says. “Recognizing how widespread this was, what factors were contributing to it, would have been helpful a number of years ago.” And she says, it might have prevented many overdose deaths.
Sebelius notes that the Affordable Care Act and the expansion of Medicaid greatly increased coverage for addiction treatment. If President Trump is serious about tackling opioids, she says his first step should be to stop fighting to repeal Obamacare.

“Obamacare gives states very little flexibility for innovation,” said Iowa Gov. Kim Reynolds, after withdrawing the state’s insurance waiver request.
Charlie Neibergall/AP
hide caption
toggle caption
Charlie Neibergall/AP
Two states looking for approval to customize their health insurance systems under the Affordable Care Act reversed course after the Trump administration said their applications couldn’t be approved in time for next year.
Iowa withdrew its proposal to the Centers for Medicare & Medicaid Services for a waiver to alter its Affordable Care Act markets. Massachusetts’ proposal was effectively denied by the administration.
Both states sought to use some of the money that would have gone toward subsidies for consumers to instead create reinsurance programs that would protect insurers from major losses. Reinsurance often lowers premiums.
Iowa Gov. Kim Reynolds, a Republican, blamed the rules of the Affordable Care Act for the failure of her state’s proposal. “Obamacare gives states very little flexibility for innovation,” Reynolds said at a news conference.
She gave credit to CMS Administrator Seema Verma for trying to get the waiver approved. “Unfortunately Obamacare is an unworkable law,” Reynolds said. She then urged Congress to pass a law to repeal the Affordable Care Act.
But there’s another way of looking at it. CMS took a “hard line” on its interpretation of the law, said Larry Levitt, a senior vice president at the Kaiser Family Foundation. In a letter to Iowa, the agency said the state’s proposal doesn’t meet the law’s requirements that the alternative plan not add to the federal deficit.
“The question is how sharp the pencils have to be that reviewers in HHS are using” Levitt said. “They could be a little looser in their analysis, but would risk a negative report down the road.”
On the same day that Iowa withdrew its waiver, CMS told Massachusetts that the agency couldn’t approve the state’s waiver in time for open enrollment, which begins Nov. 1. The Affordable Care Act requires all proposals to allow 90 days for public comment. CMS said Massachusetts’ application came too late.
The failures of the two states’ waiver applications follow a trend. Several states have seen their proposals delayed, denied or only partly approved, after administration officials actively encouraged states to apply.
Some critics say the denials are part of an administration effort to force the ACA marketplaces to fail. But Levitt says the agency is on solid legal ground in its strict interpretation of the rules.
Still , there appears to be a switch, given the administration’s previous invitation to states to seek permission for insurance market changes.
Former HHS Secretary Tom Price, who resigned last month, encouraged states to apply for the waivers. Just weeks after he was sworn in in February, Price wrote a letter to every governor in the country urging them to consider creating reinsurance programs and high-risk pools.
HHS “invites states to pursue approval of waiver proposals that include high-risk pool/state-operated reinsurance programs,” the letter says. “The Departments will work with states to review all applications within the timeframe provided … and do our best to work with states to review their applications on an expedited basis.”
Sen. Lamar Alexander, R-Tenn., has sought to relax the waiver process. A bipartisan bill he co-authored with Sen. Patty Murray, D-Wash., would cut the wait time for waivers to be approved and allow states to go ahead with just the approval of the governor rather than a vote from the legislature. The bill would also make it easier for states to get copycat waivers once a program has been approved elsewhere.
Alexander said his bill would fix the problems that doomed the Massachusetts proposal. “Under the Alexander-Murray bill, states can get waivers approved in 45 days if the situation requires urgent action,” he said in a statement. “So Massachusetts could have had its waiver approved by now to help reduce chaos when open enrollment begins next week. This is further evidence that the Affordable Care Act needs changes and that states need our bill to get flexibility from the law.”
The Alexander-Murray bill, which was co-sponsored by 24 senators, has yet to be scheduled for a vote, and President Trump has wavered on whether he supports the plan.

The state of New York is putting e-cigarettes into the same category as regular tobacco cigarettes, under new restrictions signed into law this week. Here, a man uses a vape device in London last summer, next to a No Smoking sign.
Tolga Akmen/AFP/Getty Images
hide caption
toggle caption
Tolga Akmen/AFP/Getty Images
E-cigarettes and vaping are being banned in indoor public areas in New York, after Gov. Andrew Cuomo signed a bill into law that will place the same restrictions on new and old nicotine delivery systems.
“These products are marketed as a healthier alternative to cigarettes but the reality is they also carry long-term risks to the health of users and those around them,” Cuomo said, in a news release about the signing. “This measure closes another dangerous loophole in the law, creating a stronger, healthier New York for all.”
Citing the lack of broad regulations on what chemicals e-cigarettes can contain and how much nicotine they deliver, the governor’s office says, “These factors could lead to long-term adverse health effects for e-cigarette users and bystanders.”
When it takes effect next month, New York’s new law will cover vaping under the state’s Clean Indoor Air Act. The blanket restriction will not apply to people who want to use e-cigarettes in private homes, in hotel rooms, or at retail tobacco outlets.
The potential dangers of vaping have become a topic of debate and concern in recent years, even as e-cigarettes have gained in popularity. As recently as last spring, many adult Americans said they didn’t know whether secondhand e-cigarette aerosol poses a risk to children.
As the Shots blog has reported, “Nicotine, heavy metals and tiny particles that can harm the lungs have been found in secondhand e-cigarette aerosol, according to the Surgeon General.”
It wasn’t until May of 2016 that the Food and Drug Administration banned the sale of e-cigarettes to minors, part of a broad set of new regulations the agency adopted after years of planning.
Vaping has caused a dilemma for some lawmakers and health policy experts. As NPR’s Alison Kodjak has reported, ” Some have welcomed the devices as an alternative to traditional cigarettes, whose dangers are well-known, and as an aid to help smokers quit…. Others fear the devices will addict nonsmokers to nicotine and eventually lead to more people smoking.”
Vaping’s backers — such as the Vaper Rights site — warn that restrictions could bring higher prices, broad bans in public places, and “severely limit or even prohibit flavored products for adult consumers.”
In the view of vaping defenders, Vaper Rights says, “E-vapor products are not cigarettes. You don’t light them, they don’t burn tobacco, and they produce vapor, not smoke (hence ‘vaping’ vs. ‘smoking’). The FDA classifies e-vapor products as tobacco products because they contain nicotine derived from tobacco.”
New York joins a growing list of states that have banned vaping in indoor public spaces such as bars and restaurants, in much the same way they restrict smoking. Others on the list include California; Connecticut; New Jersey; and Utah. Some states ban vaping only in areas such as government offices and schools.
As more cities and states have moved to ban vaping indoors, false stories have attempted to stir up controversy and alarm over new regulations. As the Snopes website notes, there is no truth to a story from last August that purported that 11 states were planning to ban vaping in vehicles.

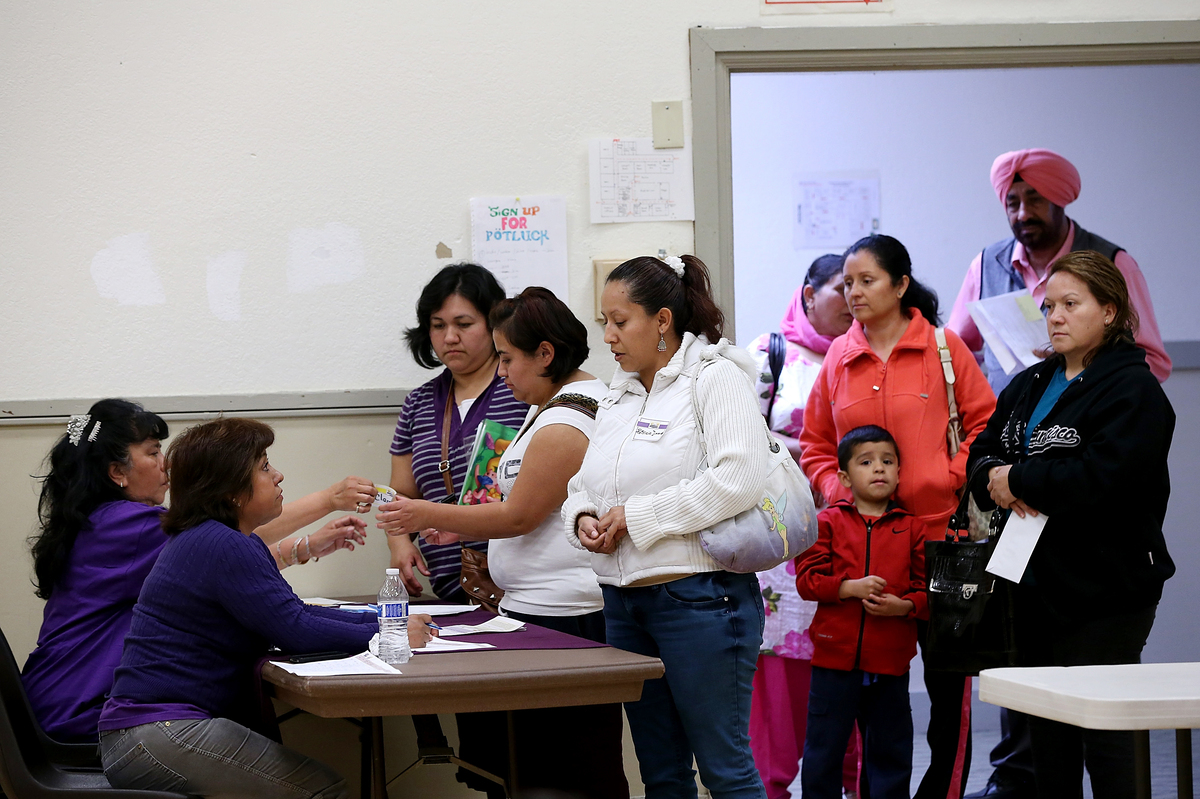
Lines like this one at a health insurance enrollment fair at the Ambrose Community Center in Bay Point, Calif., in 2014 may be longer this winter.
Justin Sullivan/Getty Images
hide caption
toggle caption
Justin Sullivan/Getty Images
For people who buy health insurance through the marketplace created by the Affordable Care Act, the 2018 open enrollment period begins in one week. But many consumers are confused about what to expect. No wonder.
The Trump administration has slashed advertising and outreach about open enrollment, so concrete consumer information is sparse. But there’s more than enough political rhetoric to make up for it, with regular partisan pronouncements that the marketplaces have collapsed and Obamacare is dead.
Though details may change if Congress makes a move, here is key information that consumers can probably bank on. (“Probably,” because in this shifting environment, nothing is certain.)
Shopping for health insurance is about as entertaining as picking dryer lint off your clothes, but this year it’s essential to sit down at your computer or work in person with a navigator (if you can find one; federal funding for these health insurance helpers has been trimmed, too,) and review the plans offered in your area.
All That Glitters May Be Gold
It’s always important to check your plan details to see if the costs, benefits, or providers have changed, and compare them to other plans. This year, failing to do so could mean you’ll miss out on significant opportunities to get more bang for your premium buck.
Marketplace plans are grouped into four levels of coverage. Bronze plans pay 60 percent of covered medical expenses on average, silver plans pay 70 percent, gold picks up 80 percent, and platinum plans pay 90 percent.
Because of a wrinkle in premium pricing this year, some consumers may be able to buy gold plans for a lower premium cost than that of a silver plan. For the same reason, consumers who buy a bronze plan may owe no premium at all.
For lower-income consumers buying coverage on the marketplace, the health law provides two types of financial help. The federal government pays cost-sharing reduction (CSR) subsidies to insurers to shrink deductibles and copayments for people with incomes up to 250 percent of the federal poverty level (about $30,000 for one person), but only if they buy a silver plan.
Also, people with incomes up to 400 percent of poverty (about $48,000 for an individual) can qualify for tax credits to help pay for premiums. The amount of the premium subsidy is based on both income and the cost of a low-priced silver plan.
Earlier this month, President Trump cut off the federal cost-sharing reduction subsidies. While some members of Congress are proposing to restore them, the outlook is unclear.
Recognizing that they might be on the hook financially if the administration cuts off payments, many insurers already incorporated the cost of those subsidies into their premiums for 2018 marketplace plans. Further, on their own or at the direction of state insurance regulators, many insurers limited those CSR price increases to the silver plans to which the premium subsidies are tied.
But boosting silver premiums may also mean that consumers get larger premium tax credits.
Even though premium tax credits are set according to a silver plan, they can be used for any plan. So shoppers who qualify for those subsidies may find that while silver plan premiums are relatively expensive this year, bronze and gold plans may be more affordable, thanks to consumers’ larger premium tax credits.
“Premiums for silver plans are higher, but not for gold or bronze,” says Caroline Pearson, a senior vice president at Avalere Health, a consulting firm. “Premiums for gold and bronze plans are unusually cheap, so they might be a better value.”
In addition, people who don’t qualify for subsidies may find better deals off the marketplace this year, depending on the state they live in.
Use Caution With Auto-Enrollment
If you don’t review your plan and update your income and other personal information, your insurer or the marketplace may automatically re-enroll you in your 2017 plan or another one that is similar in price and coverage. About two-thirds of people surveyed by the Kaiser Family Foundation earlier this fall said they would like to stick with the same plan if it’s available.
That may seem like a simple solution, but if premiums have changed, it could affect how much you owe, and a new plan may have different benefits or a different network of providers. You need to check out your options.
Expect A Shorter Enrollment Window
If you live in a state that uses the federal marketplace, open enrollment ends Dec. 15, about six weeks earlier than last year. That reality, coupled with the fact that in-person help will be tougher to find, means that people should start looking into plans sooner rather than later.
States that run their own marketplaces may allow consumers to enroll through the end of January.
“Don’t wait,” says Sarah Lueck, a senior policy analyst at the Center on Budget and Policy Priorities. Her advice for consumers: “Go and look as soon as you can.”
However, some consumers who miss the Dec. 15 enrollment deadline may have another shot at signing up. If your current plan is being discontinued, you may qualify for a special enrollment period (SEP) because it’s considered a loss of coverage, says Sandy Ahn, an associate research professor at Georgetown University’s Center on Health Insurance Reforms. Consumers in that situation have 60 days after their coverage ends on Dec. 31 to enroll in a new plan.
“If you didn’t know that open enrollment was cut short this year, you might need that SEP,” Ahn says. Consumers should hang on to their insurer letter that tells them they’re losing their coverage under their current plan to document their eligibility.
The Centers for Medicare & Medicaid Services didn’t respond for a request for comment about the eligibility for a special enrollment period in these circumstances.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Follow Michelle Andrews on Twitter: @mandrews110.

Screening for Type 2 diabetes involves a blood test, and if results are concerning a second test is recommended.
ERproductions Ltd/Blend Images/Getty Images
hide caption
toggle caption
ERproductions Ltd/Blend Images/Getty Images
Undiagnosed diabetes may not be as big of a public health problem as thought.
That’s the takeaway from a study published Monday in the Annals of Internal Medicine that says that some previous efforts have likely overestimated the number of people with undiagnosed diabetes because they relied on a single positive test result.
By contrast, this new measure used the American Diabetes Association’s diagnostic criteria, which recommend that people with one positive fasting blood glucose or A1C test should have a second test to confirm a diagnosis in all but the most severe and obvious cases of Type 2 diabetes. That’s because there’s some inherent variability in the tests and because blood sugar levels fluctuate naturally because of exercise, illness and even the time of day.
If left untreated, Type 2 diabetes can contribute to kidney disease, nerve damage, high blood pressure and stroke.
The Centers for Disease Control and Prevention has applied the less stringent standard to data from the National Health and Nutrition Examination Survey and the U.S. Census to come up with an estimate of 33.3 million people with diabetes in 2015, 7.2 million of whom, or almost 24 percent, were undiagnosed. When researchers in this study applied the stricter clinical diagnostic standard to the same data, they came up with an estimate of 25.5 million people with diabetes, with about 2.8 million, or about 11 percent, of them undiagnosed.
“This is good news,” says Elizabeth Selvin, a professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health and the lead author of the study. “We’re doing a good job with screening and diagnosis.”
But she says that doesn’t mean diabetes isn’t a public health problem, and a significant one at that; the study found the prevalence of diabetes in the U.S. population has risen from 5.5 percent in 1988-1994 to 10.8 percent in 2011-2014. The proportion of undiagnosed cases has dropped from 16.3 percent over the same period, the study found.
The difference in how the estimates are calculated is due to the difference between epidemiological studies, which track patterns and trends across an entire population, and clinical practice, which focuses on individual patients. If you’re just studying historical trends, using a single-test value isn’t such a big deal, says Selvin. “But if we are focused on the burden of undiagnosed diabetes, or the percentage of diabetes that’s undiagnosed, it becomes important,” she says. (A CDC spokeswoman says the agency doesn’t directly comment on studies that aren’t its own.)
The results suggest that public health efforts to promote screening should be focused more closely on the people who are most likely to have undiagnosed diabetes rather than the population as a whole. According to the study, that group includes people who are obese, a racial or ethnic minority, and who don’t have health insurance or get regular health care. While increased age is also a risk factor, the authors noted that there’s an undiagnosed group of overweight and obese younger adults with very high A1C levels who are likely not engaged with the health care system and are falling through the cracks.
“We’re not missing hordes of people, which isn’t to say we aren’t missing some people,” says Anne Peters, an endocrinologist and professor of medicine at the Keck School of Medicine at USC, who wrote an editorial accompanying the study. “We need to continue to reach out to the people who do need help.”
She says more and more programs are focused on preventing diabetes in the first place, focusing on people with risk factors such as obesity and high cholesterol. That can help people avoid the complications of full-blown diabetes, and the label of having a chronic disease, which have long-term psychological effects as well as consequences for buying life insurance and long-term care insurance, Peters says. (And health insurance, if current Affordable Care Act rules about pre-existing conditions should change.)
The study’s authors pointed out some limitations of their work. Among them: the data includes fasting glucose and A1C levels taken only at one point in time, and the results might differ if samples were taken later. And the diagnosis of diabetes depends on study participants’ self-reports, which may not be accurate.
Katherine Hobson is a freelance health and science writer based in Brooklyn, N.Y. She’s on Twitter: @katherinehobson.
Steve Inskeep talks to Avik Roy, president of the Foundation for Research on Equal Opportunity, about the president cutting cost-sharing reduction payments, a subsidy under the Affordable Care Act.

The foods on the left contain naturally occurring fibers that are intrinsic in plants. The foods on the right contain isolated fibers, such as chicory root, which are extracted and added to processed foods. The FDA will determine whether added fibers can count as dietary fiber on Nutrition Facts labels.
Carolyn Rogers/NPR
hide caption
toggle caption
Carolyn Rogers/NPR
What counts as dietary fiber? That’s up for debate.
The Food and Drug Administration is reviewing 26 ingredients that food manufacturers use to bulk up the fiber content of processed foods to determine if there’s a health benefit.
If you’re a nutrition-label reader, the list includes some familiar-ish sounding ingredients — such as inulin, which is often sourced from chicory root.
Other ingredients on the “do-these-count-as-fiber?” list include gum acacia, bamboo fiber, retrograded corn starch, and — get ready for a tongue-twister — xylooligosaccharides. Some of these fibers are extracted from plant sources, while others are synthetic.
Some critics argue that the FDA should not allow these added fibers to count as fiber on Nutrition Facts labels.
“The food industry has high-jacked the advice to eat more fiber by putting isolated, highly processed fiber into what are essentially junk foods,” says Bonnie Liebman of the consumer group Center for Science in the Public Interest.
A bunch of packaged foods contain added fiber. Some examples include Fiber One bar products, some cereal and instant oatmeal products, as well as some pastas and English Muffins.
Liebman says most people know that an apple is a healthier choice than a high-fiber brownie, but when they see high fiber counts on the label, “it may just be enough to convince them to go with the brownie.”
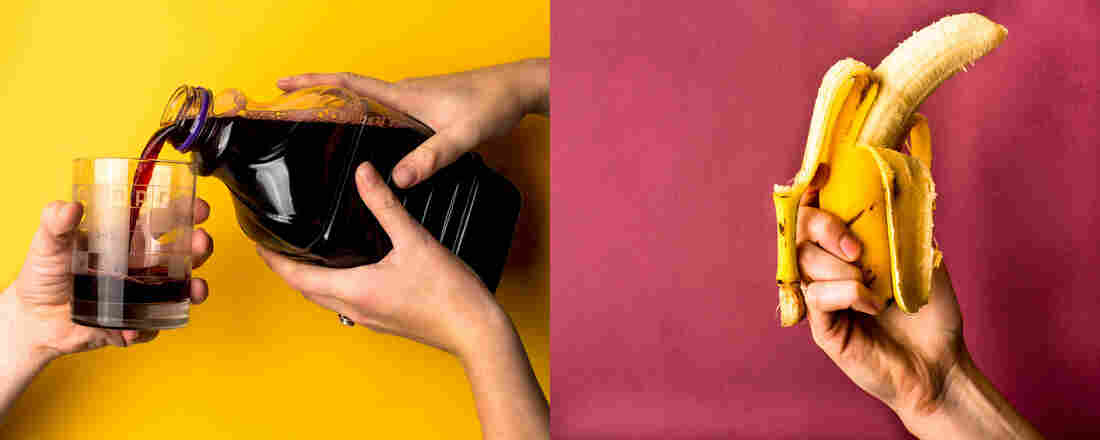
Left: grape juice with resistant maltodextrin as added fiber. Right: a banana that naturally contains fiber and other nutrients.
Carolyn Rogers/NPR
hide caption
toggle caption
Carolyn Rogers/NPR
Liebman argues a much better way to get the recommended 25 to 38 grams of daily fiber is to eat more foods that are naturally rich in fiber such as fruits, vegetables, beans and whole grains.
High-fiber diets may help protect against a range of diseases, from Type 2 diabetes and heart disease to certain types of cancer.
The FDA lists a range of health benefits linked to dietary fiber. For instance, fiber can help lower blood glucose and cholesterol levels, as well as blood pressure. Fiber can also aid laxation and bowel function, and it can promote a feeling of fullness, which may lead people to eat less.
The FDA is in the process of determining whether isolated and synthetic fibers provide a beneficial physiological effect to human health. The agency says, going forward, there must be at least one demonstrated benefit. “Only fibers that meet the definition can be declared as a dietary fiber on the Nutrition Facts label,” according to this Q & A about the review process. The agency is in the process of reviewing the science.
The food industry has weighed in, pointing to the demonstrated benefits of some of these added fibers. “I think the main benefit is that they contribute to regularity and laxation,” says Robert Burns, vice president of health and nutrition policy at the Grocery Manufacturers Association. Burns says most people don’t consume enough fiber, so “if you can supplement [with] snack bars that people are eating, it [can] go a long way to meeting dietary recommendations.”
Critics say an optimal diet is one that includes lots of whole foods such as fruits, vegetables, nuts, beans and whole grains. These foods are not only naturally rich in fiber, they also contain other beneficial compounds such as vitamins, minerals and anti-inflammatory compounds.
“Highly processed snack bars typically contain combinations of processed starch and added sugar. They’re low in vitamins and minerals,” says Dr. David Ludwig of the Harvard School of Public Health. “Just adding isolated fiber back in [to these processed foods] does not cover up for those nutritional deficiencies.”
NPR’s Melissa Block talks to Sarah Kliff, Vox senior policy correspondent, to fact check Trump’s claim that subsidies for insurance companies are “bailouts” and “a windfall” for those companies.
MELISSA BLOCK, HOST:
And now we’re going to truth squad some of President Trump’s latest claims about health care – in particular, what he’s said about his decision to stop paying for subsidies under the Affordable Care Act, or Obamacare. The president has called those subsidies bailouts to insurance companies, a windfall. Sarah Kliff joins us for a fact check. She covers health care policy for vox.com. Sarah, good morning.
SARAH KLIFF: Good morning.
BLOCK: And first, why don’t you give us a quick review of just how these cost-sharing reduction subsidies work?
KLIFF: Yeah, so these are subsidies for low-income Americans who buy Obamacare to help make their co-payments and deductibles a little bit lower, to make it a little easier to go to the doctor. And these payments have – will continue to be paid by insurance companies, even though the government will not finance them. It is just coming out of insurance companies’ own pockets at this point.
BLOCK: So basically, if they get reimbursed by the federal government, that is a wash? They’re getting just made up for what they already paid out?
KLIFF: Yeah, so the federal government, you know, makes these payments each month, and insurance companies, in turn, help lower the co-payments and deductibles of their low-income consumers. What President Trump is changing is he’s not going to make those payments, so insurance companies have no one on the back end, you know, sending them the payment to make up for that spending.
BLOCK: OK. So when President Trump calls those payments a gift to insurance companies, are they a gift?
KLIFF: I would disagree that they are a gift. You know, for one thing, they are going not necessarily to the insurance companies. They’re ultimately going to low-income Americans to help them afford their co-payments and afford their deductibles. So, you know, on that level, they don’t seem like a bailout or a gift to the insurance companies. They are required by the law. The law requires these subsidies to be made. So they’re really – you know, I see them as part of the Affordable Care Act and not necessarily a bailout.
BLOCK: The president has also said, Sarah, that the insurance companies, in his words, made a fortune with Obamacare. Is that true? What do the numbers show?
KLIFF: The numbers are a lot more mixed. The best data on this probably comes from the nonprofit Kaiser Family Foundation, which looks at quarterly margins – so how much insurance companies have each quarter leftover after paying out all those claims. In 2014 and 2015, insurance companies had a quarterly margin of just about $20 a person. That’s not a ton of money. It’s gone up as the Obamacare markets have stabilized.
In 2016, it was about $90 a person, so it’s definitely getting better. But the insurance markets – you know, I’ve covered them since they launched. And they’ve really been a very rocky experience for insurance companies financially. They didn’t know how to price at first. People were sicker than they expected. It’s only in the past year that insurance companies have made decent profits there, but I think of them as a mixed bag when it comes to financial performance.
BLOCK: Decent profits, which raises the question – if the insurance companies are losing the federal payments, they began compensating by jacking up the premiums for other people – right? – raising those premiums a lot – in some cases by double digits. Couldn’t the insurance companies just absorb the costs themselves, cut into their profits but not pass it along to consumers?
KLIFF: Yeah, so one of the things I’ve learned as a health care reporter is insurance companies tend to have relatively low profit margins, usually in the 3 to 4 percent range. So there definitely is some space. But one of the things that surprised me a little bit is state regulators often are the ones saying, you have to make those increases. They’re really worried that insurance companies might get hit with a big claim and not have enough money to pay for it.
So they want to make sure that insurance companies are getting enough revenue from their premiums to cover that loss, to make sure they can actually pay out claims. The worst-case scenario for a state regulator is to have an insurance company that just can’t pay its medical bills for patients.
BLOCK: That’s Sarah Kliff. She’s a senior policy correspondent for vox.com and host of the podcast The Impact, which covers health care policy. Sarah, thanks so much for being with us.
KLIFF: Yeah, thanks for having me.
Copyright © 2017 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}