Reports Find Health Workers Still Aren’t Alerting Police Regarding Likely Elder Abuse

Two reports from the federal government have determined that many cases of abuse or neglect of elderly patients that are severe enough to require medical attention are not being reported to enforcement agencies by nursing homes or health workers — even though such reporting is required by law.
Mary Smyth/Getty Images
hide caption
toggle caption
Mary Smyth/Getty Images
It can be hard to quantify the problem of elder abuse. Experts believe that many cases go unreported. And Wednesday morning, their belief was confirmed by two new government studies.
The research, conducted and published by the Office of Inspector General of the U.S. Department of Health and Human Services, finds that in many cases of abuse or neglect severe enough to require medical attention, the incidents have not been reported to enforcement agencies, though that’s required by law.
One of the studies focuses solely on the possible abuse of nursing home residents who end up in emergency rooms. The report looks at claims sent to Medicare in 2016 for treatment of head injuries, body bruises, bed sores and other diagnoses that might indicate physical abuse, sexual abuse or severe neglect.
Gloria Jarmon, deputy inspector general for audit services, says her team found that nursing homes failed to report nearly 1 in 5 of these potential cases to the state inspection agencies charged with investigating them.
“Some of the cases we saw, a person is treated in an emergency room [and] they’re sent back to the same facility where they were potentially abused and neglected,” Jarmon says.
But the failure to record and follow up on possible cases of elder abuse is not just the fault of the nursing homes. Jarmon says that in five states where nursing home inspectors did investigate and substantiate cases of abuse, “97 percent of those had not been reported to local law enforcement as required.”
State inspectors of nursing homes who participated in the study appeared to be confused about when they were required to refer cases to law enforcement, Jarmon notes. One state agency said that it only contacted the police for what it called “the most serious abuse cases.”
Elder abuse occurs in many settings — not just nursing homes. The second study looked at Medicare claims for the treatment of potential abuse or neglect of older adults, regardless of where it took place. The data was collected on incidents occurring between January of 2015 and June of 2017.
The federal auditors projected that, of more than 30,000 potential cases, health care providers failed to report nearly a third of the incidents to law enforcement or Adult Protective Services, even though the law requires them make such reports.
“It’s very important that the first person who notices this potential abuse and neglect reports it, because then they can begin the investigative process to determine if abuse or neglect occurred,” says Jarmon. “And if it’s not reported, it can’t be tracked.”
The HHS report says that Medicare could do a better job of analyzing the data it has on hand. It recommends that the Centers for Medicare and Medicaid Services, which oversees the health care program for older Americans, should periodically examine claims for treatment, looking for diagnoses that suggest possible abuse or neglect, as well as where and when those cases occur.
“You have to be able to get the data to see how bad the problem is,” says Jarmon, “so that “everybody who can take action has it.”
However, the Centers for Medicare and Medicaid Services, which pays for much of the health care for seniors, and provides guidance on the reporting required of health care workers and health care facilities, has rejected most of the reports’ recommendations.
CMS declined NPR’s request for an interview, but in a written response, it argues that it can take up to a year for Medicare claims to be filed. So analyzing such claims, CMS says, would “not be [a] timely enough” way to identify and respond to cases of elder abuse and neglect.
The inspector general’s report counters that the vast majority of Medicare claims are filed within a month, not a year. And Gloria Jarmon says that just letting state agencies and health care providers know that they’re being tracked, could reduce the problem of elder abuse.
‘Patients Will Die’: One County’s Challenge To Trump’s ‘Conscience Rights’ Rule

Caiaimage/Sam Edwards/Getty Images
Moral and religious objections to providing health care sometimes arise in medicine: A medical assistant might not agree with blood transfusions. A nurse might not want to assist in sex reassignment surgery.
Last month, the U.S. Department of Health and Human Services put out a new rule that “implements full and robust enforcement” of existing laws that protect what the administration calls “conscience rights” for health care workers. The rule is set to go into effect on July 22.
As NPR has previously reported, the new rule expands the kinds of workers who are covered by those laws — to include, for example, reception and billing staff. Even though relatively few of these complaints get submitted to HHS each year, this emphasis on religious freedom has been a hallmark of the department under the Trump administration.
HHS was sued right away over the expansiveness of its new rule — by the states of New York and California and by physician groups, clinics and others.
Santa Clara County in California is asking a federal judge in U.S. District Court, Northern District of California this week to put the Trump rule on hold while the legal process plays out — San Francisco and the state of California filed separate motions for preliminary injunctions last week.
To succeed in putting a temporary stop on the rule, at least one of the plaintiffs will need to convince a judge that implementing the rule would cause “irreparable harm.”
So what’s the harm of a rule designed to affirm health workers’ right to exclude themselves from providing medical care that they say violates their religious or moral beliefs?
“If the rule goes through as it’s written, patients will die,” says Santa Clara’s county executive, Jeff Smith, who is a physician as well as an attorney by training.
“We will have a guaranteed situation where a woman has had a complication of an abortion, where she’s bleeding out and needs to have the services of some employee who has moral objections,” Smith predicts. “That patient will die because the employee is not providing the services that are needed.”
Santa Clara has 2 million residents — it is more populous than 14 states, according to 2017 census data. The county runs three hospitals, including a Level 1 trauma center, clinics and pharmacies, all of which rely in part on federal funding to operate.
The issue is not whether employees who have moral objections to providing certain kinds of care should have a way to opt out, according to James Williams, county counsel for Santa Clara. The county already has a policy to deal with that, but it differs from the federal rule in two key ways.
“One: Health care providers need to notify us in advance,” Williams says. “It can’t just be an on-the-fly objection. And that makes sense because, how are you supposed to run a hospital if you don’t know what your staff has a concern about until the actual procedure needs to happen? And second: There’s an exception for dealing with an emergency situation.”
HHS declined to offer comment for this story, because litigation regarding its rule is ongoing. But the department summarized and responded to nearly a quarter-million comments that were submitted during the 60-day public comment period after the rule was first proposed in January 2018.
In response to commenters who raised the emergency issue, HHS said its final rule does not explicitly conflict with federal laws that require health workers to provide emergency treatment for any and all patients.
To this, Santa Clara County counsel Williams responds, “What the [federal] rule doesn’t do is actually say that it doesn’t apply in emergencies.”
If the conscience rule does go into effect, and Santa Clara does not comply with it, the federal funding the county relies on to operate its public health system could be withheld or subject to “funding claw-backs to the extent permitted by law,” according to the HHS rule.
On the other hand, Williams says, if the county attempted to comply with the rule, it would have another problem — figuring out how.
“HHS didn’t explain or consider how this rule would actually be implemented in practice,” Williams says. “The rule kind of suggests that, basically, you need to have extra staffing to accommodate the fact that there may be people who have objections. That would be very costly.”
County officials worry more broadly about the direct impact of the federal rule on patients. In the lawsuit, Santa Clara argues that the rule could delay care, which could, among other things, open the county up to malpractice suits.
And, county officials add, posting notice about the “conscience rights” policy, as the HHS rule instructs, in “a prominent and conspicuous physical location” within hospitals and clinics that receive federal funding could scare away vulnerable patients — including women seeking abortions or transgender patients.
To this last point, HHS wrote in its rule: “The Department disagrees that a notice of federal conscience and anti-discrimination laws would in any way discourage a patient seeking emergency treatment.”
This is not the first time Santa Clara County has sued the Trump administration — the county also sued over Trump’s attempts to undermine DACA and over the administration’s legal threats against sanctuary cities.
The county has had its eye on the conscience rights issue since the rule was proposed in 2018. When the final rule came down in May 2019, Santa Clara was ready to go.
“We have, as a county, more flexibility to litigate because we have a county Board of Supervisors that’s very supportive of patients’ rights,” says Smith, the county executive. “But every county, every public health system, will have the same concerns.”
Trump administration officials say the federal rule is necessary to protect health workers’ religious freedom. As NPR has reported, Roger Severino, the director of HHS’s Office for Civil Rights, has made the right of health workers to refuse to offer care for religious reasons to some patients his signature issue. In a statement sent to NPR, Severino vowed to “defend the rule vigorously.”
The next step: A judge in U.S. District Court will decide whether any of the California plaintiffs pass the test for preliminary injunctive relief — that if the rule goes into effect, they will suffer “irreparable harm.”
If any or all plaintiffs pass that test, the judge could put the rule on hold while the lawsuits play out. Currently, challenges to the rule in New York and San Francisco are both scheduled for hearings on July 12 — just days before the federal rule is set to go into effect.
How Safe Is Sunscreen And How Much Should We Wear?

NPR’s Audie Cornish talks with Trisha Calvo of Consumer Reports about a study that finds the active ingredients in sunscreen may be absorbed into the bloodstream.
Expert Panel Recommends Wider Use Of Daily Pill To Prevent HIV Infections

In 2012, the Food and Drug Administration approved the use of Truvada to prevent HIV infection in people at high risk.
Justin Sullivan/Getty Images
hide caption
toggle caption
Justin Sullivan/Getty Images
The U.S. Preventive Services Task Force has a new recommendation aimed at preventing HIV infections and AIDS. The influential panel’s guidance says people at high risk of being infected with HIV should be offered preventive antiretroviral medications — taken in a daily pill.
There’s lots of evidence that preexposure prophylaxis — also known as PrEP — is effective. The Food and Drug Administration-approved pill Truvada contains two antiretroviral medicines (tenofovir and emtricitabine).
The Centers for Disease Control and Prevention cites evidence that PrEP can reduce the risk of HIV infection by up to 92% in people who are at high risk and who take the drug consistently.
The CDC recommended PrEP several years ago and calls it “a powerful HIV prevention tool,” but so far uptake of PrEP has been slow.
“Currently, less than 10% of individuals with an indication for PrEP are receiving this medication,” write Hyman Scott and Paul Volberding in an editorial published Tuesday alongside the new recommendation in the medical journal JAMA. Both authors are physicians and researchers at the University of California, San Francisco who have been involved in HIV research.
“The gap between indication and use is most pronounced among black and Latino men who have sex with men,” Volberding and Scott write.
And the new recommendation “should serve to promote policies to expand PrEP access to those at risk,” they conclude.
People at high risk of HIV infection include those who inject drugs and those who have sex without condoms when they don’t know the HIV status of their high-risk partner.
Many insurers already pay for Truvada, but the task force’s recommendation could be influential in expanding coverage of the drug, whose list price runs $21,360 a year.
“The cost of the medication is absolutely a barrier for a lot of people in the U.S.,” Scott said in an interview. “We have patients who go to the pharmacy and are told they have to pay $1,300 or $1,600 for their month’s supply of Truvada.”
Many at-risk people can get the drug at a reduced cost or at no cost, depending on their insurance. “We try to educate patients to let them know there are many programs to help offset the costs,” Scott says.
“We’ve done a good job in medicine at being able to treat HIV, in the sense it’s now become a chronic disease for most people … but we still have a problem with new HIV infections,” says John Epling, a physician and professor of family and community medicine at Virginia Tech and a member of the U.S. Preventive Services Task Force. The goal is to prevent these infections.
More than 38,000 new HIV cases were diagnosed in the U.S. in 2017, according to the CDC. “So, we need for primary care clinicians to engage in offering PrEP to their high-risk patients,” Epling says.
The task force’s recommendation is published with a new review of the evidence, including an analysis of multiple studies evaluating the safety and effectiveness of PrEP.
The studies found that most side effects, including gastrointestinal complaints and some nausea, were mild and reversible. Another side effect in some people taking Truvada is elevated creatinine, a measure of kidney function, so patients on the drug are monitored periodically.
The review finds that the therapy significantly reduces the risk of acquiring HIV infection compared with a placebo, although effectiveness drops when people fail to take the pill daily.
“PrEP is highly effective at preventing HIV acquisition,” Epling says, “if it’s taken every single day and condoms are used.”
Oregon’s Criminal Justice System To Be Examined Over Treatment Of Mentally Ill People
Some Oregon inmates with mental illness are in jail rather than a state mental health hospital. A federal judge will hear arguments Tuesday that Oregon is not providing timely, appropriate care.
Storytelling Helps Hospital Staff Discover The Person Within The Patient

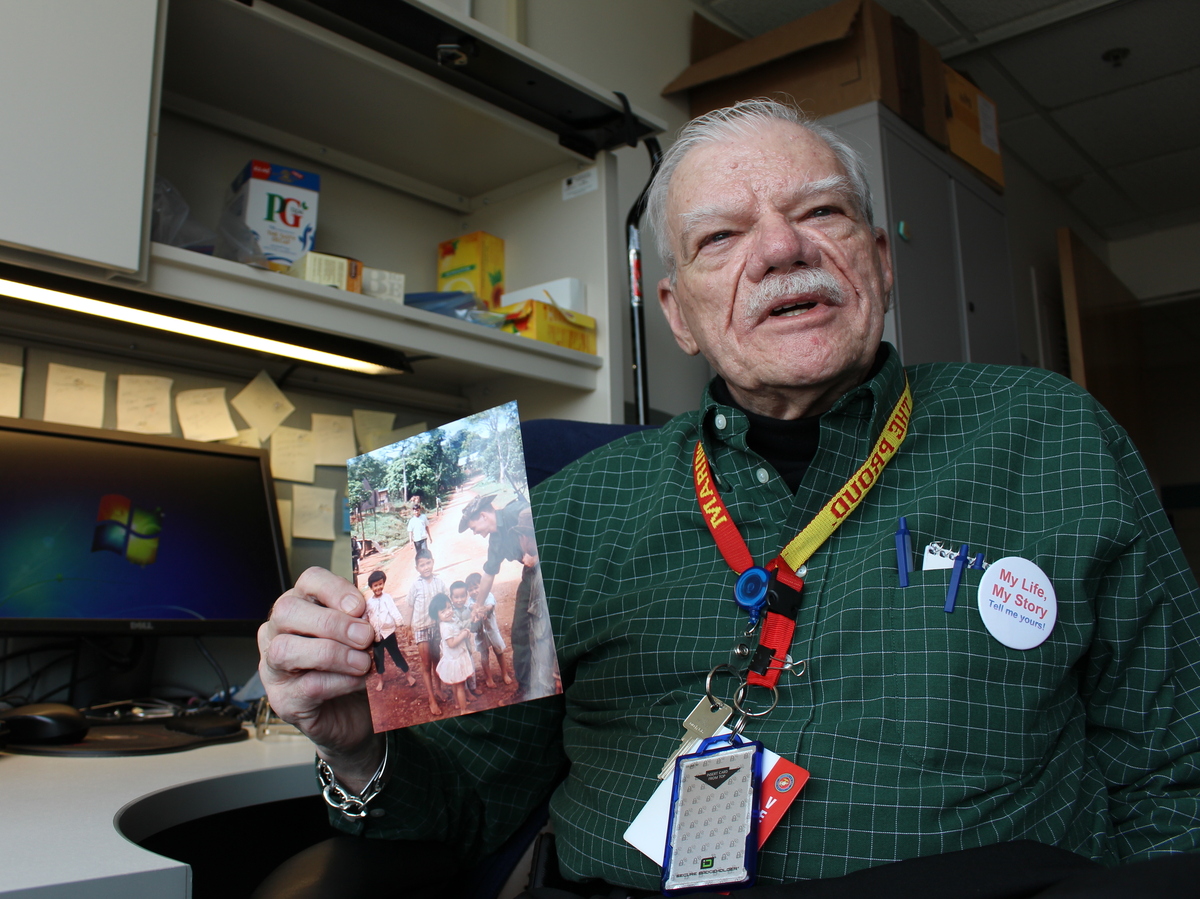
Thor Ringler (right) interviewed Ray Miller (left) in Miller’s hospital room at the William S. Middleton Memorial Veterans Hospital in Madison, Wis., in April. Miller’s daughter Barbara (center) brought in photos and a press clipping from Miller’s time in the National Guard to help facilitate the conversation.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Bob Hall was recovering from yet another surgery when the volunteer first walked into his hospital room. It was March 2014, and unfortunately Hall had been in and out of the hospital quite a bit. It had been a rocky recovery since his lung transplant, three months earlier, at the William S. Middleton Memorial Veterans Hospital in Madison, Wis.
But the volunteer wasn’t there to check on his lungs or breathing. Instead she asked Hall if we wanted to tell his life story.
Hall was being treated at the VA because he had served in the Marine Corps during the Vietnam War. After the war, he had a political career as a Massachusetts legislator, and then led professional associations for 30 years.
Hall, who was 67 at the time, welcomed the volunteer and told her he’d be happy to participate.
“I’m anything but a shy guy, and I’m always eager to share details about my life,” Hall says, half-jokingly.
He spoke to the volunteer for more than an hour about everything — from his time as “a D student” in high school (“I tell people I graduated in the top 95 percent of my class”) to his time in the military (“I thought the Marines were the toughest branch and I wanted to stop the communists”). He finished his story with a description of his health problems — those that that finally landed him in the hospital, and many that continue to the present day.
The interview was part of a program called My Life, My Story. Volunteer writers seek out vets like Hall in the hospital, and ask them about their lives. Then they write up this life story, a 1,000-word biography, and go over it with the patient, who can add more details or correct any mistakes.
“Of course, being a writer I rewrote the whole thing,” Hall confesses with a smile.
Once the story is finished, it’s entered into to the patient’s electronic medical record, so any doctor or nurse working anywhere in the VA system who opens the medical record can read it.
Hall was one of the earliest patients interviewed for the project, back in 2014. Today more than 2,000 patients at the Madison VA have shared their personal life stories.
Project organizers say My Life, My Story could change the way providers interact with patients at VA hospitals around the country.

Bob Hall was one of the earliest patients to be interviewed for the My Life, My Story program at the VA hospital in Madison, Wisc. “I’d never experienced something like that in a hospital before,” Hall says.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR

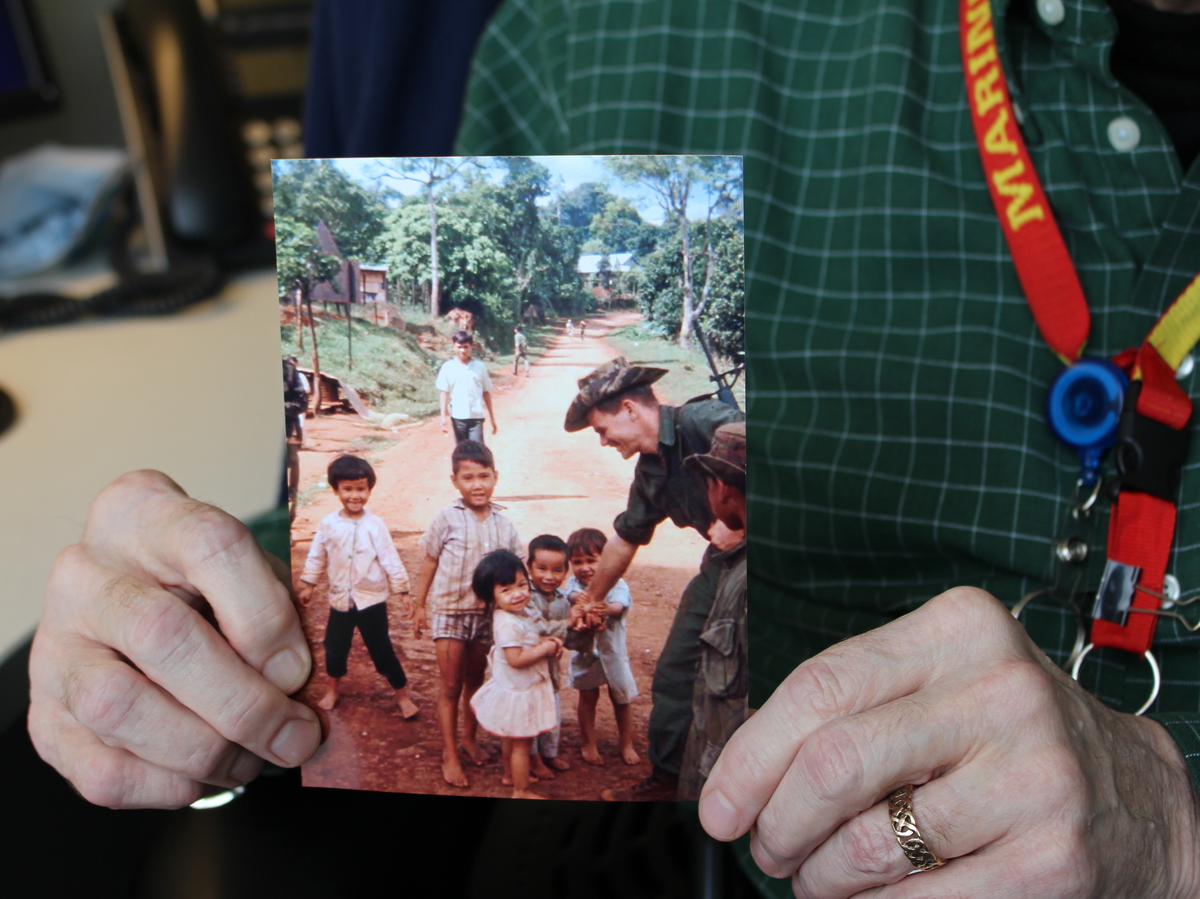
A close-up of Hall’s photograph of his conversation with children in a Vietnamese village. He served in the Marine Corps during the Vietnam War — an important part of his personal story.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Personalizing impersonal records
“If you’re a health care person, if you’re someone who is in the [electronic medical] record all the time, you’ll know that the record is a mess,” says Thor Ringler, who has managed the My Life, My Story project since 2013.
Clinicians can get access to a lot of medical data through a patient’s electronic medical record, but there’s nowhere to learn about a patient’s personality, or learn about her career, passions or values, Ringler says.
“If you were to try to get a sense of someone’s life from that record, it might take you days,” Ringler says.
The idea for My Life, My Story came from Dr. Elliot Lee, a medical resident who was doing a training rotation at the Madison VA in 2012. The typical rotation for medical residents lasts only about a year, so Lee wanted to find a way to bring these new, young doctors quickly up to speed on the VA patients. He wanted a way for them to absorb not just their health histories, but more personal information, like their hobbies, and which hospital staffers knew them best.
“It seemed to make sense that the patient might know a lot about themselves, and could help provide information to the new doctor,” Lee recalls.
But the question remained: What was the best way to get patients to share these details, to get their life stories into the records? Lee says he and some colleagues tried having patients fill out surveys, which were useful but still left the team wanting more. Next, they tried getting patients to write down their life stories themselves, but not many people really wanted to. Finally, an epiphany: Hire a writer to interview the patients, and put what they learned on paper.
It wasn’t hard to find a good candidate: A poet in Madison, Thor Ringler, had also just finished his training as a family therapist. He was good at talking to people, and also skilled at condensing big thoughts into concise, meaningful sentences.
“Of course!” Ringler remembers thinking. “I was made for that!'”

Thor Ringler has run the My Life, My Story program at the the William S. Middleton Memorial Veterans Hospital in Madison since 2013. In that time the program has recorded life stories of more than 2,000 veterans — and placed the short biographies in each vet’s’ electronic medical record.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Under Ringler’s guidance, the project has developed a set of training materials to allow other VA hospitals to launch their own storytelling programs. About 40 VA hospitals around the U.S. are currently interested, according to Ringler.
Based on his experience building the program in Madison, Ringler estimates hospitals would need to hire just one writer — working half- or full-time, depending on the hospital’s size — to manage a similar storytelling program. That means the budget could be as low as $23,000 a year. That relatively small investment can pay huge dividends in terms of patient satisfaction, Ringler says, by restoring personal connections between patients and the medical team.
“If we do good stories, people will read them, and they will want to read them,” he adds.
In addition to the interest from within the VA system, the idea has spread farther — to hospitals like Brigham and Women’s Hospital in Boston, and Regions Hospital in St. Paul, Minn.
A ‘gift’ to doctors and nurses
There is also research suggesting that when caregivers know their patients better, those patients have improved health outcomes.
One study, for example, found that doctors who scored higher on an empathy test had patients with better-controlled blood sugar. Another study found that in patients with a common cold, the cold’s duration was reduced by nearly a full day for those patients who gave their doctor a top rating for empathy.
University of Colorado professor Heather Coats studies the health impact of biographical storytelling. She notes a 2008 study found that radiologists did a more thorough job when they were simply provided a photo of the patients whose scans they were reading.
“They improved the accuracy of their radiology read,” Coats says. “Meaning [fewer] misspelled words; a better report that’s more detailed.” Current research is investigating whether storytelling might have a similar effect on clinical outcomes.
And, Coats adds, the benefits of the kind of storytelling happening at the VA don’t just accrue to the patients.
“I consider it a gift to the nurses and the doctors,” Coats says.
A survey of clinicians conducted by the Madison VA backs that up: It showed 85 percent of them thought reading the biographies of patients produced by Thor Ringler’s team of writers was “a good use” of clinical time and also helped them improve patient care.
“It gives you a much better understanding about the entirety of their life and how to help them make a decision,” says Dr. Jim Maloney, a VA surgeon who performed Bob Hall’s lung transplant in 2013.
That’s critical for doctors like Maloney, because only about half the people who undergo a lung transplant are still alive after five years. Maloney believes knowing more about a patient’s life story makes it easier for the doctor to have difficult but necessary conversations with a patient — to learn, for example, how aggressively to respond if a complication occurs.

Jim Maloney, a transplant surgeon at the Madison VA, says being able to read a patient’s personal story, along with their medical story, helps him help them through difficult decisions. “It gives you a much better sense of the entirety of their lives,” Maloney says.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Maloney says the stories generated by My Life, My Story give the entire transplant team near immediate access to a valuable tool, one that helps them connect quickly with patients and family members, and start conversations about sensitive issues or difficult choices about end-of-life care.
Dr. Tamara Feingold-Link has also experienced the power of being able to read a patient’s life story. Now a second-year medical resident at Brigham and Women’s Hospital in Boston, Feingold-Link first encountered one of the biographies generated by My Life, My Story when she was on rotation at a Boston-area VA. Her attending physician asked her to run a meeting with a patient’s family.
“I barely knew the patient, who was so sick he could hardly talk,” Feingold-Link recalls.
She noticed his medical record included the patient’s life story, something she had never seen before. She immediately read the story.
“It brought me to tears,” she remembers. “When I met his family, I could connect with them immediately.”
“It made his transfer to hospice much smoother for everyone involved,” she says.
Now Dr. Feingold-Link has started a similar program at Brigham and Women’s Hospital.
Meaningful stories go beyond medical care
Bob Hall has learned the stories can be meaningful to caregivers even when they’re not working. During one of his stays at the Madison VA, a nursing aide came into his room after she read his life story in his medical record.
“She came in one night and sat down on my bed just to talk to me for a while, because she’d read my story,” Hall says. “I found out later she wasn’t on the clock. She just came in after her shift ended to chat for a while.”
It’s been 5 years since Hall’s lung transplant, and he’s doing well. He even found a part-time job putting his writing skills to work as part of the My Life, My Story team. In just two years, Hall has written 208 capsule biographies of veterans who come to this hospital for care, just like he did.
“Dr. Maloney came to me one day recently, and I was telling him how many stories I’d done,” Halls says, “and he says, ‘You know I think you’ve given more back to the VA with these stories than they gave to you.'”
“I said, ‘Doctor, I don’t think that’s true, but it’s very kind of you to say so.’ It made me feel good.”
This story is part of NPR’s reporting partnership with Kaiser Health News.
Poll: Majority Want To Keep Abortion Legal, But They Also Want Restrictions

Georgia state Rep. Erica Thomas speaks during a protest against recently passed abortion-ban bills at the state Capitol on May 21 in Atlanta.
Elijah Nouvelage/Getty Images
hide caption
toggle caption
Elijah Nouvelage/Getty Images
Three-quarters of Americans say they want to keep in place the landmark Supreme Court ruling, Roe v. Wade, that made abortion legal in the United States, but a strong majority would like to see restrictions on abortion rights, according to a new NPR/PBS NewsHour/Marist Poll.
What the survey found is a great deal of complexity — and sometimes contradiction among Americans — that goes well beyond the talking points of the loudest voices in the debate. In fact, there’s a high level of dissatisfaction with abortion policy overall. Almost two-thirds of people said they were either somewhat or very dissatisfied, including 66% of those who self-identify as “pro-life” and 62% of those who self-identify as “pro-choice.”
“What it speaks to is the fact that the debate is dominated by the extreme positions on both sides,” said Barbara Carvalho, director of the Marist Poll, which conducted the survey. “People do see the issue as very complicated, very complex. Their positions don’t fall along one side or the other. … The debate is about the extremes, and that’s not where the public is.”
The poll comes as several states have pushed to limit abortions in hopes of getting the Supreme Court to reconsider the issue. Abortion-rights opponents hope the newly conservative court will either overturn Roe or effectively gut it by upholding severe restrictions. The survey finds that while most Americans favor limiting abortion, they don’t want it to be illegal and don’t want to go as far as states like Alabama, for example, which would ban it completely except if the woman’s life is endangered or health is at risk.
A total of 77% say the Supreme Court should uphold Roe, but within that there’s a lot of nuance — 26% say they would like to see it remain in place, but with more restrictions added; 21% want to see Roe expanded to establish the right to abortion under any circumstance; 16% want to keep it the way it is; and 14% want to see some of the restrictions allowed under Roe reduced. Just 13% overall say it should be overturned.
Loading…
Don’t see the graphic above? Click here
Even though Americans are solidly against overturning Roe, a majority would also like to see abortion restricted in various ways. In a separate question, respondents were asked which of six choices comes closest to their view of abortion policy.
In all, 61% said they were in favor of a combination of limitations that included allowing abortion in just the first three months of a pregnancy (23%); only in cases of rape, incest or to save the life of the woman (29%); or only to save the life of the woman (9%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anti-abortion demonstrators hold a protest on May 31 outside the Planned Parenthood Reproductive Health Services Center in St. Louis, the last location in the state that performs abortions.
Saul Loeb/AFP/Getty Images
hide caption
toggle caption
Saul Loeb/AFP/Getty Images
Eighteen percent said abortion should be available to a woman any time she wants during her entire pregnancy. At the other end of the spectrum, 9% said it should never be permitted under any circumstance.
More than half (53%) of Americans say they would definitely not vote for a candidate who would appoint judges to the Supreme Court who would limit or overturn Roe.
Politically, abortion has been a stronger voting issue for Republicans than for Democrats. This poll found that abortion ranks as the second-most-important issue for Republicans in deciding their vote for president, behind immigration. But for Democrats, it is fifth — behind health care, America’s role in the world, climate change and personal financial well-being.
The poll also notably found the highest percentage of people self-identifying as “pro-choice,” those who generally support abortion rights, since a Gallup survey in December 2012. In this survey, 57% identified that way versus 35%, who called themselves “pro-life,” those who are generally opposed to abortion rights.
Loading…
Don’t see the graphic above? Click here
The percentage self-identifying as “pro-choice” is an increase since a Marist Poll in February, when the two sides split with 47% each. The pollsters attribute that shift to efforts in various states to severely restrict abortion.
“The public is very reactive to the arguments being put forth by the more committed advocates on both sides of the issue,” Carvalho said, adding, “The danger for Republicans is that when you look at independents, independents are moving more toward Democrats on this issue. … When the debate starts overstepping what public opinion believes to be common sense, we’ve seen independents moving in Democrats’ corner.”
In the case of self-identification, 60% of independents identified as “pro-choice.” Asked which party would do a better job of dealing with the issue of abortion, a plurality of Americans overall chose Democrats (47%) over Republicans (34%).
Independents chose Democrats on the question of which party would do a better job by an 11-point margin (43% to 32%).
Loading…
Don’t see the graphic above? Click here
Asked if they’d be more likely to support state laws that decriminalize abortion and make laws less strict or ones that do the opposite, 60% of Americans overall, including two-thirds of independents, chose laws that decriminalize abortion and are less strict.
What specifically do Americans support and oppose?
The poll also asked a long series of questions to try to figure out what Americans support or oppose when it comes to potential changes to abortion laws pending in several states. Poll respondents were not told which states these proposals come from.
The poll found that Americans are very much against requiring fines and/or prison time for doctors who perform abortions. There was also slim majority support for allowing abortions at any time during a pregnancy if there is no viability outside the womb and for requiring insurance companies to cover abortion procedures. A slim majority also opposed allowing pharmacists and health providers the ability to opt out of providing medicine or surgical procedures that result in abortion.
At the same time, two-thirds were in favor of a 24-hour waiting period from the time a woman meets with a health care professional until having the abortion procedure itself; two-thirds wanted doctors who perform abortions to have hospital admitting privileges; and a slim majority wanted the law to require women to be shown an ultrasound image at least 24 hours before an abortion procedure.
Loading…
Don’t see the graphic above? Click here
“What’s most interesting here,” Carvalho said, is that “the extremes are really outliers. When they advocate for their positions and change the debate toward the most extreme position on the issue, they actually do the opposite. They move public opinion away from them.”
The more vocal advocates on either side, however, have had the ability to shift the debate and public opinion to their point of view. Consider that many of the specific items above, at one point or another, have been hotly debated.
When does life begin?
The poll also asked the very big question of when Americans think life begins. There was not an overwhelming consensus. A plurality of the six choices given, but far less than a majority, said life begins at conception (38%). Slightly more than half (53%) disagreed, saying that life begins either within the first eight weeks of pregnancy (8%), the first three months (8%), between three and six months (7%), when a fetus is viable (14%) or at birth (16%).
Loading…
Don’t see the graphic above? Click here
Gender gap? Try a stark party divide, particularly among women
The most acute divide among Americans on the issue of abortion, arguably, is not a gender divide but between the parties — and of women of different parties.
For example, 54% of men identified as “pro-choice,” compared with 60% of women. For women of the different parties, 77% of Democratic women identified as “pro-choice,” while 68% of Republican women identified as “pro-life.” (A lower percentage of Republican men, 59%, considered themselves “pro-life.”)
Throughout the poll, the divide was stark. On Roe, for example, 62% of Republican women said overturn it or add restrictions; 73% of Democratic women said keep it the way it is, expand it to allow abortions under any circumstance or reduce some of the restrictions.
Eighty-four percent of Democratic women said they are more likely to support state laws that decriminalize abortion and make laws less strict; 62% of Republican women said they are more likely to support laws that criminalize abortion or make laws stricter.
On requiring insurance companies to cover abortion procedures, 75% of Democratic women support that, while 78% of Republican women oppose it, higher than the 63% of Republican men who said the same.
Republican women also stand out for the 62% of them who said they oppose laws that allow abortion at any time during pregnancy in cases of rape or incest. They are the only group to voice majority opposition to that. Fifty-nine percent of Republican men, for example, said they would support such a law.
And Republican women are the only group to say overwhelmingly that life begins at conception. About three-quarters said so, compared with less than half of Republican men and a third of Democratic women.
It’s a reminder that Republican women, in many ways, are the backbone of the movement opposing abortion rights.
The survey of 944 adults was conducted by live interviewers by telephone from May 31 through June 4. It has a margin of error of plus or minus 4.5 percentage points.
Editor’s note: The survey asked respondents to identify as either “pro-life” or “pro-choice.” This question wording, using the labels “pro-life” and “pro-choice,” was included in the survey because it has tracked the public debate on abortion over decades. It is sensitive to current events and public discussion even though it does not capture the nuanced positions many people have on the issue.
‘Mental Health Parity’ Is Still An Elusive Goal In U.S. Insurance Coverage

{kind=link}
The best help for patients struggling with addiction, eating disorders or other mental health problems sometimes includes intensive therapy, the evidence shows. But many patients still have trouble getting their health insurers to cover needed mental health treatment.
Gary Waters/Ikon Images/Getty Images
hide caption
toggle caption
Gary Waters/Ikon Images/Getty Images
Amanda Bacon’s eating disorder was growing worse. She had lost 60% of her body weight and was consuming only about 100 calories a day.
But that wasn’t sick enough for her Medicaid managed-care company to cover an inpatient treatment program. She was told in 2017 that unless she weighed 10 pounds less — which would have put her at 5-foot-7 and 90 pounds — or was admitted to a psychiatric unit, she wasn’t eligible for coverage.
“I remember thinking, ‘I’m going to die,’ ” the Las Cruces, N.M., resident recalls.
Eventually, Bacon, now 35, switched to a plan that paid for treatment, although she says it was still an arduous process getting the services approved.
Many patients, like Bacon, struggle to get insurance coverage for their mental health treatment, even though two federal laws were designed to bring parity between mental and physical health care coverage. Recent studies and a legal case suggest serious disparities remain.
The 2008 Mental Health Parity and Addiction Equity Act required large group health plans that provide benefits for mental health problems to put that coverage on an equal footing with physical illness. Two years later, the Affordable Care Act required small-group and individual health plans sold on the insurance marketplaces to cover mental health services, and do so at levels comparable with medical services. (In 2016, parity rules were also applied to Medicaid managed-care plans, which cover the majority of people in that federal-state health program for low-income residents.)
The laws have been partially successful. Insurers are no longer permitted to write policies that charge higher copays or deductibles for mental health care, nor can they set annual or lifetime upper-limits on how much they will pay for such care. But advocates for patients say insurance companies still interpret mental health claims more stringently than those for physical illness.
“Insurance companies can easily circumvent mental health parity mandates by imposing restrictive standards of medical necessity,” says Meiram Bendat, a lawyer leading a class-action lawsuit against a mental health subsidiary of UnitedHealthcare.
In a closely watched ruling, a federal court in March sided with Bendat and patients who alleged the insurer was deliberately shortchanging mental health claims. Chief Magistrate Judge Joseph Spero of the U.S. District Court for the Northern District of California ruled that United Behavioral Health wrote its guidelines for treatment much more narrowly than common medical standards, covering only enough care to stabilize patients “while ignoring the effective treatment of members’ underlying conditions.”
UnitedHealthcare works to “ensure our products meet the needs of our members and comply with state and federal law,” says spokeswoman Tracey Lempner.
Several studies, though, have found evidence of disparities in insurers’ decisions.
Growing gap in coverage in hospitals
In February, researchers at the Congressional Budget Office reported that private insurance companies are paying 13% to 14% less for mental health care than Medicare does.
The insurance industry’s own data show a growing gap between coverage of mental and physical care in hospitals and skilled nursing facilities. For the five years ending in 2017, out-of-pocket spending on inpatient mental health care grew nearly 13 times faster than all inpatient care, according to inpatient data reported in February by the Health Care Cost Institute, a research group funded by the insurance companies Aetna, Humana, UnitedHealthcare and Kaiser Permanente. (Kaiser Health News is not affiliated with Kaiser Permanente.)
And a 2017 report by the actuarial firm Milliman found that an office visit with a therapist is five times as likely to be out-of-network, and thus more expensive, than a primary care appointment.
In this environment, only half of the nearly 8 million children who have been diagnosed with depression, anxiety or attention deficit hyperactivity disorder receive treatment, according to a February research letter in the medical journal JAMA Pediatrics. Fewer than 1 in 5 people with substance use disorder are treated, a national survey suggests, and, overall, nearly 6 in 10 people with mental illness get no treatment or medication, according to the National Institute Of Mental Health.
Amanda Bacon, who is still receiving care for her eating disorder, remembers fearing that she wouldn’t get treatment. She was at one point rushed to an emergency room for care, but after several days in the hospital she was sent home, no closer to getting well.
Today, because of her disability, Bacon’s primary medical insurance is through Medicare, which has paid for treatment that her earlier Medicaid provider, Molina Healthcare, refused. She has been treated in four inpatient programs in the past two years — twice through Presbyterian Centennial Care, a Medicaid plan she switched to after Molina, and twice though her current Medicare plan. Bacon is also enrolled in a state-run Medicaid plan.
Molina says it can’t comment on Bacon’s case. “Molina complies with mental health parity laws,” say spokeswoman Danielle Smith, and it “applies industry-recognized medical necessity criteria in any medical determinations affecting mental health.”
The ‘wrong criteria’
Dr. Eric Plakun, CEO of the Austen Riggs Center, a psychiatric hospital and residential program in Massachusetts, says that often insurers are “using the wrong criteria” for what makes something medically necessary. They pay enough only to stabilize a patient’s condition, Plakun says, but not enough to improve their underlying illness. He was one of the experts who testified in the case before Judge Spero in California.
Insurers say they recognize the importance of mental health care coverage and that they are complying with the law.
Cathryn Donaldson, a spokeswoman for the trade group America’s Health Insurance Plans, says the industry supports parity, but that it is also harder to prove when a mental health treatment is needed.
Compared with the data on medical and surgical care, she says, the data and standards to measure mental health care “trail far behind.” She cited a 2016 study of Minnesota hospitals, where nearly one-fifth of the time patients spent in psychiatric units occurred after they were stabilized and ready to be discharged.
“Just like doctors use scientific evidence to determine the safest, most effective treatments,” insurers do the same to cover treatment “consistent with guidelines showing when and where it’s effective for patients,” Donaldson says.
Health plans commonly apply several controls that limit their coverage of mental health care. And these strategies by insurers are legal — unless they are applied more strictly for mental health care than medical care.
For example, they often require patients to try cheaper options first, a strategy called “fail first.” Patients referred by their doctors to a residential program for opioid addiction, for example, might be denied coverage by their insurers until they try — and fail — to improve at a less expensive part-time out-patient program.
Hiring doctors, nurses and pharmacists to review claims is another technique.
Dr. Frederick Villars, who reviews mental health claims for Aetna, remembers arguing with insurers to approve treatment when he was a practicing psychiatrist. His team decides what Aetna will cover based on clinical standards, he says. And providers upset about a coverage decision “are well aware of what these guidelines are.”
“It’s not a pleasant process,” Villars says, “but it’s the only tool that exists in this setting to try to keep costs under control.”
Kaiser Health News is a nonprofit, editorially independent program of the Kaiser Family Foundation. It is not affiliated with Kaiser Permanente. Graison Dangor is a journalist living in Brooklyn.
Social Security Error Jeopardizes Medicare Coverage For 250,000 Seniors

{kind=link}
Thinkstock/Getty Images
A quarter of a million Medicare beneficiaries may be receiving bills for as many as five months of premiums they thought they had already paid.
But they shouldn’t toss the letter in the garbage. It’s not a scam or a mistake.
Because of what the Social Security Administration calls “a processing error” in January, it did not deduct premiums from some seniors’ Social Security checks and it didn’t pay the insurance plans, according to the agency’s “frequently asked questions” page on its website.
The problem applies to private drug policies and Medicare Advantage plans that provide both medical and drug coverage and that substitute for traditional government-run Medicare.
Some people will discover they must find the money to pay the plans. Others may find their plans canceled. Medicare officials say approximately 250,000 people are affected.
Medicare and Social Security say they expect that proper deductions and payments to insurers will resume this month or next. Insurers are required to send bills directly to their members for the unpaid premiums, according to Medicare.
But neither agency would explain how the error occurred or provide a more exact number or the names of the plans that were shortchanged. The amount the plans are owed also wasn’t disclosed. A notice to beneficiaries on Medicare’s website lacks key details.
Rep. Richard Neal, D-Mass., who chairs the Ways and Means Committee, and two colleagues wrote to both agencies about the problem on May 22 but have not received a response from Medicare. Social Security’s response referred most questions to Medicare officials.
Organizations that help seniors say they are getting some questions from Medicare beneficiaries.
Two seniors in Louisiana lost drug coverage after their policies were canceled due to the SSA error, says Vicki Dufrene, director of the state’s Senior Health Insurance Information Program. One woman had the same drug plan since 2013, which dropped her at the end of April. She was without coverage for the entire month of May until earlier this week, when Dufrene was able to get her retroactively re-enrolled.
Dufrene says some people might not notice that their checks did not include a deduction for their Medicare Advantage or drug plan premiums. If their check was a little more than expected, they could have assumed that extra amount was the expected cost-of-living increase, among other things.
In Ohio, a Medicare Advantage plan reinstated a member due to unpaid premiums less than 48 hours after the state’s health insurance information program for seniors got involved, says director Christina Reeg.
Medicare beneficiaries have had the option of paying their premiums through a deduction from their Social Security checks for more than a decade, she says. However, they can also charge payments directly to a credit card or checking account instead of relying on Social Security.
Humana spokesman Mark Mathis says about 33,000 members were affected — or fewer than 1% of its total Medicare membership. None of those members lost coverage. The company blamed Medicare’s nearly 15-year-old IT systems for the failure and urged the agency to invest in new equipment.
A UnitedHealthcare representative says none of its 32,000 Medicare Advantage or Part D members affected by the SSA problem lost coverage. The company has the highest Medicare enrollment in the U.S.
Aetna has not received payments for Medicare Advantage and drug plans for the months of February through May for 43,000 affected members, says spokesman Ethan Slavin. Customers will receive bills for the unpaid premiums and can set up payment plans if they can’t pay the entire amount.
These and other affected insurers must allow their members at least two months from the billing date to pay. And they must offer a payment plan for those who can’t pay several months of premiums at once, Medicare says. With both steps, “plans can avoid invoking their policy of disenrollment for failure to pay premiums while the member is adhering to the payment plan,” Jennifer Shapiro, the acting director for the Medicare Plan Payment Group, warned the companies in a May 22 memo.
Lindsey Copeland, federal policy director for the Medicare Rights Center, an advocacy group, says she is concerned that older adults will view the bill with suspicion.
“If you think your premiums are being paid automatically and then your plan tells you six months later that wasn’t the case, you may be confused,” she says.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Contact Susan Jaffe at Jaffe.KHN@gmail.com or @susanjaffe
Former German Nurse Guilty Of Killing 85 Patients In Serial Murder Case

{kind=link}
Former nurse Niels Högel was found guilty of killing patients in his care by injecting them with drugs and then trying to resuscitate them. He’s seen here in court, awaiting his verdict in Oldenburg, Germany.
Hauke-Christian Dittrich/AFP/Getty Images
hide caption
toggle caption
Hauke-Christian Dittrich/AFP/Getty Images
Updated at 1:32 p.m. ET
Former nurse Niels Högel — who has admitted to giving potentially lethal drugs to patients so he could try to resuscitate them — has been sentenced by a German court to life in prison for murdering 85 people.
“Your guilt is unimaginable,” Oldenburg district court Judge Sebastian Bührmann said as he sentenced Högel, according to Deutsche Welle. “The human mind struggles to take in the sheer scale of these crimes.”
It’s the latest judgment in what the local police chief in Oldenburg has called a “horrifying” serial killer case. Högel is already serving a life sentence for killing two patients.
The disgraced nurse’s victims ranged in age from 34 to 96, according to the district court in Oldenburg. Högel was found to have injected them with a variety of drugs that included the heart medicines ajmaline, amiodarone and sotalol, along with potassium and the anesthetic lidocaine.
As the scope of Högel’s crimes became clear, authorities exhumed dozens of bodies to test them for the cocktail of drugs he had administered to his victims. The true extent of his killings may never be known — in some cases, the bodies of people who died under Högel’s care already had been cremated.
He was initially accused in a handful of deaths but was discovered to have been involved in dozens more. In the current case, Högel had been charged with committing 100 murders between early 2000 and the middle of 2005, but prosecutors were unable to prove he was responsible for 15 of those deaths.
The former nurse carried out the killings to gain attention at two different jobs: in an Oldenburg medical clinic and a hospital in Delmenhorst. While he admitted to inducing cardiac arrest in scores of patients, there were so many victims that in some instances, he said he simply couldn’t recall details about the people who died. In others, he denied playing a role.
“I feel like an accountant of death,” Judge Bührmann said Thursday, noting the scope of the crimes.
The judge’s ruling includes a notation on the “special severity” of the crimes, which will likely complicate any attempts to parole Högel after 15 years, as is common for people serving life sentences in Germany.
German courts cannot impose multiple life sentences. But in a message to NPR, a representative of the court said that because of the judge’s notation, “in the end it is possible that Mr. Högel will not be released ever.”
This week, Högel offered an apology to families and others who lost loved ones. Some of those surviving relatives spoke outside of the district court today — including families of former patients whose cases remain painfully unresolved.
“That is very, very bitter,” said Frank Brinkers, according to The Associated Press. The cause of his father’s death is still unconfirmed, although Högel is suspected of playing a role. Brinkers added, “I have gone through hell, and that is hard to bear.”
As they explored the case, investigators criticized some of Högel’s colleagues, saying they could have done more to stop the nurse after noticing his irregular behavior. Some hospital employees in Delmenhorst, near Bremen, were charged with negligent manslaughter for not taking quick and decisive action to stop Högel — even after a colleague saw him inject a patient with ajmaline.
And police have complained that Högel was given a clean reference when he moved to the Delmenhorst hospital from the clinic in Oldenburg, where police said people were aware of his “abnormalities.”