Beyond 'Bumper Sticker' Slogans: 2020 Democrats Debate Details Of Medicare-For-All

Sen. Bernie Sanders, I-Vt., promotes his Medicare-for-all proposal at the 2017 Convention of the California Nurses Association/National Nurses Organizing Committee in San Francisco, Calif., an issue that is dominating the early debate in the 2020 presidential contest.
Justin Sullivan/Getty Images
hide caption
toggle caption
Justin Sullivan/Getty Images
Bernie Sanders is back, but one of his signature policies never left.
In 2015, he introduced Medicare-for-all to many Democrats for the first time. Since Sanders’ first run for president, that type of single-payer health care system has become a mainstream Democratic proposal.
Last week, Sanders launched his second presidential campaign, amid a field of presidential candidates who are trying to figure out how to position themselves around the policy. Trying to stand out from the pack, though — especially on health care — poses a problem: Differentiating yourself means getting into the details, and getting into the details can turn voters off.
Over the last few weeks, candidates have been working to show voters the daylight between their respective health care proposals.
New Jersey Sen. Cory Booker has stressed that he supports Medicare-for-all, and that he wants private insurers to have a role in that system. “Even countries that have vast access to publicly offered health care still have private health care,” he told reporters this month.
Minnesota Sen. Amy Klobuchar says she wants a public option, in the form of letting people buy into Medicaid. As for single-payer health care, she says it’s a possibility in the long-term.
Ohio Sen. Sherrod Brown, who says he’s still debating a run, also wants a sort of public option, but only for people above age 50, whom he would allow to buy in to Medicare. “I think Medicare-for-all will take a while, and it’s difficult,” he told CNN’s State of the Union.
Long story short: In a huge Democratic presidential field, health care is the first issue where candidates are really differentiating themselves.
Bumper sticker politics
“Health reform is always more popular as a bumper sticker than as a piece of legislation,” said Larry Levitt, senior vice president for health reform at the Kaiser Family Foundation.
He points to both the Obamacare and the Obamacare repeal efforts as examples — some ideas behind Obamacare, like insuring pre-existing conditions, were popular. But other aspects that proponents said were necessary to make it work, like the individual mandate, infuriated some voters, helping propel Republicans to big wins in 2010.
Likewise, the Obamacare repeal effort fired up many Republican voters, but the implications of the various repeal plans — fewer people with insurance, lack of protections for pre-existing conditions — ultimately helped doom the effort.
Medicare-for-all may prove to be yet another example of this trend, according to Levitt.
“There’s a huge political benefit for candidates to be in favor of the idea of Medicare-for-all in a primary,” he said. “But the more the details get filled in, the less popular that idea will be.”

When Sen. Bernie Sanders, I-Vt., introduced his Medicare-for-all legislation in 2017, he was joined by several other senators now seeking the 2020 Democratic presidential nomination, including Elizabeth Warren of Massachusetts, Kirsten Gillibrand of New York, Cory Booker of New Jersey and Kamala Harris of California.
JIM WATSON/AFP/Getty Images
hide caption
toggle caption
JIM WATSON/AFP/Getty Images
California Sen. Kamala Harris may be the first to face a big lesson in this. At a recent CNN town hall, host Jake Tapper asked her about her support of Sanders’ Medicare-for-all bill, which he said would “totally eliminate private insurance.”
(A quick note here: Sanders’ plan does not totally eliminate private insurance, but it would vastly diminish its role.)
Harris said that she would eliminate private insurance — but after a quick backlash, the next day clarified, with a campaign spokesman saying she also supports more incremental health care overhauls.
Polling also shows how tricky selling Medicare-for-all could be once the details come into play. A January poll from Kaiser shows that nearly 7 in 10 Americans like Medicare-for-all if they hear it will eliminate premiums and out-of-pocket costs. But that support drops to around 4 in 10 if people hear it will mean higher taxes.
Both of those things could be true of a Medicare-for-all system. But trying to sell even this basic trade-off on the campaign trail — especially this early — is tough.
At the other, more moderate end of the spectrum, Klobuchar said she’s for the broad goal of “universal health care,” and did get specific on her support of a public option. But when it comes to Medicare-for-all, she remained vague, saying it could be a possibility. Voters will almost certainly try to pin her down more on that in coming months, but for now her answer may help keep her from alienating some more liberal voters.
For many candidates, keeping health care rhetoric broad might be a smart move for now, says Nadeam Elshami, former chief of staff to House Speaker Nancy Pelosi.
“It’s okay for a candidate to say, ‘Look: This is generally what I believe in. But I’m willing to hear first and then get into specifics later, after I have a deeper discussion of this issue,'” he said.
The “socialist” threat
Progressive health care overhauls will also likely feed into one of President Trump’s main attack lines: labeling Democrats as “socialists” as a way of painting them as extreme.
“It’s a surprising development that 10 years after the passage of the Affordable Care Act and after a massive political backlash against it, and a huge effort to defend it, Democrats are in there immediately swerving so hard to an even greater government role for health care,” said Michael Steel, a Republican strategist who worked for former House Speaker John Boehner and Jeb Bush’s 2016 campaign.
Republicans know political backlash well — the backlash to their repeal efforts culminated in the GOP losing the House in 2018. Whatever criticism Trump throws Democrats’ way on health care for 2020, they will likely counter by asking him if he has his own alternative to Obamacare, having failed to fully repeal it.
Until then, Democrats will be doing similar calculations on both health care and a variety of other issues: weighing sweeping, progressive ideas that the president could try to label as “socialist” against incremental policies that might not excite liberal voters — and deciding which choice is most likely to get a Democrat into office.
Voters want sweeping health care changes …maybe
A basic tension underlies Democratic plans to overhauls the health care system: Only 1 in 3 Americans rate health care in the U.S. as “excellent” or “good,” according to Gallup. But at the same time, a large majority — 7 in 10 — view their own personal health care as “excellent” or “good.”
Which is to say, it’s easy to see how voters might want the system massively reformed. In addition, incremental changes that don’t go as far as Medicare-for-all might particularly infuriate progressive voters.
But at the same time, voters will likely bristle if that reform threatens to change their own health coverage, as some major health care overhauls, like Medicare-for-all, might do.
“There is a reason that President Obama’s signature promise on Obamacare was ‘If you like your plan, you can keep it,'” Steel said.
That promise proved untrue — some Americans saw their health care plans canceled under the new Obamacare rules, and Politifact named Obama’s statement the “lie of the year” in 2013.
Should a Democratic candidate’s health care proposal similarly threaten people’s current health plans, it’s a safe bet that it will become a major Republican line of attack.
Planned Parenthood President Leana Wen On Trump Administration Title X Changes

NPR’s Lulu Garcia-Navarro talks with Leana Wen, a physician and the president of Planned Parenthood, about how a rule change from the Trump administration on Title X will affect her organization.
LULU GARCIA-NAVARRO, HOST:
Planned Parenthood, long the target of social conservatives, could lose a significant portion of its funding under a new Trump administration rule released on Friday. The rule will cut federal funding from organizations that make referrals for abortions or provide the procedure. This is a win for anti-abortion activists who pressured lawmakers to defund organizations with ties to abortion.
But critics say it will hurt lower-income women who depend upon family planning centers that receive what are known as Title X funds. Leana Wen is a physician and the president of Planned Parenthood, and she joins us now.
Welcome to WEEKEND EDITION.
LEANA WEN: Thank you, Lulu – good to be with you.
GARCIA-NAVARRO: You call these changes to the Title X program a gag rule. Explain.
WEN: This is a gag rule because what President Trump is doing is to put a gag on doctors like me to prevent us from providing our patients with full and accurate medical information. So if you are a woman who goes to a health center that receives public funding, you cannot be referred to abortion care, even if your life depends on it. This gag rule is unethical and unconscionable.
I mean, imagine if the Trump administration issued a rule that forbid doctors from telling our patients about their options for any other aspect of health care. It’s a direct interference with the practice of medicine and with our ethical obligation to our patients. And this is why over 100 medical and public health organizations oppose the gag rule, including the American Medical Association, the American Nurses Association and the American College of Obstetricians and Gynecologists.
GARCIA-NAVARRO: I’ve read that you won’t accept funds under the new rules.
WEN: Planned Parenthood will never force our doctors and nurses to compromise their ethics. We will never let politicians censor our health care providers and erode the trust that our patients have placed in us, which is to provide them with compassionate, judgment-free and comprehensive care. That’s our promise to our patients.
GARCIA-NAVARRO: But you could receive federal funds if you separated abortion services from family planning centers. The new rules say there needs to be clear physical and financial separation between government-funded services and abortion-related services.
WEN: This Title X gag rule isn’t about providing good medical care. It only does one thing, which is to restrict patients’ access to reproductive health care. It has no basis in medicine or science. And the only effect is going to be preventing 4 million Americans from receiving basic health care, including breast and cervical cancer screenings, affordable birth control and STI tests.
GARCIA-NAVARRO: Religiously affiliated groups are hoping to get the money instead. Conservatives say this provides good alternatives to women.
WEN: We should talk about what is evidence-based, science-based methods for ensuring that all people have access to the health care that they need. Title X is our nation’s program for affordable birth control and health care. And this program is intended to ensure that people with low incomes who live in rural areas or who don’t have health insurance still have access to cancer screenings and preventive care.
And I think it’s important to talk about the individuals who it will affect the most. It will disproportionately affect those who already face the greatest barriers to care. It’s women of color and families of low income. And we need to talk about the discrimination involved here because if you are wealthy and you have private insurance, you can still get the best medical care.
GARCIA-NAVARRO: But religious groups say they could provide those alternatives, that they feel like they too deserve these funds so that there isn’t a monopoly on care.
WEN: Look. I’m a doctor and a scientist. And I need to do what’s best for my patients based on medicine and science. And what we have done for nearly 50 years through Title X is to follow the best available medicine and science. Title X is recognized to be one of the most successful public health programs in reducing sexually transmitted infections and reducing unintended pregnancies. This is what works.
GARCIA-NAVARRO: Leana Wen is the president of Planned Parenthood. Thank you very much.
WEN: Thanks so much, Lulu. And thank you for your time.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Big Pharma Heads To Capitol Hill
The heads of the largest pharmaceutical companies will defend their pricing before the Senate next week. STAT reporter Nicholas Florko tells NPR’s Scott Simon that this will be a televised crucible.
SCOTT SIMON, HOST:
Criticism of America’s major drug companies is one of the few areas of bipartisan agreement of the U.S. Congress. Lawmakers in both parties profess to be outraged about price increases for life-saving drugs and treatments. Next Tuesday, the executives of some of the largest pharmaceutical companies in the country will go before the Senate Finance Committee. It’s expected to be a rough day for them. Nicholas Florko is the Washington correspondent for STAT, a news organization that covers health and the life sciences. He joins us in our studios. Thanks so much for being with us.
NICHOLAS FLORKO: Thanks for having me.
SIMON: Is it a little surprising they even agreed to come in?
FLORKO: Well, they really didn’t have a choice, quite frankly. If a congressional hearing – congressional committee wants to hear from you, either you come in voluntarily, or they can issue you a subpoena. And, frankly, they’re a lot nicer when you come in voluntarily.
SIMON: Can we assume the PR firms that are of counsel to all these major corporations have been working overtime to try and help them?
FLORKO: Yes, absolutely – not only PR firms but probably law firms that specialize in this as well.
SIMON: What kind of reception do you think they’re going to get?
FLORKO: It’s probably not likely that they’re going to get a friendly reception. I mean, these hearings are just as much about getting information from the drug companies as it is an opportunity for the lawmakers to make a public stand about this issue.
SIMON: I imagine no legislator thinks he or she will look very good if they say, by the way, I think price increases are great. Thank you.
FLORKO: Exactly. They realize that they are going to be on TV, the nightly news. And they want to make a point about this issue to their constituents.
SIMON: Tell us about some of the figures we’re going to be seeing – for example, Richard Gonzalez.
FLORKO: Yeah. They’re a really interesting group. So Richard Gonzalez is the CEO of the company AbbVie. Interesting company because they are not a household name, but they make a drug that’s a household name, which is Humira. You’ve probably seen the TV ads for them.
SIMON: An expensive household name.
FLORKO: Very expensive household name and on pace to be the most lucrative drug in pharmaceutical history. He is a college dropout. But he has worked his way up to CEO at AbbVie. But he’s going to face some really tough questions about these strategies the company’s used to protect this drug for so long from competition that would lower the price.
SIMON: The producer of the top-selling insulin in this country is Sanofi. I hope I’m pronouncing that correctly.
FLORKO: Yes.
SIMON: And Olivier Brandicourt.
FLORKO: That’s correct. So I call him the heel of the group because he is the one who’s going to probably face some of the toughest questions. There is bipartisan anger over the issue of insulin prices. And he is sort of No. 1 target for asking questions about why the price of insulin is so high.
SIMON: It’s essentially quadrupled for a lot of people, right?
FLORKO: That’s correct.
SIMON: Pascal Soriot of AstraZeneca.
FLORKO: So he’s my favorite of the group. My guess is if you’re going to have somebody who’s going to have a slightly embarrassing soundbite on the nightly news, it might be him. He’s kind of known for being the outspoken one, grew up in the suburbs of Paris, has talked a lot about how he used to be in fistfights as a kid. He’s actually groused to the media about how he’s the lowest paid CEO in the group, even though he makes over $12 million a year. It’s going to be interesting to see how he handles the questions that he gets.
SIMON: Whatever speeches lawmakers are going to deliver, is it a little too simplistic to hold the pharmaceutical companies responsible in and of themselves for drug prices? Because, of course, there’s a third-party payment system.
FLORKO: Yeah. I mean, it’s a super complicated area – no doubt that’s going to be the line that a lot of these companies use is you have to look at others in the supply chain. But my guess is that – obviously, the members of Congress want to hear from the drugmakers. But my guess is they want to hear from others, too. So I’d stay tuned in that round to see if there’s other hearings where we might hear from others in the supply chain.
SIMON: Pharmaceutical companies, I imagine, will also argue that you have to have, let’s say, an increasing price for insulin so they have the money to develop whatever eventually replaces insulin.
FLORKO: Of course. The issue with that argument, though – somebody like Richard Gonzalez is going to have some trouble with that because that’s a drug – his drug Humira as a reminder – that drug has been – was supposed to be eligible for generic competition a long time ago. And they’ve been accused of essentially gaming the system to keep their protection longer and longer. So the argument from lawmakers is you had your time to recoup your investment. Now it’s time to let cheaper drugs come on the market.
SIMON: Do your reportorial instincts tell you the hearing will be fair and real in attempt to discover something or just an opportunity for politicians to get soundbites?
FLORKO: It’s a little bit of both, honestly. It’s definitely going to be a show. I mean, we’ve looked at the hearings that have happened previously. You know, you had the Martin Shkreli pharma bro hearing a few years ago. And you had the EpiPen hearing about the price of that drug. There’s definitely going to be a fair bit of just grandstanding and opportunities to slam drug companies. But between the lines, these lawmakers are interested in figuring out how to legislate here. So there’ll be some interesting questions, too, that can inform legislation.
SIMON: Nicholas Florko, reporter for STAT news, thanks so much for being with us.
FLORKO: Thank you so much for having me.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Democrats Debate Health Care Policy
Vermont Sen. Bernie Sanders entered the 2020 presidential race this week as Democratic candidates engaged in their first big policy fight — centered around health care.
CVS Looks To Make Its Drugstores A Destination For Health Care

CVS plans to transform some of its stores into “health hubs,” retail locations revamped to include more health care services and products. One of the first is in Spring, Texas, a suburb of Houston.
Alison Kodjak/NPR
hide caption
toggle caption
Alison Kodjak/NPR
When it comes to making changes in health care, CVS Health isn’t settling for tinkering around the edges. The company is looking to strike at the heart of how health care is delivered in the U.S.
In November, the drugstore chain completed a $70 billion acquisition of health insurance giant Aetna that CVS has said will change the company and in the process alter the way consumers experience health care.
“We’re trying to transform the industry,” says Dr. Alan Lotvin, executive vice president for transformation for the company. The health care industry, he says, is now organized for the convenience of doctors, hospitals and other providers of care. “I think there’s an opportunity to organize around the consumer,” Lotvin says.
With almost 10,000 retail stores across the country, CVS says it is already where consumers are. Now, with the addition of Aetna, CVS also provides health coverage for 22 million people.
CVS plans to transform some of its stores and their existing retail clinics into hubs that will offer more health care services and products. The company put its first test locations in areas with lots of Aetna patients, in hopes of directing patients away from expensive emergency rooms to the stores’ less pricey MinuteClinics.
The company says this retail approach will make it easier and cheaper for people — particularly those with chronic illnesses like diabetes, heart disease or asthma — to manage their conditions.
But the company faces challenges in making the combination of an insurance company and drugstore chain work. In a statement about quarterly financial results released Wednesday, CVS CEO Larry Merlo said, “2019 will be a year of transition as we integrate Aetna and focus on key pillars of our growth strategy.”
Some of CVS’s lines of business have suffered lately, including its business supplying medicines to long-term-care facilities. CVS shares fell 8 percent Wednesday after the company posted a $2.2 billion loss for the fourth quarter and lowered its profit outlook for 2019. The pressure is on CVS to get the Aetna addition to pay off quickly.
CVS Health began talking about the idea of health care hubs in late 2017 when it launched its bid to buy Aetna. At the time, Merlo asked NPR’s Steve Inskeep to “imagine a world where [a] patient can walk into a CVS pharmac[y], they can engage with a nutritionist about their diet. They can talk to a nurse practitioner, perhaps have their blood glucose level checked, talk to their pharmacist about medication.”
But there were few details about how the company would pull it off, until now. CVS has opened three test locations in Texas, including one in the Houston suburb of Spring.
At first glance, it’s not all that different from any other CVS. There are aisles packed with candy and Band-Aids, fridges full of soda and in the back a bustling pharmacy counter.

Rosita Rodriguez uses the expanded MinuteClinic at a local CVS store to help her manage her arthritis pain and diabetes.
Alison Kodjak/NPR
hide caption
toggle caption
Alison Kodjak/NPR
But over to the side there are sliding doors with the word “WELLNESS” in giant letters, and behind them a dozen seniors are taking a free yoga class.
Rosita Rodriguez, 68, is one of them. “I did yoga,” she says. “And it was such a joy.”
She says she found out about the yoga class when she came into the store to find some painkillers for her arthritis that wouldn’t nauseate her. The store’s “care concierge,” Jesse Gonzalez, helped her choose a medication and told her about the yoga class and about how she could get her diabetes checked as well.
“Whenever I need something, I see Jesse here,” she says. “I talk to him and, you know, he’s there for me.”
Rodriguez says the store is easier to get to than her doctor’s office, which is about 20 miles away in central Houston.
The MinuteClinic here is a major department. In addition to the care concierge, there are three exam rooms, a dietitian, a respiratory therapist and a lab where people can have blood drawn.
On a recent afternoon, a patient who came to see the nurse practitioner was rushed to a nearby hospital.
“They weren’t feeling well and they were actually about to have a significant heart event,” says Kevin Hourican, president of CVS Pharmacy, who oversees the company’s entire retail operation. “So they were sent to the emergency room.”
That incident, he says, shows why it’s good to have retail clinics all over the country. About 1,000 CVS locations currently have a small version of the MinuteClinic, he says, and 85 percent of Americans live within about 4 miles of a CVS store. The need for ER care for this patient also shows the limits of what a retail clinic can do.

CVS’s health hubs, like this one in Spring, Texas, offer a wider array of health products and equipment than the company’s typical drugstore.
Alison Kodjak/NPR
hide caption
toggle caption
Alison Kodjak/NPR
To help people manage their chronic diseases, CVS will expand its services to include eye and foot exams for patients with diabetes and airflow monitoring for people with asthma.
“I see a number of upsides for patients,” says Dora Hughes, a physician and associate professor of health policy at George Washington University.
“Managing a chronic disease, I mean, that is hard work,” Hughes says. “To have CVS and their broad community footprint available, to have providers that you can see at nights and on the weekends, to be able to get your bloodwork done when you want — I mean, that could be hugely beneficial for patients.”
But Hughes says the company will do the most good only if it locates “health hubs” where there is the greatest need — where people with chronic diseases like diabetes don’t have easy access to doctors.
The company chose the locations for its first three test stores where there are a large number of patients covered by Aetna, including its commercial, Medicare and Medicaid businesses, and a lot of people with diabetes.
Another question, Hughes says, is whether CVS can communicate well with patients’ primary care doctors. Some research shows that people with a regular primary care doctor have better health in general, and some shows that people with diabetes get higher quality care from a regular primary care physician than when receiving episodic care from other doctors or nurse practitioners.
“I can see concerns that people might have that this might make that connection with the primary care home lower, says Kosali Simon, a health economist at Indiana University in Bloomington. “I now might say, ‘Maybe I don’t need to have a primary care physician that’s connected to a hospital.’ “
In fact, a survey by J.D. Power showed that 45 percent of people said they would consider getting their primary medical care at a CVS clinic. Older people were more hesitant to try a MinuteClinic, the survey shows. Only 36 percent of people 65 and over said they would go to CVS for primary care.
But Simon says, and the survey confirms, that the added convenience is likely to draw people in.
After buying Aetna, CVS expects these new clinics will help keep some Aetna patients out of the hospital and allow the insurance side of the company to avoid the high costs of hospital care.
At the same time, the expanded stores will make money treating patients at the MinuteClinic and selling an array of health care products. The store in Spring, in addition to the usual CVS products, has an aisle stocked with wheelchairs, walkers and CPAP machines that help people with sleep apnea. There are yoga equipment, snacks appropriate for people with diabetes and electronic activity monitors.
CVS says the health care services will be available to patients with any kind of insurance.
The company won’t say how many stores it plans to convert to health hubs. CVS’s Hourican says the company first wants to see how it goes in three Texas trial locations.
Insurers Hand Out Cash and Gifts To Sway Brokers Who Sell Employer Health Plans

Katherine Streeter for NPR
The pitches to the health insurance brokers are tantalizing.
“Set sail for Bermuda,” says insurance giant Cigna, offering top-selling brokers five days at one of the island’s luxury resorts.
Health Net of California’s pitch is not subtle: A smiling woman in a business suit rides a giant $100 bill like it’s a surfboard. “Sell more, enroll more, get paid more!” In some cases, its ad says, a broker can “power up” the bonus to $150,000 per employer group.
Not to be outdone, New York’s EmblemHealth promises top-selling brokers “the chance of a lifetime:” going to bat against the retired legendary New York Yankees pitcher Mariano Rivera. In another offer, the company, which bills itself as the state’s largest nonprofit plan, focuses on cash: “The more subscribers you enroll … the bigger the payout.” Bonuses, it says, top out at $100,000 per group, and “there’s no limit to the number of bonuses you can earn.”
Such incentives sound like typical business tactics, until you understand who ends up paying for them: the employers who sign up with the insurers — and, of course, their employees.
Human resource directors often rely on independent health insurance brokers to guide them through the thicket of costly and confusing benefit options offered by insurance companies. But what many don’t fully realize is how the health insurance industry steers the process through lucrative financial incentives and commissions. Those enticements, critics say, don’t reward brokers for finding their clients the most cost-effective options.
We want to hear from you.
Have you worked in health insurance? ProPublica and NPR are investigating the industry and want to hear from you. Please complete our brief questionnaire.
Here’s how it typically works: Insurers pay brokers a commission for the employers they sign up. That fee is usually a healthy 3 to 6 percent of the total premium. That could be about $50,000 a year on the premiums of a company with 100 people, payable for as long as the plan is in place. That’s $50,000 a year for a single client. And as the client pays more in premiums, the broker’s commission increases.
Commissions can be even higher, up to 40 or 50 percent of the premium, on supplemental plans that employers can buy to cover employees’ dental costs, cancer care or long-term hospitalization.
Those commissions come from the insurers. But the cost is built into the premiums the employer and employees pay for the benefit plan.
Now, layer on top of that the additional bonuses that brokers can earn from some insurers. The offers, some marked “confidential,” are easy to find on the websites of insurance companies and broker agencies. But many brokers say the bonuses are not disclosed to employers unless they ask. These bonuses, too, are indirectly included in the overall cost of health plans.
These industry payments can’t help but influence which plans brokers highlight for employers, says Eric Campbell, director of research at the University of Colorado Center for Bioethics and Humanities.
“It’s a classic conflict of interest,” Campbell says.
There’s “a large body of virtually irrefutable evidence,” Campbell says, that shows drug company payments to doctors influence the way they prescribe. “Denying this effect is like denying that gravity exists.” And there’s no reason, he says, to think brokers are any different.
Critics say the setup is akin to a single real estate agent representing both the buyer and seller in a home sale. A buyer would not expect the seller’s agent to negotiate the lowest price or highlight all the clauses and fine print that add unnecessary costs.
“If you want to draw a straight conclusion: It has been in the best interest of a broker, from a financial point of view, to keep that premium moving up,” says Jeffrey Hogan, a regional manager in Connecticut for a national insurance brokerage and one of a band of outliers in the industry pushing for changes in the way brokers are paid.
As the average cost of employer-sponsored health insurance premiums has tripled in the past two decades, to almost $20,000 for a family of four, a small, but growing, contingent of brokers are questioning their role in the rise in costs. They’ve started negotiating flat fees paid directly by the employers. The fee may be a similar amount to the commission they could have earned, but since it doesn’t come from the insurer, Hogan says, it “eliminates the conflict of interest” and frees brokers to consider unorthodox plans tailored to individual employers’ needs. Any bonuses could also be paid directly by the employer.
Brokers provide a variety of services to employers. They present them with benefits options, enroll them in plans and help them with claims and payment issues. Insurance industry payments to brokers are not illegal and have been accepted as a cost of doing business for generations.
When brokers are paid directly by employers, the results can be mutually beneficial. In 2017, David Contorno, the broker for Palmer Johnson Power Systems, a heavy-equipment distribution company in Madison, Wisconsin, saved the firm so much money while also improving coverage that Palmer Johnson took all 120 employees on an all-expenses paid trip to Vail, Colorado, where they rode four-wheelers and went whitewater rafting. In 2018, the company saved money again and rewarded each employee with a health care “dividend” of about $700.
Contorno was not being altruistic. He earned a flat fee, plus a bonus based on how much the plan saved, with the total equal to roughly what he would have made otherwise.
Craig Parsons, who owns Palmer Johnson, says the new payment arrangement puts pressure on the broker to prevent overspending. His previous broker, he says, didn’t have any real incentive to help him reduce costs. “We didn’t have an advocate,” he says. “We didn’t have someone truly watching out for our best interests.” (The former broker acknowledged there were some issues, but said it had provided a valuable service.)
Working for employers, not insurers
Contorno is part of a group called the Health Rosetta, which certifies brokers who agree to follow certain best practices related to health benefits, including eliminating any hidden agreements that raise the cost of employee benefits. To be certified, brokers (who refer to themselves as “benefits advisers”) must disclose all their direct and indirect sources of income — bonuses, commissions, consulting fees, for example — and who pays them, to the employers they advise.

David Contorno at an office in Mooresville, NC. Contorno is the founder of E Powered Benefits which is aimed at reducing the cost of healthcare coverage for employers by cutting ties between brokers and insurance companies.
Travis Dove for ProPublica
hide caption
toggle caption
Travis Dove for ProPublica
Dave Chase, a Washington businessman, created Rosetta in 2016 after working with tech health startups and launching Microsoft’s services to the health industry. He says he saw an opportunity to transform the health care industry by changing the way employers buy benefits. He says brokers have the most underestimated role in the health care system.
“The good ones are worth their weight in gold,” Chase says. “But most of the benefit brokers are pitching themselves as buyer’s agents, but they are paid like a seller’s agent.”
There are only 110 Rosetta certified brokers in an industry of more than 100,000, although others who follow a similar philosophy consider themselves part of the movement.
From the employer’s point of view, one big advantage of working with brokers like those certified by Rosetta, is transparency. Currently, there’s no industry standard for how brokers must disclose their payments from insurance companies, so many employers may have no idea how much brokers are making from their business, says Marcy Buckner, vice president of government affairs for the National Association of Health Underwriters, the trade group for health benefits brokers. And thus, she says, employers have no clear sense of the conflicts of interest that may color their broker’s advice to them.
Buckner’s group encourages brokers to bill employers for their commissions directly to eliminate any conflict of interest, but, she says, it’s challenging to shift the culture. Nevertheless, Buckner says she doesn’t think payments from insurers undermine the work done by brokers, who must act in their clients’ best interests or risk losing them. “They want to have these clients for a really long term,” Buckner says.
Industrywide, transparency is not the standard. ProPublica sent a list of questions to 10 of the largest broker agencies, some worth $1 billion or more, including Marsh & McLennan, Aon and Willis Towers Watson, asking if they took bonuses and commissions from insurance companies, and whether they disclosed them to their clients. Four firms declined to answer; the others never responded despite repeated requests.
Insurers also don’t seem to have a problem with the payments. In 2017, Health Care Service Corporation, which oversees Blue Cross Blue Shield plans serving 15 million members in five states, disclosed in its corporate filings that it spent $816 million on broker bonuses and commissions, about 3 percent of its revenue that year. A company spokeswoman acknowledged in an email that employers are actually the ones who pay those fees; the money is just passed through the insurer. “We do not believe there is a conflict of interest,” she says.
In one email to a broker reviewed by ProPublica, Blue Cross Blue Shield of North Carolina called the bonuses it offered — up to $110,000 for bringing in a group of more than 1,000 — the “cherry on top.” The company told ProPublica that such bonuses are standard and that it always encourages brokers to “match their clients with the best product for them.”
Cathryn Donaldson, spokeswoman for the trade group America’s Health Insurance Plans, wrote in an email that brokers are incentivized “above all else” to serve their clients. “Guiding employees to a plan that offers quality, affordable care will help establish their business and reputation in the industry,” she wrote.
Some insurer’s pitches, however, clearly reward brokers’ devotion to them, not necessarily their clients. “To thank you for your loyalty to Humana, we want to extend our thanks with a bonus,” says one brochure pitched to brokers online. Horizon Blue Cross Blue Shield of New Jersey offered brokers a bonus as “a way to express our appreciation for your support.” Empire Blue Cross told brokers it would deliver new bonuses “for bringing in large group business … and for keeping it with us.”
Delta Dental of California’s pitches appears to go one step further, rewarding brokers as “key members of our Small Business Program team.”
ProPublica reached out to all the insurers named in this story, and many didn’t respond. Cigna said in a statement that it offers affordable, high-quality benefit plans and doesn’t see a problem with providing incentives to brokers. Delta Dental emphasized in an email it follows applicable laws and regulations. And Horizon Blue Cross said its gives employers the option of how to pay brokers and discloses all compensation.
The effect of such financial incentives is troubling, says Michael Thompson, president of the National Alliance of Healthcare Purchaser Coalitions, which represents groups of employers who provide benefits. He says brokers don’t typically undermine their clients in a blatant way, but their own financial interests can create a “cozy relationship” that may make them wary of “stirring the pot.”
Employers should know how their brokers are paid, but health care is complex, so they are often not even aware of what they should ask, Thompson says. Employers rely on brokers to be a “trusted adviser,” he says. “Sometimes that trust is warranted and sometimes it’s not.”
Bad faith tactics
When officials in Morris County, New Jersey, sought a new broker to manage the county’s benefits, they specified that applicants could not take insurance company payouts related to their business. Instead, the county would pay the broker directly to ensure an unbiased search for the best benefits. The county hired Frenkel Benefits, a New York City broker, in February 2015.
Now, the county is suing the firm in Superior Court of New Jersey, accusing it of double-dipping. In addition to the fees from the county, the broker is accused of collecting a $235,000 commission in 2016 from the insurance giant Cigna. The broker got an additional $19,206 the next year, the lawsuit claims. To get the commission, one of the agency’s brokers allegedly certified, falsely, that the county would be told about the payment, the suit says. The county claims it was never notified and never approved the commission.
The suit also alleges the broker “purposefully concealed” the costs of switching the county’s health coverage to Cigna, which included administrative fees of $800,000.
In an interview, John Bowens, the county’s attorney, says the county had tried to guard against the broker being swayed by a large commission from an insurer. The brokers at Frenkel did not respond to requests for comment. The firm has not filed a response to the claims in the lawsuit. Steven Weisman, one of attorneys representing Frenkel, declined to comment.
Sometimes employers don’t find out their broker didn’t get them the best deal until they switch to another broker.
Josh Butler, a broker in Amarillo, Texas, who is also certified by Rosetta, recently took on a company of about 200 employees that had been signed up for a plan that had high out-of-pocket costs. The previous broker had enrolled the company in a supplemental plan that paid workers $1,000 if they were admitted to the hospital to help pay for uncovered costs. But Butler says the premiums for this coverage cost about $100,000 a year, and only nine employees had used it. That would make it much cheaper to pay for the benefit without insurance.
Butler suspects the previous broker encouraged the hospital benefits because they came with a sizable commission. He sells the same type of policies for the same insurer, so he knows the plan came with a 40 percent commission in the first year. That means about $40,000 of the employer’s premium went into the broker’s pocket.
Butler and other brokers say the insurance companies offer huge commissions to promote lucrative supplemental plans like dental, vision and disability. The total commissions on a supplemental cancer plan one insurer offered come to 57 percent, Butler says.
These massive year-one commissions lead some unscrupulous brokers to “churn” their supplemental benefits, Butler says, convincing employers to jump between insurers every year for the same type of benefits. The insurers don’t mind, Butler says, because the employers end up paying the tab. Brokers may also “product dump,” Butler says, which means pushing employers to sign employees up for multiple types of voluntary supplemental coverage, which brings them a hefty commission on each product.
Carl Schuessler, a broker in Atlanta who is certified by the Rosetta group, says he likes to help employers find out how much profit insurers are making on their premiums. Some states require insurers to provide the information, so when he took over the account for the Gasparilla Inn, an island resort on the Gulf Coast of Florida, he obtained the report for the company’s recent three years of coverage with UnitedHealthcare. He learned that the insurer had only paid out in claims about 65 percent of what the Inn had paid in premiums.
But in those same years the insurer had increased the Inn’s premiums, says Glenn Price, its chief financial officer. “It’s tough to swallow” increases to our premium when the insurer is making healthy profits, Price says. UnitedHealthcare declined to comment.
Schuessler, who is paid by the Inn, helped it transition to a self-funded plan, meaning the company bears the cost of the health care bills. Price says the Inn went from spending about $1 million a year to about $700,000, with lower costs and better benefits for employees, and no increases in three years.
A need for regulation
Despite the important function of brokers as middlemen, there’s been scant examination of their role in the marketplace.
Don Reiman, head of a Boise, Idaho, broker agency and a financial planner, says the federal government should require health benefit brokers to adhere to the same regulation he sees in the finance arena. The Employee Retirement Income Security Act, better known as ERISA, requires retirement plan advisers to disclose to employers all compensation that’s related to their plans, exposing potential conflicts.
The Department of Labor requires certain employers that provide health benefits to file documents every year about their plans, including payments to brokers. The department posts the information on its website.
But the data is notoriously messy. After a 2012 report found 23 percent of the forms contained errors, there was a proposal to revamp the data collection in 2016. It is unclear if that work was done, but ProPublica tried to analyze the data and found it incomplete or inaccurate. The data shortcomings mean employers have no real ability to compare payments to brokers.
***
About five years ago, Contorno, one of the leaders in the Rosetta movement, was blithely happy with the status quo: He had his favored insurers and could usually find traditional plans that appeared to fit his clients’ needs.
Today, he regrets his role in driving up employers’ health costs. One of his LinkedIn posts compares the industry’s acceptance of control by insurance companies to Stockholm Syndrome, the feelings of trust a hostage would have toward a captor.
Contorno began advising equipment distribution company Palmer Johnson in 2016. When he took over, the company had a self-funded plan and its claims were reviewed by an administrator owned by its broker, Iowa-based Cottingham & Butler. Contorno brought in an independent claims administrator who closely scrutinized the claims and provided detailed cost information. The switch led to significant savings, says Parsons, the company owner. “It opened our eyes to what a good claims review process can mean to us,” he says.
Brad Plummer, senior vice president for employee benefits for Cottingham & Butler, acknowledged “things didn’t go swimmingly” with the claims company. But overall his company provided valuable service to Palmer Johnson, he says.
Contorno also provided resources to help Palmer Johnson employees find high-quality, low-cost providers, and the company waived any out-of-pocket expense as an incentive to get employees to see those medical providers. If a patient needed an out-of-network procedure, the price was negotiated up front to avoid massive surprise bills to the plan or the patient.
The company also contracted with a vendor for drug coverage that does not use the secret rebates and hidden pricing schemes that are common in the industry. Palmer Johnson’s yearly health care costs per employee dropped by more than 25 percent, from about $11,252 in 2015 to $8,288 in 2018. That’s lower than they’d been in 2011, Contorno says.
“Now that my compensation is fully tied to meeting the clients’ goals, that is my sole objective,” he says. “Your broker works for whoever is cutting them the check.”
ProPublica data fellow Sophie Chou contributed to this story.
ProPublica is a nonprofit newsroom based in New York. Sign up for ProPublica’s Big Story newsletter to receive stories like this one in your inbox as soon as they are published.
How One Woman Is Working To Educate Parents On Vaccinations
Public health advocates have struggled to change the minds of these so called anti-vaxxers. But one South Carolina woman has a different approach: reaching parents before they even become parents.
ARI SHAPIRO, HOST:
An outbreak of measles in Washington and Oregon has refocused attention on parents who choose not to vaccinate their kids, often known as anti-vaxxers. Public health advocates have struggled to change these parents’ minds. One South Carolina woman has a different approach. She is reaching out to people before they even become parents. Alex Olgin of member station WFAE has the story.
ALEX OLGIN, BYLINE: In 2017, Kim Nelson had just moved her family back to her hometown in South Carolina. Moving boxes were still scattered around. While her two young daughters played, Nelson scrolled through a newspaper article on her phone. It said religious exemptions for vaccines had jumped nearly 70 percent in recent years in their part of the state, around Greenville. She yelled to her husband in the other room.
KIM NELSON: David, you have to get in here. I can’t believe this because, you know, I just – all my mom friends had vaccinated. I’d never encountered somebody who didn’t.
OLGIN: Nelson had her immunizations, and so did her kids. But this news scared her. She didn’t want anyone in her hometown to get sick. Nelson decided she had to do something.
NELSON: I very much believe that if you have the ability to advocate, then you have to. The onus is on us if we want change.
OLGIN: Like a lot of moms, Nelson had spent hours online. And she knew how easy it was to fall down an Internet hole into the world of fake studies and scary stories.
NELSON: As somebody who just cannot stand wrong things being on the Internet, if I saw something with vaccines, I was very quick to chime in, that’s not true, or no, that’s not how that works. I usually got banned.
OLGIN: Nelson started her own group for South Carolina parents. She began posting scientific articles online, but then she thought it would be best to zero in on moms that were still on the fence about vaccines.
NELSON: It’s easier to pull a hesitant parent over than it is somebody who is firmly anti-vax. They feel validated by that choice. It’s part of their community. It’s part of their identity.
OLGIN: And the most important thing was timing – reaching moms during pregnancy when they’re actually going online to figure out how to keep their babies healthy. Nelson latched onto one study that showed 90 percent of expectant women have made up their minds on vaccines by the time they were six months pregnant. After that, it’s kind of too late.
NELSON: They’re not going to a pediatrician. Their OBGYN is probably not speaking to the pediatric vaccine schedule. So where are they going? They’re going online.
OLGIN: Before parents got bad information, Nelson would be there first with facts – online, but also in person. She rented out a room at the public library and advertised on mom forums. She was nervous that the anti-vaxxers might show up.
NELSON: Are they here to rip me a new one, or are they here to learn about vaccines? And I just decided if they’re here, I’m going to give them good information.
OLGIN: Amy Morris was pregnant, but she drove an hour and a half to attend the class. It wasn’t her first pregnancy. She already had three kids. But this time around, she was nervous about vaccines. In Nelson’s class, she learned the risks of not vaccinating.
AMY MORRIS: That spoke to me more than anything.
OLGIN: Now, holding her healthy 8-month-old son Thorin on her lap, she says she’s glad she went because she was feeling vulnerable.
MORRIS: I always knew it was the right thing to do. I was listening to that fear monster in the back of my head.
OLGIN: Nelson says that fear is what the anti-vaccine community feeds on. She’s learned to ask questions to help parents get at the root of their anxiety.
NELSON: I do think they appreciate it when you meet them sympathetically, and you don’t just try to blast facts down their throat.
OLGIN: Nelson is now trying to get local hospitals to integrate that vaccine talk into their birthing classes. And she’s studying for a master’s in public health and even considering a run for office. For NPR News, I’m Alex Olgin in Greenville, S.C.
SHAPIRO: And this story is part of a partnership between NPR, Kaiser Health News and WFAE.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
White House Plan To Stop HIV Faces A Tough Road In Oklahoma

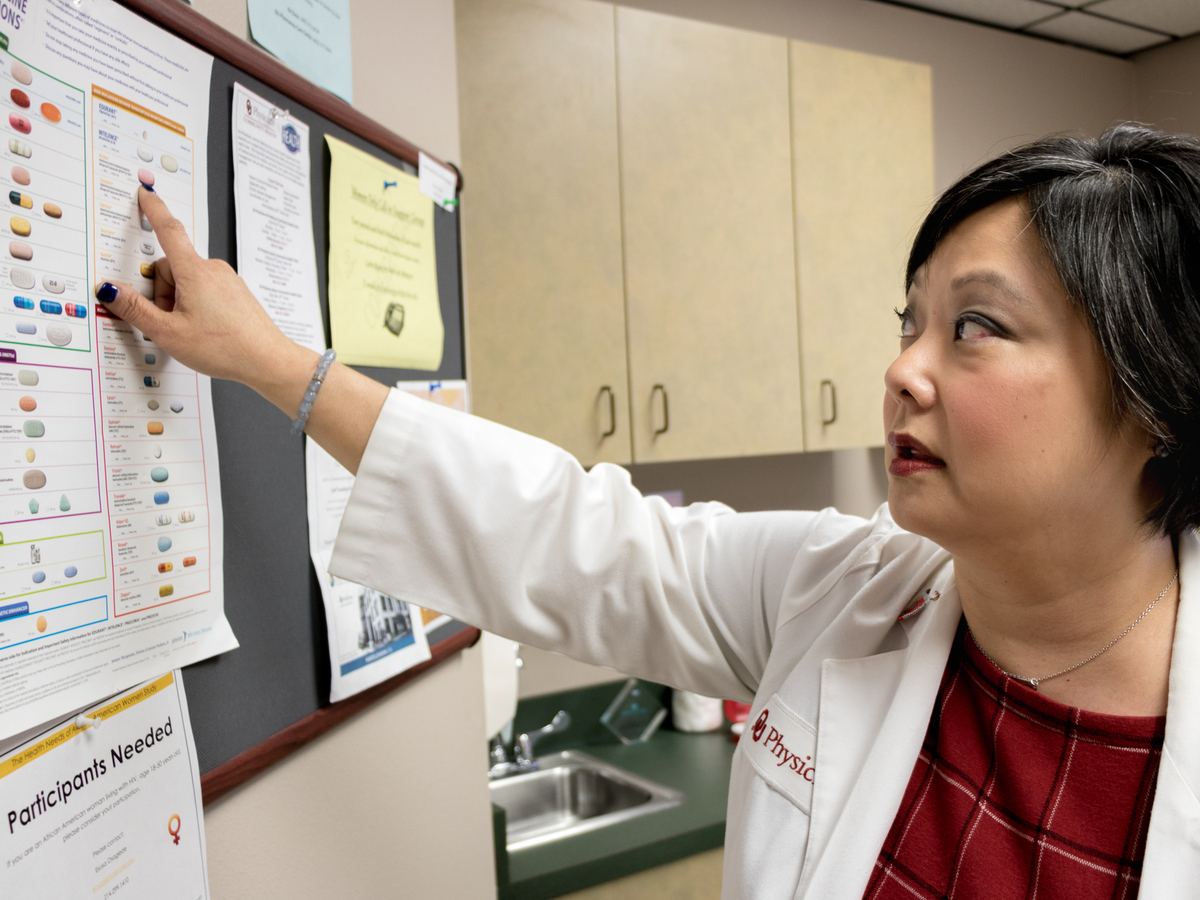
Dr. Michelle Salvaggio, medical director of the Infectious Diseases Institute at the University of Oklahoma Health Sciences Center in Oklahoma City, points to drugs used to treat HIV/AIDS. Medical advancements since the epidemic surfaced in the 1980s have helped many of her HIV-positive patients lead healthy lives.
Jackie Fortier/StateImpact Oklahoma
hide caption
toggle caption
Jackie Fortier/StateImpact Oklahoma
One of the goals President Trump announced in his State of the Union address was to stop the spread of HIV in the U.S. within 10 years.
In addition to sending extra money to 48 mainly urban counties, Washington, D.C., and San Juan, Puerto Rico, Trump’s plan targets seven states where rural transmission of HIV is especially high.
Health officials and doctors treating patients with HIV in those states say any extra funding would be welcome. But they say that strategies that work in progressive cities like Seattle won’t necessarily work in rural areas of Alabama, Arkansas, Kentucky, Mississippi, Missouri, Oklahoma and South Carolina.
Stigma around HIV and AIDS and around being gay runs deep in parts of Oklahoma, says Dr. Michelle Salvaggio, medical director of the Infectious Diseases Institute at the University of Oklahoma Health Sciences Center in Oklahoma City. The institute is one of two federally funded HIV clinics in Oklahoma; the other is in Tulsa, the second-largest city in the state.
A long drive for anonymity
Salvaggio’s clinic has six exam rooms where she sees patients, many of whom drive hours for treatment. The clinic used to employ a case manager in rural Woodward County, a little more than two hours’ drive northwest of Oklahoma City.
But Salvaggio says that having a case manager there ended up being a waste of money. “We had to let that position go, because nobody would go see her,” Salvaggio says. “Because they didn’t want to be seen walking into the HIV case manager’s office in that tiny town — that can only mean one thing.”
In Oklahoma, as in much of the U.S., black gay and bisexual men have the highest risk of HIV infection. Other groups with elevated risk in Oklahoma include Latinos, heterosexual women and Native Americans.
Salvaggio applauds the goal of ending HIV transmissions within 10 years, but says she doesn’t think it’s feasible in Oklahoma. The plan fails to recognize the particular ways different populations experience the epidemic, she says.
Native Americans in Oklahoma, for example, can’t count on the anonymity of a large health clinic.
“When they go into an Indian Health Service clinic, it is possible that they will see their cousin behind the desk, and their cousin’s brother-in-law working in medical records, and their niece’s boyfriend working in the pharmacy,” Salvaggio says.
Even if Native Americans have access to HIV care at the clinic, she says, “they are literally in fear of being outed.”

Ky Humble, who now lives in Oklahoma City, says there needs to be more support for people who are HIV-positive.
Jackie Fortier/StateImpact Oklahoma
hide caption
toggle caption
Jackie Fortier/StateImpact Oklahoma
Social support services needed
Ky Humble’s hometown is Afton, Okla., which had a population of about 800 people when he was growing up. He belongs to the Cherokee Nation, and was raised a Southern Baptist. He doesn’t remember learning about HIV at all when he was in school.
“Even if I did, it clearly wasn’t enough,” Humble says. “I knew I was gay in middle school; I think I would have paid attention.”
When he was diagnosed with HIV six years ago, at age 21, Humble felt like his life was ending.
“I knew that that was a thing, [but] I was very ignorant,” he recalls. “I was two weeks away from graduating from college — you’re supposed to be on top of the world. I thought it was a death sentence.”
He called his mom right away. She immediately drove across the state to be with him.
“We just sat there and cried for six hours straight,” Humble says. “And then we actually went [out] and bought several books on HIV, and just started reading them — to try to figure out what was going on.”
Today, Humble is healthy. His HIV levels are undetectable and he gets regular medical treatment to keep it that way. He now lives in Oklahoma City, but his family still lives in his hometown. He says some people back in Afton know he has HIV, and some don’t.
“It’s like coming out as diabetic,” Humble says. “I don’t necessarily tell people that I’m HIV-positive. It’s just part of who I am; it doesn’t define me.”
He says he is cautiously optimistic that the Trump administration’s plan could mean more funding for HIV prevention in Oklahoma. But rural Oklahomans, Humble says, also need access to “wraparound services” — such as food pantries, mental health therapy and transportation assistance — to help them deal with the disease.
“I have friends who have HIV and live in rural areas, and just getting to appointments is challenging,” he says.
Oklahoma’s uninsured rate is the second-highest in U.S.
Exactly how much money the president’s HIV plan will get is up to Congress. But even inexpensive, proven methods for fighting HIV — like distributing condoms — can be a tough sell in a state that doesn’t mandate comprehensive sex education.
Informational HIV talks with teenagers often turn into a basic health class for dispelling myths, says Andy Moore, clinic administrator of the Infectious Diseases Institute at the University of Oklahoma.

Dr. Michelle Salvaggio holds one of the medicines she prescribes to her patients with HIV.
Jackie Fortier/StateImpact Oklahoma
hide caption
toggle caption
Jackie Fortier/StateImpact Oklahoma
“We’ve had teenagers write questions like, ‘I’ve heard that if you douche with Mountain Dew after sex that it kills sperm,’ ” Moore says. They earnestly want to know if that’s true. “We have to back way up, and explain what sex is, how babies are made, different types of sex — before we can teach them about HIV prevention,” he says.
Salvaggio says thousands of people across Oklahoma would need to be tested for HIV to reach the administration’s goal. And Oklahoma has the second-highest uninsured rate in the nation after Texas — meaning many people don’t have a primary care doctor, let alone prescription drug coverage for drugs like Truvada, which can be used to prevent HIV infection.
It’s also one of 14 states that hasn’t expanded Medicaid under the Affordable Care Act. So, even if more people were HIV-tested, getting those that need it into treatment wouldn’t be easy, Salvaggio says.
Health care in Oklahoma is underfunded, she says, and couldn’t cope with a sudden influx of new patients. “I don’t know what we’d do with all those new patients,” she says. “We don’t have a facility to see them in, and we don’t have [the] providers.”
This story is part of NPR’s reporting partnership with StateImpact Oklahoma and Kaiser Health News. You can follow Jackie Fortier on Twitter: @JackieFortier.
In Arkansas, Thousands Of People Have Lost Medicaid Coverage Over New Work Rule

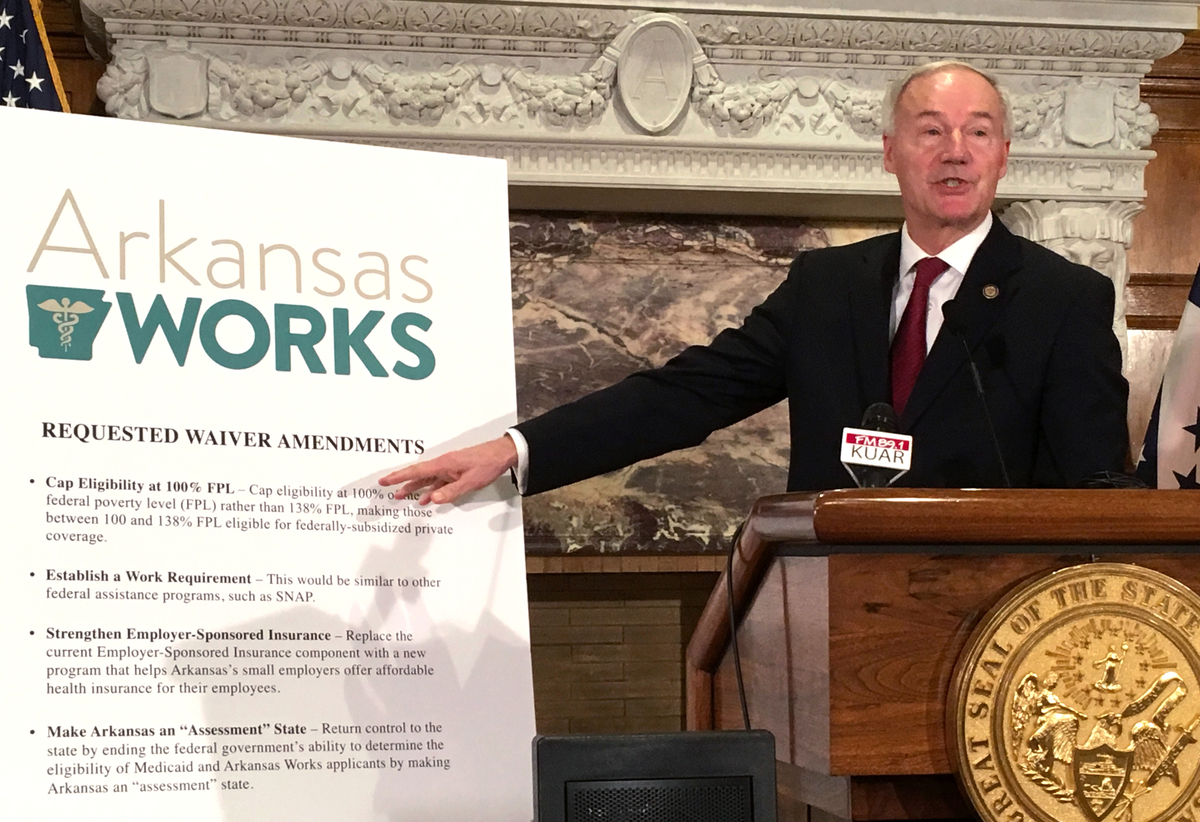
Arkansas Gov. Asa Hutchinson announces changes to the state Medicaid program called Arkansas Works, including the addition of a work requirement for certain beneficiaries, on March 6, 2017.
Michael Hibblen/KUAR
hide caption
toggle caption
Michael Hibblen/KUAR
Grisel Sustache Flores takes a seat at a health clinic in Springdale, Ark., for low-income patients. The 46-year old Puerto Rico native says she learned last fall that she qualified for Medicaid, which Arkansas expanded under the Affordable Care Act to cover more adults. It would cost her only $13 a month, so Flores, who suffers from multiple sclerosis, eagerly signed up.
“My doctors in Puerto Rico say my condition is very difficult,” Flores says through an interpreter at the Community Clinic facility. “Every day, it gets harder and harder.”
She holds out both hands. “Today my fingers are swollen and numb,” she says. “Some days it’s hard to stand for long periods.”
But in Arkansas, as in a handful of other states, Medicaid coverage now comes with some strings attached for certain beneficiaries. The Trump administration has allowed states to impose what’s known as a work requirement. In Arkansas, that means Flores has to work, volunteer or attend school at least 80 hours a month and periodically file progress reports to prove she’s doing so.
“Recently they have taken me out of enrollment because I was not reporting my hours of work,” she says.
Flores says losing her Medicaid health coverage was devastating because she needs medicines and physical therapy to control her disease. “I cried. I cried a lot,” she says.
Community Clinic serves 37,000 low-income patients in the northwest part of the state. Irvin Martinez, its health insurance enrollment specialist, says he’s witnessed a lot of turmoil among patients attempting to comply with the new Medicaid rules. In Arkansas, the program is called Arkansas Works.
Using his keyboard, Martinez opens the Arkansas Works web portal and clicks on some arrow icons. “I’ve actually seen, when I’ve logged into the website with them, that they are being locked out of their accounts if they enter the wrong data,” he says.
Patients who are locked out are instructed to call a hotline to help them complete their paperwork.
“But that has problems, too,” Martinez says. “I had one patient call and he was given the number to a prison, then to a private home. It took him three calls to the call center to get access to his account.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Community Clinic serves 37,000 low-income patients in northwest Arkansas at 13 locations, such as this one in Springdale. A Community Clinic insurance enrollment specialist says he’s seen firsthand the difficulties people have had trying to comply with the state’s new Medicaid work rule.
Courtesy of Lea Ann Thomas/Community Clinic
hide caption
toggle caption
Courtesy of Lea Ann Thomas/Community Clinic
In August 2018, a month after the work reporting requirement took effect, the state Department of Human Services said there were 265,223 total enrollees in Arkansas Works, with more than 62,000 of them subject to the new rule. By December, more than 18,000 had been disenrolled from their Medicaid insurance because they didn’t meet the requirement.
In response, DHS says it has beefed up its call center and is doing outreach to locate beneficiaries who might have lost insurance — by phone, email and home visits. The department has also launched an awareness campaign with paid advertising on public transit systems across the state and in college newspapers reminding people they need to comply with the work rule.
The department does offer a “good cause exemption” for beneficiaries dealing with unexpected circumstances that make it hard to meet the work requirement. But Martinez says Arkansas Works private insurance carriers and local nonprofits have had to step up to help confused patients navigate enrollment and reporting.
“Before the Affordable Care Act, nearly half of our patients were uninsured,” says Kathy Grisham, CEO of Community Clinic. “Many resorted to local emergency rooms for free health care.”
More people got insured when Arkansas expanded Medicaid. But Grisham says this new work requirement poses a serious burden on patients — and the providers who serve them.
“People do freak out when they find they are cut off,” she says. “So we shift them to our uninsured population because we are obligated to take care of them.”
Robin Rudowitz, associate director for the Kaiser Family Foundation Program on Medicaid and the Uninsured, says a few other states have also been approved by the Trump administration to test expanded Medicaid work rules, but those experiments cost money.
“We know Kentucky had done some original estimates that were in the range of $375 million to implement their waiver over two years,” she says.
Arkansas has spent $7.5 million on startup costs, according to the Department of Human Services.
But Gov. Asa Hutchinson, who initiated Arkansas Works, says the program is a success. “We’ve already had more than 7,000 Arkansas Works participants who have moved into work,” he says.
People disenrolled from Arkansas Works failed to comply, according to the governor, who says the work rule instills responsibility among certain Medicaid recipients who need a push.
“We are simply saying if you are able-bodied and able to work, and you don’t have dependent children at home,” he says, “you ought to either be working or you ought to be in school or you ought to be volunteering or contributing.”
Hutchinson says Medicaid case closures are often the result of churn — people moving away, earning too much money to qualify or securing health insurance elsewhere.
“There’s not an increase in uncompensated care,” he says. “There is not a huge flock of those coming back and re-enrolling this year, so I think we are seeing that the system is removing people who have been ineligible for the service.”
But KFF’s Rudowitz held anonymous enrollee focus groups and says enrollees reported steep learning curves in following the rules.
“The rules are complicated and involve multiple steps to comply, and many who were trying to comply faced some problems such as creating these online accounts or navigating the monthly reporting. They had problems with passcodes or couldn’t get assistance or had difficulty accessing the Internet, couldn’t find a computer, or were uncomfortable using a computer.”
In Springdale, Flores was able to re-enroll in Medicaid with the help of Martinez at Community Clinic. She pulls out her new insurance paperwork from her briefcase.
“My new documents have arrived,” she says, “and I am learning how it works.”
But Flores says she is now seeking counseling to help her cope with the stress of complying with her new health insurance.
Legal Aid of Arkansas, acting on behalf of nine Arkansas Works patients, has filed a lawsuit against the federal government over the regulations. The suit argues that the requirements are too cumbersome and cause harm to recipients.
Venezuela's Collapse Puts Strain On Latin American Health Care
The collapse of the health care system in Venezuela is having ramifications throughout Latin America. Disease outbreaks across the continent are being linked back to Venezuela.