A Clearer Map For Aging: ‘Elderhood’ Shows How Geriatricians Help Seniors Thrive

Meth In The Morning, Heroin At Night: Inside The Seesaw Struggle of Dual Addiction

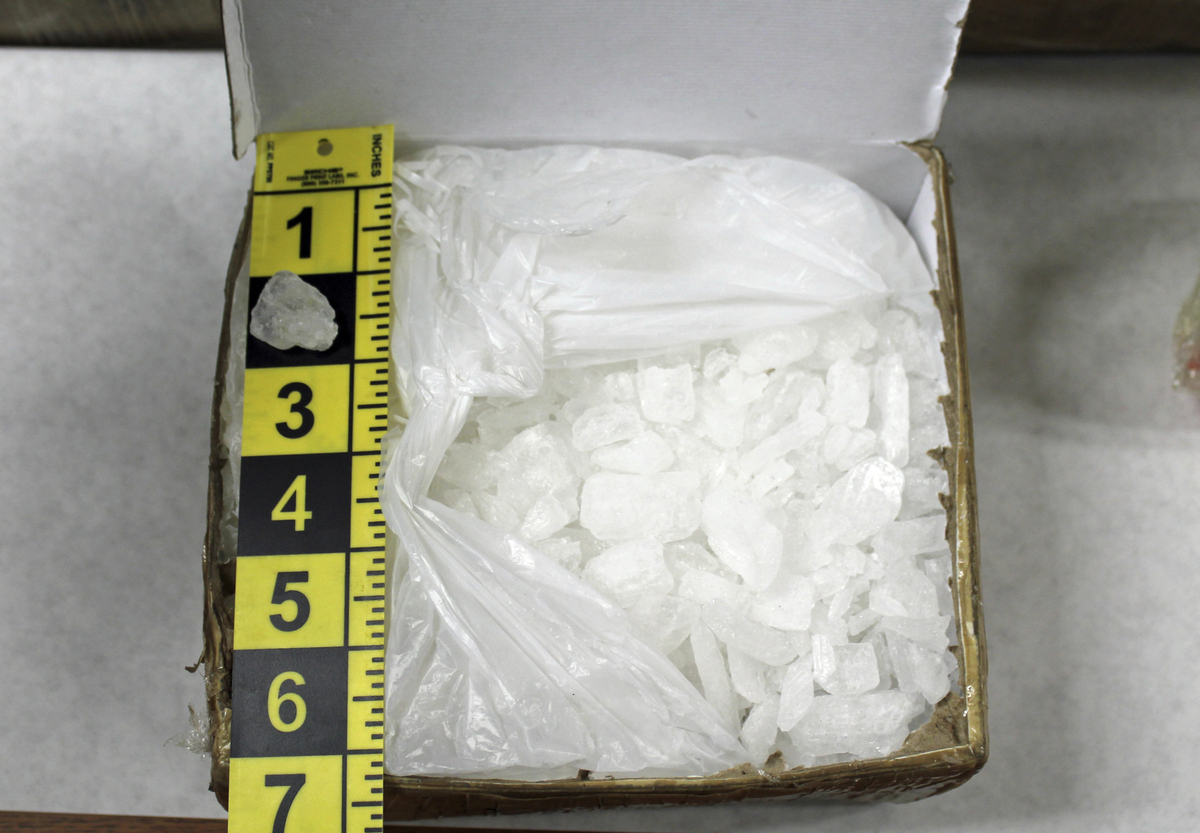
Powder methamphetamine packaged in foil for an illegal street sale. Across the U.S., more and more opioid users report using methamphetamine as well as opioids — up from 19% in 2011 to 34% in 2017, according to one study.
Science Source
hide caption
toggle caption
Science Source
In the 25 years since she snorted her first line of methamphetamine at a club in San Francisco, Kim has redefined “normal” many times. At first, she says, it seemed like meth brought her back to her true self — the person she was before her parents divorced, and before her stepfather moved in.
“I felt normal when I first did it, like, ‘Oh! There I am,’ ” she says.
Kim is 47 now and has been chasing “normal” her entire adult life. That chase has brought her to some dark places, so we agreed not to use her last name, at her request. For a long time, meth, known commonly as speed, was Kim’s drug of choice.
Then she added heroin to the mix. She tried it for the first time while she was in treatment for meth.

After struggling with addiction to both heroin and meth for decades, Kim got care at a residential treatment program for women — Epiphany Center, in San Francisco. She’s now working and plans to go back to college in the fall.
April Dembosky/KQED
hide caption
toggle caption
April Dembosky/KQED
“That put me on a nine-year run of using heroin,” Kim says. “And I thought, ‘Oh, heroin’s great. I don’t do speed anymore.’ To me, it saved me from the tweaker-ness,” she says, referring to the agitation and paranoia many meth users experience, and how heroin, an opiate, calmed that.
Now, Kim has just finished addiction treatment for both drugs.
She was part of the last meth wave of the ’90s, and now she’s part of a new meth epidemic sweeping through parts of the United States, especially the West. Deaths involving methamphetamine are up. Hospitalizations are up.
Taking meth and opioids for a “synergistic high”
Researchers who have tracked drug use for decades believe the new meth crisis got a kick-start from the opioid epidemic.
“There is absolutely an association,” says Dr. Phillip Coffin, director of substance use research at the San Francisco Department of Public Health.
Across the U.S., more and more opioid users say they use methamphetamine as well, up from 19% in 2011 to 34% in 2017, according to a study published in the journal Drug and Alcohol Dependence last year. The greatest increases were in the western United States.
That research suggests that efforts to get doctors to cut down on writing opioid prescriptions may have driven some users to buy meth on the street instead.
“Methamphetamine served as an opioid substitute, provided a synergistic high, and balanced out the effects of opioids so one could function ‘normally,’ ” the researchers write.
It’s kind of like having a cup of coffee in the morning to wake up and a glass of wine in the evening to wind down — or using meth on Monday to get to work and heroin on Friday to ease into the weekend.
Amelia says that’s how her drug use evolved to include meth.
At first, drugs were just a fun thing she would do on the weekend — ecstasy and cocaine with her friends. Then, on Monday, Amelia would just go about her workweek.
“I’m a horse trainer, so I worked really hard, but I also partied really hard,” she says.
Then one weekend, when Amelia was feeling kind of hungover from the night before, a friend passed her a pipe and said it was opium.
“I thought it was like smoking weed or hash, you know?,” Amelia says now. “I just thought it was like that.”
She says she grew to like the opium stuff and eventually contacted the friend’s dealer.
“The woman said, ‘How long have you been doing heroin for?’ and my jaw nearly hit the ground,” Amelia says. “I was just really, honestly, shocked. I was like, ‘What? I’ve been doing heroin this whole time?’ I felt really naive, really stupid for not even putting the two together.”
Pretty soon, Amelia started feeling sick around the same time every day. It was withdrawal symptoms — a clear sign she was becoming dependent on the drug. Her weekend smoke became her daily morning smoke. Then it was part of her lunchtime routine.
“I just kind of surrendered to that and decided, ‘Screw it,’ ” she says. “I’ll just keep doing it. I’m obviously still working, I’m fine.’ “
A heroin habit is expensive. Amelia was working six days a week to pay for it. Any horses that needed to be ridden, any lessons that needed to be taught, she said yes to because she wanted the money.
But bankrolling her heroin use was exhausting. One day, one of the women she worked with at the horse barn offered her some meth as a pick-me-up.
Meth is comparatively cheap these days. It became the thing that kept Amelia going so she could earn enough money to buy heroin.
“The heroin was the most expensive part,” she says. “That was $200 a day at one point. And the meth was $150 a week.”
This pattern lasted for three years, until Amelia discovered she was pregnant. As soon as her daughter was born, she entered a residential treatment program in San Francisco — the Epiphany Center — that would accept her and her baby.
“I was OK with being a drug addict,” Amelia says. “I was OK with that being my life.” she says. “But I wasn’t OK with having kids and letting that be part of my life.”
Rehab admissions on the rise for mixers of heroin and meth
Admissions to drug rehabilitation for heroin have remained steady in recent years in San Francisco. But the number of heroin addicts reporting methamphetamine as a secondary substance problem has been rising. In 2014, 14% of heroin users entering rehab in San Francisco said meth was also a problem. Three years later, 22% said meth was also a problem.
“That is very high,” says Dr. DanCiccarone, a professor of family community medicine at the University of California, San Francisco, who has been studying heroin for almost 20 years. “That’s alarming and new and intriguing and needs to be explored.”
The speedball — heroin plus cocaine — is a classic combination, he says.
“It’s like peanut butter cups, right — chocolate and peanut butter together,” he says. “Methamphetamine and heroin are an unusual combination.”
The meth and heroin combo is colloquially referred to as a goofball, Ciccarone adds, because it makes the user feel “a little bit silly and a little bit blissful.”
For Kim, the methamphetamine use came first. Then she added heroin.
“I ended up doing both at the same time every day, both of them,” she says.
For Kim, it was always about finding the recipe to what felt normal. Start with meth. Add some heroin. Touch up the speed.
“You’re like a chemist with your own body,” she says. “You’re balancing, trying to figure out your own prescription to how to make you feel good.”
Now Kim is trying to find that balance without drugs. She’s been sober for a year. So has Amelia, the horse trainer. Her sober anniversary is the same as her daughter’s birthday.
This story is part of NPR’s health reporting collaboration with KQED and Kaiser Health News.
A Year After Spinal Surgery, A $94,000 Bill Feels Like A Backbreaker

Since her spinal surgery, Liv Cannon has been able to work in the garden and play with her energetic dogs without having to worry about pain.
Julia Robinson for Kaiser Health News
hide caption
toggle caption
Julia Robinson for Kaiser Health News
Spinal surgery made it possible for Liv Cannon to plant her first vegetable garden.
“It’s a lot of bending over and lifting the wheelbarrow and putting stakes in the ground,” the 26-year-old says as she surveys the tomatillos, cherry tomatoes and eggplants growing in raised beds behind her house in Austin, Texas. “And none of that I could ever do before.”
For the first 24 years of her life, Cannon’s activities were limited by chronic pain and muscle weakness.
“There was a lot of pain in my legs, which I can now recognize as nerve pain,” she says. “There was a lot of pain in my back, which I thought was, you know, just something everybody lived with.”
Cannon saw lots of doctors over the years. But they couldn’t explain what was going on. She’d pretty much given up on finding an answer for her pain until her fiancé, Cole Chiumento, pushed her to try one more time.

Liv Cannon and her fiancé, Cole Chiumento, considered calling off their wedding because of uncertainty over medical debt from her surgery. “I think about it every time I go to the mailbox,” Cannon says.
Julia Robinson for Kaiser Health News
hide caption
toggle caption
Julia Robinson for Kaiser Health News
“It never improved. It never got better,” Chiumento says. “That just didn’t sound right to me.”
So Cannon went to a specialist who ordered a scan of her spine. A few days later, her phone rang.
“We found something on your MRI,” a voice said.
The images showed that Cannon had been born with diastematomyelia, a rare disorder related to spina bifida. It causes the spinal cord to split in two.
In Cannon’s case, the disorder also led to a tumor that trapped her spinal cord, causing it to stretch as she grew.
In December 2017, a neurosurgeon opened up her spinal column and operated for several hours, freeing the cord.
“I think it was Day 3 after my surgery I could feel the difference,” Cannon says. “There was just a pain that wasn’t there anymore.”
As she recovered, Cannon saw lots of huge medical bills go by. They were all covered by her insurance plan. Almost a year went by after the operation.
Then a new bill came.
Patient: Liv Cannon, 26, of Austin, Texas. At the time of her surgery, she was a graduate student insured with Blue Cross and Blue Shield of Texas through her job at the University of Texas.
Total bill: $94,031 for neuromonitoring services. The bill was submitted to Blue Cross and Blue Shield of Texas, which covered $815.69 of the amount and informed her she was responsible for the balance. The insurer covered all of Cannon’s other medical bills, which came to more than $100,000, including those from the hospital, surgeon and anesthesiologist.
Service provider: Traxx Medical Holdings LLC, an Austin company that provides neuromonitoring during spinal surgery. Neuromonitoring uses electrical signals to detect when a surgeon is causing damage to nerves.
Medical service: Cannon was born with a rare spinal condition that had caused chronic pain and muscle weakness since she was a child. In December 2017, she had successful spinal surgery to correct the problem. Her surgeon requested neuromonitoring during the operation.
What gives: Neuromonitoring made sense for the type of surgery Cannon had. The bill did not. Cannon should have been warned long before her surgery that the neuromonitoring company would be an out-of-network provider whose fees might not be covered by her insurer.

Liv Cannon was diagnosed with diastematomyelia, a rare disorder related to spina bifida, and had surgery in December 2017 to correct the problem. Most of the cost of the surgery was covered by her insurance, but more than $93,000 for out-of-network neuromonitoring services was not.
Julia Robinson for Kaiser Health News
hide caption
toggle caption
Julia Robinson for Kaiser Health News
At first, she was baffled by the billing information that Blue Cross sent her. “It was one of those things from the insurance company that says this is the amount we cover and this is the amount you might owe your provider,” she says.
The statement listed four separate charges from the day of her surgery. Each was described as a “diagnostic medical exam.” Together, they came to $94,031.
Blue Cross said the covered amount was $815.69 — minus a $750 deductible and $26.27 for coinsurance — and informed Cannon she might have to pay the balance — $93,991.58
“I was shocked,” she says. Chiumento was outraged.
“As soon as I saw that, I thought it was a scam,” he says.
Share Your Story And Bill With Us
If you’ve had a medical-billing experience that you think we should investigate, you can share the bill and describe what happened here.
The bill had come from an Austin company called Traxx Medical Holdings LLC. Traxx did not respond to emails, phone calls and a fax seeking comment on the charge.
The company’s website shows that Traxx provides a service called intraoperative neurophysiological monitoring, which evaluates the function of nerves during surgery. The goal is to help a surgeon avoid causing permanent damage to the nervous system.
There is an ongoing debate about whether neuromonitoring is needed for all spinal surgery. But it is standard for a complicated operation like the one Cannon had, says Richard Vogel, president of the American Society of Neurophysiological Monitoring.
On the other hand, a $94,000 charge for the service can’t be justified, Vogel says.
“You’re not going to meet anybody who believes that a hundred thousand dollars or more is reasonable for neuromonitoring,” Vogel says.
Most neuromonitoring companies charge reasonable fees for a valuable service and are upfront about their ownership and financial arrangements, he says. But some companies are greedy and submit huge bills to an insurance company, hoping they won’t be challenged, he adds.
Even worse, “some neuromonitoring groups charge excessive fees in order to gain business by paying the money back to surgeons,” Vogel says.
Last year, Vogel’s group published a position statement condemning these “kickback arrangements” and other unethical business practices.
It is unclear whether Traxx, the company that provided neuromonitoring for Cannon, has any financial arrangements with surgeons. Cannon’s surgeon did not respond to requests for comment.
The size of the fee for Cannon’s neuromonitoring was only part of the problem. The other part was that Traxx — unlike her hospital, surgeon and anesthesiologist — had no contract with Blue Cross and Blue Shield of Texas.
As an out-of-network provider, the company could set its own fees and try to collect from Cannon any amount it didn’t get from her insurer.
Blue Cross and Blue Shield of Texas said it doesn’t comment on problems affecting individual members. But the insurer did offer a general statement by email about the problem:
“Unfortunately, non-contracted providers can expose our members to significantly greater out-of-pocket costs. These charges often have no connection to underlying market prices, costs or quality. If given the opportunity, we will try to negotiate with the provider to reduce the cost.”
One thing working against Cannon is that she is pretty sure that just before surgery, she signed a paper that authorized the out-of-network neuromonitoring.
“It was 4:30 in the morning and you’re like, ‘OK, let’s get this over with,’ ” she recalls.
Getting consent in the hospital may be legal, but it’s not reasonable, says Dr. Arthur Garson Jr., who directs the Health Policy Institute at the Texas Medical Center in Houston.
For example, a patient might be having a heart attack, Garson says. “You got chest pain, you’re sweating, sick as you can be, and they hand you a piece of paper and they say, ‘Sign here.’ “
The Texas Legislature passed a bill in May to protect patients from the sky-high bills this practice can produce. And Congress is considering similar legislation.
These are small steps in the right direction, Garson says.
“Asking the individual patient to make that decision even when they’re not sick, I think, is difficult,” he says, “and maybe we ought to think of some better way to do it.”
The Texas legislation is expected to take effect later this year but affects only bills that occur after it becomes law. So that $94,000 figure is never far from Cannon’s mind, even as she and Chiumento plan their wedding.
“Every time I go out and I collect the mail, I’m wondering, ‘Is this the day it’s going to show up and we’re going to have to deal with this?’ ” she says.
The takeaway: Neuromonitoring during complex surgery involving the spine can help prevent inadvertent damage. But monitoring may be unnecessary for lower-risk back operations, like spinal fusion.
It is strange that neuromonitoring is charged as a separate service, rather than part of the spine surgery. Cardiac monitoring is not charged separately during bypass surgery, for example.
When considering spine surgery, ask your doctor whether neuromonitoring will be part of the procedure. If so, will it be billed separately? Try to find out the name of the provider and get an estimate of the cost beforehand.
Check with your insurer to determine if the neuromonitoring provider is within your network and to make sure the estimated charge will be covered.
Attorneys Unveil Plan For National Settlement Of Lawsuits From Opioid Epidemic

Attorneys who represent hundreds of local governments have a new proposal for how to deal with the opioid crisis. They unveiled the framework for nationwide settlement in federal court on Friday.
MARY LOUISE KELLY, HOST:
All right, attorneys representing hundreds of local governments around the country met this morning in Ohio. They unveiled a plan they hope will lead to a national settlement of lawsuits stemming from the opioid epidemic. Tens of billions of dollars are at stake. A lot of that money could go to helping people struggling with addiction, but big hurdles remain before the drug industry agrees to major payouts.
North Country Public Radio’s Brian Mann reports.
BRIAN MANN, BYLINE: The motion was filed in a federal court in Ohio by a team of attorneys who represent 1,200 counties, cities and towns that all say they need money to help respond to the opioid epidemic. One of those attorneys, Joe Rice, says they’ve been trying to reach a settlement with two dozen drugmakers and distributors that sold opioid medications. But during negotiations over the last year, companies haven’t signed on.
JOE RICE: The defendants don’t have a sense of how they get closure. How can they put this issue behind them? And with the whole country involved, it’s a difficult question.
MANN: The problem, says Richard Ausness, a professor at the University of Kentucky who follows opioid litigation, is that if companies like Purdue Pharma and McKesson settle for billions of dollars with one group of towns and cities, they could still face other litigation. What the drug industry wants, he says, is a deal that brings closure.
RICHARD AUSNESS: Because obviously they don’t want too many outliers suing them after they’ve settled with the majority. And this proposed settlement seems to anticipate that and try to provide for as much of a global settlement as is possible.
MANN: The plan unveiled today doesn’t include the dollar amounts for a settlement or a formula for who would pay. Negotiations haven’t gotten that far. What this plan does is lay out a deal where roughly 24,000 local governments would all be swept into a single group that could settle with drug companies together. Those communities would get to vote on any proposed payout. They could also opt out of the arrangements altogether. But attorney Joe Rice says he hopes for a lot of buy-in if this plan is approved by the court.
RICE: This is an attempt to bring a organizational load to the municipalities around the country in order they can speak with a voice.
MANN: This kind of closure and clarity could be an important bargaining chip because local governments hope for massive compensation, payouts that would rival the big tobacco settlements of the 1990s.
RICE: Tens of billions of dollars would be needed to make a significant – a real significant impact on this epidemic.
MANN: Attorneys for two of the drug companies involved in this lawsuit describe the proposal as interesting but preliminary. They said they haven’t had time to work through the details of how it would work. Some companies are also still reluctant to admit wrongdoing. Johnson & Johnson is facing a state civil trial right now in Oklahoma, accused of improperly marketing opioid products. Earlier this year, Jennifer Taubert, CEO of Johnson & Johnson’s Janssen division, testified before Congress, insisting the company isn’t responsible for the prescription opioid epidemic.
(SOUNDBITE OF ARCHIVED RECORDING)
JENNIFER TAUBERT: Everything that we have done with our products when we promoted opioid products, which we stopped marketing a long time ago, was very appropriate and responsible.
MANN: Joe Rice, attorney with the plaintiffs group that filed the motion today, says he doesn’t think this proposed settlement framework will resolve all opioid litigation against Big Pharma. But he does think it might allow companies or groups of companies to now come forward and cut a deal.
RICE: I think that the distributors could potentially all get on the same page. I think the manufacturers could potentially get on the same page.
MANN: The judge overseeing the consolidated federal opioid case in Ohio, Dan Polster, has been pushing for the parties to reach a settlement. So far, that’s been elusive, but sources tell NPR the creation of this new framework was one of the steps the court asked for to help make a final deal possible. Brian Mann, NPR News.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Architecture For Possible Nationwide Opioid Settlement Unveiled

Updated at 4:20 p.m. ET
Attorneys for local governments across the country unveiled a plan Friday that they say would move the nation closer to a global settlement of lawsuits stemming from the deadly opioid crisis.
Final payouts could rival the massive tobacco settlements of the 1990s. Such a deal, if reached, could funnel tens of billions of dollars to communities struggling with the opioid addiction crisis, while restoring stability to one of the country’s biggest industries.
“There has got to be a comprehensive approach to addressing the national epidemic, and this is a step toward that,” said Joe Rice, co-lead council for attorneys who filed the motion, representing hundreds of the communities suing Big Pharma.
He said the framework, which attorneys filed in federal court in Ohio and still needs approval by the court, could help more than 24,000 communities across the U.S. fight the opioid crisis. None of the defendant companies, which are facing a tsunami of litigation stemming from the epidemic, have signed off on the framework yet.
“The defendants don’t have a sense of how they get closure, how can they put this issue behind them,” Rice said. “So they have asked us for a roadmap.”
In all, more than 1,800 lawsuits have been filed so far against drugmakers such as Johnson & Johnson, distributors like McKesson and street-corner pharmacies including CVS and Walmart. (Note: Walmart is one of NPR’s financial supporters.)
Plaintiffs claim the companies earned billions in profit by aggressively marketing and selling prescription opioids.
Richard Ausness, a professor at the University of Kentucky who follows opioid litigation, says unless some kind of structure like this is created, companies could settle for billions of dollars with one group of towns and cities but still face other lawsuits.
“Obviously they don’t want too many outliers suing them after they’ve settled with the majority,” Ausness told NPR. “This proposed settlement seems to anticipate that and provide for as much of a global settlement as possible.”
Attorneys for two of the drug companies involved in this lawsuit described the proposal as interesting but preliminary. The attorneys, who asked not to be named because they had not been authorized to speak publicly, said they haven’t had time to work through the details of how it would work.
Overdoses tied to prescription pain pills have killed more than 200,000 Americans, according to the Centers for Disease Control and Prevention, and cost taxpayers billions of dollars.
The wave of civil suits has already forced one drugmaker, Insys Therapeutics, into bankruptcy. Another major firm, Purdue Pharma, has indicated they may follow suit. Judge Dan Polster, who is overseeing a trial of hundreds of consolidated opioid cases, has repeatedly urged communities and companies to reach a deal.
That hasn’t happened yet. But intense negotiations are continuing, and sources tell NPR they expect many of the two dozen drug industry firms involved in the consolidated Ohio case to agree to some kind of substantial payout. In the end, there may be multiple settlements, involving separate companies or groups of companies, all contributing to a national fund designed to ease the opioid epidemic.
“Tens of billions of dollars would be needed to make a real significant impact on this epidemic,” Rice told NPR.
Under this plan, nearly every community in the U.S. — cities, towns, villages and counties — would be swept into a single “negotiating class.” Under that legal designation, local leaders would be able to approve or disapprove any settlements reached with drug companies. The vote would be weighted by population.
If three-quarters of communities sign off on deals that are struck, it would be finalized and money would be paid out, ending the company’s liability. A separate emergency fund, roughly 15% of any settlements would be set aside for towns or cities particularly hard-hit by the opioid crisis. And 10% of all drug industry payouts would go to pay the hundreds of private trial attorneys involved in the litigation.
Communities that don’t want to be part of any global settlement can also opt out entirely, but Rice says this plan was developed in consultation with many of the local officials and legal teams around the U.S. that are suing the drug industry.
Meanwhile, pressure has been growing on drug companies in recent months to reach some kind of accord with communities. In March, Purdue Pharma settled with the state of Oklahoma for roughly $270 million. Before its bankruptcy, Insys Therapeutics agreed to pay the federal government more than $225 million in penalties tied to opioid marketing. Five of that company’s executives were convicted of federal racketeering charges. Johnson & Johnson is currently on trial in Oklahoma state court.
With the much larger Ohio case set to begin in October, public scrutiny and pressure will only grow. Judge Polster has refused to dismiss claims against drug firms, and he’s made it clear he feels the drug industry is partly to blame for the opioid epidemic.
During a hearing in preliminary January 2018, Polster urged the parties to reach a deal that would “get some amount of money to the government agencies for treatment. Because sadly every day more and more people are being addicted, and they need treatment.”
Why Air Ambulance Bills Are Still Sky-High

In many rural areas, helicopters are the only speedy way to get patients to a trauma center or hospital burn unit. As more than 100 rural hospitals have closed around the U.S. since 2010, the need for air transport has only increased.
Ollo/Getty Images
hide caption
toggle caption
Ollo/Getty Images
In April 2018, 9-year-old Christian Bolling was hiking with his parents and sister in Virginia’s Blue Ridge Mountains, near their home in Roanoke. While climbing some boulders, he lost his footing and fell down a rocky 20-foot drop, fracturing both bones in his lower left leg, his wrist, both sides of his nose and his skull.
A rescue squad carried him out of the woods, and a helicopter flew him to a pediatric hospital trauma unit in Roanoke.
Most of Christian’s care was covered by his parents’ insurance. But one bill stood out. Med-Trans, the air ambulance company, was not part of the family’s health plan network and billed $36,000 for the 34-mile trip from the mountain to the hospital. It was greater than the cost of his two-day hospitalization, scans and cast combined.
“When you’re in that moment, you’re only thinking about the life of your child,” says Christian’s mother, Cynthia Bolling, an occupational therapist. “I know I’m being taken advantage of. It’s just wrong.”
The rising number of complaints about surprise medical bills is spurring efforts on Capitol Hill and at the White House to help consumers. Over and over again, the high cost associated with air ambulance service gives patients the biggest sticker shock — the subject has come up at nearly every Capitol Hill hearing and news conference on surprise medical bills.
Yet air ambulance costs are not addressed in any of the proposals introduced or circulating in Congress. Even a congressional decision last year to set up a panel that would study air ambulance billing hasn’t gone anywhere.
“We’re doing a disservice to patients if we protect them from hospital bills but bankrupt them on the way there,” said James Gelfand, senior vice president for health policy for the ERISA Industry Committee, a trade association for large employers.
The issue came up again Wednesday at a House Energy and Commerce subcommittee hearing where Rick Sherlock, president and CEO of the Association of Air Medical Services (the industry group for air ambulances), was among eight witnesses.
Rep. Ben Ray Luján, D-N.M., sharply questioned Sherlock as to why costs for air ambulance services have risen by 300% in his state since 2006.
“I’m trying to get my hands around why this is costing so much and why so many of my constituents are being hit by surprise bills,” Luján said.
Sherlock explained that reimbursements from Medicare and Medicaid do not cover the cost of providing services. So charges to private patients, he told the legislators, must make up that difference.
Air ambulances serve more than 550,000 patients a year, according to industry data, and in many rural areas, air ambulances are the only speedy way to get patients to trauma centers and burn units. As more than 100 rural hospitals have closed around the U.S. since 2010, the need has increased for air services.
More than 80 million people can get to a Level 1 or 2 trauma center within an hour only if they’re flown by helicopter, according to Sherlock.
The service, though, comes at a cost. According to a recent report from the Government Accountability Office, two-thirds of the more than 34,000 air ambulance transports examined were not in the patients’ insurance networks. That can leave patients on the hook for the charges that their insurers don’t cover, a practice known as balance billing.
In 2017, the GAO found that the median price charged nationally by air ambulance providers was around $36,400 for helicopter rides and even higher for other aircraft. The total generally includes the costs for both the transportation and the medical care aboard the aircraft.
Additionally, the Bill of the Month investigative series by NPR and Kaiser Health News has received more than a dozen such bills, ranging from $28,000 to $97,000.
Cynthia Bolling says her insurance company paid about a third of Christian’s air ambulance bill, and the family settled this week with Med-Trans, agreeing to pay $4,400 out of pocket.
Reid Vogel, director of marketing and communications for Med-Trans, says he can’t discuss a particular patient’s case because of privacy rules. But, he adds, Med-Trans works with patients to find “equitable solutions” when their bills are not covered by insurance.
Since nearly three-quarters of flights are for patients insured by low-paying Medicare, Tricare and Medicaid, he says, “providers must shift costs to insured patients.”
Yet private insurers usually will pay only an amount close to what Medicare reimburses, which is around $6,500. That gives air ambulance companies an incentive to remain out of network, according to a 2017 GAO report.
“A representative from a large independent provider noted that being out of network with insurance is advantageous to the provider because a patient receiving a balance bill will ask for a higher payment from the insurance company, which often results in higher payment to the air ambulance provider than having a pre-negotiated payment rate with the insurer,” the GAO found in its report.
Sherlock, of the air transport trade association, disputes the report’s findings, saying his members are actively trying to be in network in more places, although he can’t provide any specific numbers.
“I think that everywhere they can, they’re incentivized to be in network,” he says.
States are hampered in their efforts to ease the strain for residents.
The Airline Deregulation Act of 1978, which was intended to encourage more competition, prohibits states from regulating prices for any air carrier, including air ambulances. What’s more, many large employers’ health insurance is not governed by states but regulated by the federal labor law known as ERISA.
So a remedy likely has to come from Congress. And it has proved to be a heavy lift.
For example, the committees that deal with regulation of the air industry — the Commerce Committee in the Senate and the Transportation Committee in the House — don’t make health policy or regulate health insurance.
Last year, some lawmakers sought to let states regulate air ambulances with a provision in the bill reauthorizing the Federal Aviation Administration.
But that measure was ultimately eliminated. Instead, the bill called for the creation of an advisory committee to study air ambulance prices and surprise bills.
“The air ambulance lobby did a very good job playing defense during FAA authorization,” says Gelfand.
The panel, which was supposed to be formed within 60 days of the law’s enactment date — Oct. 5, 2018 — still has not been created.
Representatives from the air ambulance industry don’t think congressional action is necessary, although they are calling for higher reimbursements from Medicare.
Chris Eastlee, vice president for government relations at the Association of Air Medical Services, says his group does not favor more congressional regulation of prices but would support mandatory disclosure of costs to the secretary of the Department of Health and Human Services. Greater transparency, Eastlee’s group argues, will help companies negotiate more in-network contracts.
A fix for surprise bills that is supported by some researchers and advocates would require every health care provider within a medical facility to accept any insurance plan that contracts with that hospital. It might also help bring down air ambulance bills, says Loren Adler, associate director of USC-Brookings Schaeffer Initiative for Health Policy.
It would avoid the situation where someone picks an in-network hospital only to find out that a surgeon or anesthesiologist at that hospital doesn’t take the patient’s insurance. Air transport should also be included in the rule, Adler says.
“It’s the exact same situation as with the out-of-network emergency facility rates,” Adler says. “The same solutions should apply.”
Gelfand suggests also that the House Ways and Means Committee require air ambulance companies seeking to participate in Medicare to always charge in-network rates.
That would require only a small tweak of the legislative language, as Gelfand sees it. “Every proposal that includes something to address surprise bills for emergency care, all you [would] have to do is add in the words ‘air ambulances,’ ” he says.
Right now, the closest any surprise-billing proposal has come to addressing air ambulances is a draft legislative plan on medical costs from Sen. Lamar Alexander, R-Tenn., and Sen. Patty Murray, D-Wash.
Their plan would require that bills for air ambulance trips be itemized to show both medical charges and the transportation charges — so patients and health plans can understand them better.
Kaiser Health News is a nonprofit, editorially independent program of the Kaiser Family Foundation. KHN is not affiliated with Kaiser Permanente.
How One Father Became A Leading Activist In The Fight Against Opioids
When Greg McNeil’s son Sam died of a heroin overdose in 2015, after first becoming addicted to prescription pain pills, the father reinvented himself as an opioid activist.
Ban On Abortion Funding Stays In House Bill As 2020 Democrats Promise Repeal

Presidential candidate and former Vice President Joe Biden publicly switched his position on the Hyde Amendment under pressure from other Democrats.
Charlie Neibergall/AP
hide caption
toggle caption
Charlie Neibergall/AP
Democrats on the 2020 campaign trail are emphasizing their support for expanded abortion rights, but in Washington, House Democrats are preparing to retain a decadeslong ban on most federal funding for abortions.
Presidential candidates from Sen. Elizabeth Warren to former Vice President Joe Biden and Sen. Kamala Harris have all denounced the funding restrictions under what is known as the Hyde Amendment. Harris has said it targets poor women who rely on federal health care benefits, Warren says she would “lead the fight to have it overturned” and Biden now says that backing Hyde violates his belief that health care is a human right.
But these Democrats, along with most Democrats who served in Congress since the provision was attached regularly to spending bills, have a history of voting for spending bills that include the Hyde Amendment.
The House is set to vote Thursday on a bill that would extend the prohibition for at least another year. That is creating extra tension for the more than one dozen Democrats who are splitting time between campaigning for their party’s nomination and legislating in a politically divided Washington.
Origin of Hyde Amendment
Named for its author, Illinois Republican congressman Henry Hyde, the 1976 vote was a response to Roe v. Wade, the landmark Supreme Court decision legalizing abortion, which was decided three years earlier.
At the time, Democrats had a wide majority in the House. More than 100 Democrats voted for the amendment when it came up for a standalone vote, providing more than half of the support for the addition to that year’s labor and health bill.
Since then, it has been baked into annual spending bills. This year it is part of a broad package that funds the departments of Labor and Health and Human Services as well as the departments of defense, energy and state.
Democratic leaders blame divided government
House Speaker Nancy Pelosi, D-Calif., is one of many abortion rights supporters in Congress who have resigned themselves to supporting spending bills that include the Hyde restrictions.
“I do not think it is good public policy, and I wish we never had a Hyde Amendment, but it is the law of the land right now,” Pelosi told an audience this week at an event sponsored by the Peter G. Peterson Foundation. “I don’t see that there is an opportunity to get rid of it with the current occupant of the White House and some in the United States Senate.”
The health portion of the House Democrats’ first major spending bill is loaded with several major Democratic priorities, including more than $2 billion for Alzheimer’s research and more than $3 billion to fight AIDS.
That’s why leaders tamped down an effort by freshman Massachusetts Democratic Rep. Ayanna Pressley to strip the Hyde Amendment from this year’s funding bill.
House Progressive Caucus Co-Chair Pramila Jayapal, D-Wash., told reporters this week that she wishes Hyde didn’t exist. She explained that the party is now overwhelmingly in favor of abortion rights and most members would prefer to get rid of Hyde, but spending bills need bipartisan support to avoid another government shutdown.
“You know, we are where we are,” Jayapal said. “People don’t want to throw that into an appropriations bill that has to go to a Republican Senate and be signed by a Republican president.”
The view from the campaign trail
Democrats in Congress acknowledge that presidential candidates have to take a stand. Biden was recently forced to come out against Hyde after abortion rights supporters — and other Democratic candidates — attacked the former vice president for publicly backing the ban.
House Democratic Caucus Chairman Hakeem Jeffries, D-N.Y., said a number of the candidates running for president are in the same position as Biden.
“I believe that every single candidate for president who served in either the House or the Senate — every single one of them — voted for an appropriations bill that contains the Hyde Amendment,” Jeffries said at a press conference.
The list includes Harris, Biden, Warren and nearly a dozen other candidates.
But not all candidates accept that framing. In an interview this week with The NPR Politics Podcast, Harris said supporting spending bills isn’t the same as supporting Hyde.
“Let’s be clear, I’ve not voted for the Hyde Amendment,” Harris said. “The Hyde Amendment is the law. And so it has been attached to other funding bills, and until we repeal it, which is what I am in favor of, it will be attached to federal government funding bills. That’s the problem with the Hyde amendment.”
Federal Grants Restricted To Fighting Opioids Miss The Mark, States Say

Drug agents last fall worked with a Minneapolis police SWAT team to seize just under 171 pounds of methamphetamine. Many U.S. states say they face an escalating problem with meth and drugs other than opioids.
Cannon River Drug and Violent Task Force/AP
hide caption
toggle caption
Cannon River Drug and Violent Task Force/AP
In his 40 years of working with people who struggle with addiction, David Crowe has seen various drugs fade in and out of popularity in Pennsylvania’s Crawford County.
Methamphetamine use and distribution is a major challenge for the rural area, says Crowe, the executive director of Crawford County Drug and Alcohol Executive Commission. And opioid-related overdoses have killed at least 83 people in the county since 2015, he says.
Crowe says his organization has received just over $327,300 from key federal grants designed to curb the opioid epidemic. While the money was a godsend for his county, he says methamphetamine remains a major problem.
And here’s the hitch: Crawford County, which lies south of Lake Erie, on the Ohio state line, can’t use the federal opioid grants to treat meth addiction.
“Now I’m looking for something different,” Crowe says. “I don’t need more opiate money. I need money that will not be used exclusively for opioids.”
The federal government has doled out at least $2.4 billion in state grants since 2017, in hopes of stemming an opioid epidemic that killed 47,600 people in the U.S. in that year alone.
But state officials note that drug abuse problems seldom involve only one substance. And while local officials are grateful for the funding, the grants can be spent only on creating solutions to combat opioids, such as prescription OxyContin, heroin and fentanyl.
According to the most recent data from the Centers for Disease Control and Prevention, 11 states — including California, Pennsylvania and Texas — have reported that opioids were involved in fewer than half of their total drug overdose deaths in 2017.
Also, the federal cash infusion is guaranteed for only a few years, which throws the sustainability of the states’ efforts into question. Drug policy specialists say the money may not be adequate to improve the mental health care system. And more focus is needed on answering the underlying question of why so many Americans struggle with drug addiction, they say.
“Even just the moniker — ‘the opioid epidemic’ — out of the gate, is problematic and incorrect,” says Leo Beletsky, an associate professor of law and health sciences at Northeastern University in Boston. “This was never just about opioids.”
States have received the federal funds for opioids primarily through two grants: State Targeted Response to the Opioid Crisis and State Opioid Response. The first grant, authorized by the 21st Century Cures Act, totaled $1 billion. The second pot of money, $1.4 billion (approved as part of last year’s omnibus spending bill), sets aside a portion of the funding for states with the most drug poisoning deaths.
For Ohio and Pennsylvania, the need was great. Nearly 4,300 and 2,550 residents, respectively, died from opioid-related overdoses in the two states in 2017. Ohio was awarded $137 million in grants; Pennsylvania, $138.1 million.
State officials say the federal money enabled them to invest significantly in programs like training medical providers on addiction, offering more points of access for treatment and providing interventions for special populations, such as pregnant women.
The grants also stipulate a minimum amount of money for every state, so even areas with reportedly low opioid-related overdose death rates now have considerable funds to combat the crisis. Arkansas, for example, reported 188 opioid-related deaths in 2017 and received $15.7 million from the federal government.
Statistics show 2,199 people in California died from opioid-related causes in 2017, though its opioid death rate was one of the 10 lowest in the country. The Golden State received $195.8 million in funding — more than any other state.
“This funding is dedicated to opioids,” said Marlies Perez, a division chief at the California Department of Health Care Services, “but we’re not blindly just building a system dedicated just to opioids.”
Mounting evidence points to a worrisome rise in methamphetamine use nationally. The presence of cheap, purer forms of meth in the drug market coupled with a decline in opioid availability has fueled the stimulant’s popularity.
The number of drug overdose deaths involving meth tripled from 2011 to 2016, the CDC reports.
And hospitalizations involving amphetamines — the class of stimulants that includes methamphetamine — are spiking.
The problem of meth addiction is hard to address, doctors say. Treatment options for this addiction are narrower than the array available for opioids. In light of the increase in deaths related to other substances, are these restricted grants the best way to fund states’ response to opioids?
Bertha Madras, a professor of psychobiology at Harvard Medical School and a former member of the President’s Commission on Combating Drug Addiction and the Opioid Crisis, says the federal government has responded well by tailoring its response to opioids because those drugs continue to kill tens of thousands of Americans per year.
However, Madras adds, as more people living with addiction are identified and other drugs rise in popularity, the nation’s focus will need to change.
Beletsky emphasizes that the grants are insufficient to support fixes to the mental health care system, which must respond to patients living with an addiction of any kind.
People addicted to a particular substance typically use other drugs as well. Controlling addiction throughout a person’s life can be akin to playing whack-a-mole, says Dr. Paul Earley, president of the American Society of Addiction Medicine, because they may stop using one substance only to abuse another.
But specific addictions may also require specific treatments that cannot be addressed with tools molded for opioids, addiction specialists say, and the appropriate treatment may not be as available.
“I think we have to really begin to self-examine why this country has so much substance use to begin with,” Madras says.
Kaiser Health News is a nonprofit, editorially independent program of the Kaiser Family Foundation, and is not affiliated with Kaiser Permanente.
Rural Health: Financial Insecurity Plagues Many Who Live With Disability

Kim Ryu for NPR
Carol Burgos is worried her neighbors think she is bringing the neighborhood down.
She lives in a mobile home park in a woodsy part of Columbia County, N.Y, just off a two-lane highway. The homes have neat yards and American flags. On a spring Saturday, some neighbors are out holding yard sales, with knickknacks spread out on folding tables. Others are out doing yardwork.
Burgos’ lawn is unruly and overgrown.
“How bad do I feel when these little old ladies are mowing their lawn and I can’t because I’m in so much pain?” she says.
Burgos is in her early 50s. She can’t mow her lawn herself because of pain and physical limits related to her osteoarthritis, degenerative disk disease and other health issues. She was deemed disabled in 1997 and lives on payments from Social Security Disability Insurance. She gets health coverage through Medicare.
She also can’t afford to pay someone to mow the lawn for her. “I don’t want another bill,” she explains. “I don’t want to be in more debt. I’m embarrassed. I don’t know, who do you ask?”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Carol Burgos is deeply frustrated she can’t even physically mow her own lawn because of pain from her osteoarthritis, degenerative disk disease and other health issues.
Selena Simmons-Duffin/NPR
hide caption
toggle caption
Selena Simmons-Duffin/NPR
Burgos estimates she is $30,000 in debt. That’s a lot, especially with so little coming in. “Less than $1,500 a month,” she says. “And that doesn’t include [costs of] fuel; cooking gas; electric; water usage.”
For food, she gets a bit of money in food stamps every month. Her income works out to about $18,000 a year — not too far off from what most people living on disability benefits make.
There’s no way she could pay a $1,000 expense right away, Burgos says. According to a recent poll NPR conducted with the Robert Wood Johnson Foundation and the Harvard T.H. Chan School of Public Health, 49% of rural Americans couldn’t afford a sudden expense of that size.
The percentage was much higher — 70% — for people who, like Burgos, have disabilities. More than half of those with disabilities said their families have had problems paying for medical or dental bills in the past few years.
Burgos says she doesn’t want to have to rely on disability benefits. She used to work — she’s had lots of jobs, including helping developmentally challenged people with life skills.
She identifies as a “working person with disabilities” even though she hasn’t worked for 10 years. She is frustrated by the copays she has to pay for doctor visits and at the pharmacy — she ends up filling only her most important prescriptions, she says.
“I want to work,” she says. “Screw the money! Give me medical coverage — full medical — so I can be an able body that is willing to work.”
Burgos feels stuck in poverty and physically stuck, because it’s so hard for her to get around.
Having good access to transportation — or not — has a huge impact on the health of people living in rural parts of the country, says Dr. Kirsten Bibbins-Domingo, a professor of epidemiology and biostatistics at the University of California, San Francisco who studies the health of vulnerable populations.
“If you go to less populated areas — rural areas — access to a car that functions well [and] the costs for gas becomes such an essential element,” Bibbins-Domingo says. “Both to drive to seek medical care, as well as to drive to access the other resources that are necessary to pursue good health.”
Without that transportation — or ready access to other basics like healthy food or good housing — people can get into a vicious cycle, she says.
“Poor health contributes to financial instability and to poverty,” Bibbins-Domingo says, “and poverty itself we know contributes to poor health.”
That cycle of poor health and poverty hits people with disabilities particularly hard. “Their poverty levels are over two times higher, compared to those without disabilities,” says Bill Erickson of the Yang-Tan Institute on Employment and Disability at Cornell University.
The federal government does provide help to people with disabilities under two different programs. Some people, like Burgos, have a work history that entitles them to payments from Social Security Disability Insurance. Others, who never worked — perhaps because of a developmental disability — are eligible for Supplemental Security Income.
But other hurdles can arise. If you’re disabled, live in a rural area and want to work, you still have to find a job you can do.
“Since the Great Recession, rural counties really haven’t seen as much employment growth as urban counties,” Erickson says. “Also just the types of jobs that are available to those sorts of communities may be tending toward, you know, requiring people to be able to move things physically or whatever.
“And the limitations that the individual with disabilities may have,” Erickson continues, “may be preventing them from being able to do those particular types of jobs — or employers can’t provide the accommodations that may be necessary.”
Erickson’s colleague at ILR, Thomas Golden, adds that the complexity of disability benefits presents another problem for people who would like to work. It’s not clear to many people how much they are allowed to work without jeopardizing their benefits, he says, or what programs are available to help them in the job search.
For the past six years, Golden and Erickson have worked with young people receiving Supplemental Security Income as part of the New York State PROMISE initiative.
“In a lot of cases, those youth and their families weren’t ready to talk about work because they couldn’t pay their rent,” Golden says. “Or they were getting evicted. Or other basic needs needed to be met first before they could think about their own self-development, when it came to work and economic independence.”
Burgos says she would like to find a job she is able to do, with enough hours to supplement her income but not trigger a loss of her Social Security benefits. First, though, she says, she must figure out how to deal with the overgrown lawn and a student loan bill that just arrived in the mail. And she is trying to coordinate nursing care for her elderly mother.
There are good things in her life, too, Burgos says. She has her faith — she’s a born-again Christian. Her car is a bit beat up, but it works. And she has a very sweet little dog.
And even though she has to rely on a walker for long distances — and fears she eventually will end up in a wheelchair — for now, she is still well enough to get up and down the stairs to her front door.
NPR science intern Susie Neilson contributed reporting for this story.