Racial Disparities In Cancer Incidence And Survival Rates Are Narrowing

Dramatic decreases in deaths from lung cancer among African-Americans were particularly notable, according to the American Cancer Society.
Siri Stafford/Getty Images
hide caption
toggle caption
Siri Stafford/Getty Images
For decades, the rate of cancer incidence and deaths from the disease among African-Americans in the United States far outpaced that of whites. But the most recent analysis of national data by the American Cancer Society suggests that “cancer gap” is shrinking: In recent years, death rates from four major cancers have declined more among blacks than among whites.
The report was published online Thursday in CA: A Cancer Journal for Clinicians, a peer-reviewed journal of the American Cancer Society.
African-Americans still bear a disproportionate share of the cancer burden in the U.S., having the highest death rate and the lowest survival rate of any racial or ethnic group for most cancers.
“In 2019, approximately 202,260 new cases of cancer and 73,030 cancer deaths are expected to occur among blacks in the United States,” the analysis by ACS investigators notes.
But their report also shows that the gap between blacks and whites has closed considerably over the past few decades when it comes to lung, prostate and colorectal cancers. In fact, during the period from 2006 to 2015, overall death rates from cancer declined 2.6 percent per year among black men, compared to 1.6 percent per year among white men. Among women, for that same time period, death rates from cancer declined 1.5 percent per year among blacks compared to 1.3 percent per year among whites.
“Twenty?five years of continuous declines in the cancer death rate among black individuals translates to more than 462,000 fewer cancer deaths,” according to the report’s authors.
The improvement among African-Americans is largely due to dramatic decreases in incidence and death from lung cancer, says Dr. J. Leonard Lichtenfeld, acting chief medical officer for the American Cancer Society, and that likely reflects the steep declines in the prevalence of smoking.
“I can’t say why smoking has decreased so dramatically in the black community but the fact that it has is very good news,” he says. “It has significantly narrowed the gap between blacks and whites and we are very grateful.”
Still, racial disparities in cancer continue. The reasons are likely multiple, Lichtenfeld notes, and include disparities in education, socioeconomic status and access to health care.
When the U.S. ensures that everyone has equal access to good health care, screening and treatment, Lichtenfield says, “we’ll see even greater success. We have to make a commitment to make that happen.”
Why Men In Mississippi Are Still Dying Of AIDS, Despite Existing Treatments

President Trump has pledged to eliminate HIV in America by 2030. But in the South, rates of HIV/AIDS among black gay and bisexual men remain stubbornly high.
Medical Anthropologist Explores 'Vaccine Hesitancy'
Hesitancy about vaccination in a community has a lot to do with acculturation to its norms.
Karl Tapales/Getty Images
hide caption
toggle caption
Karl Tapales/Getty Images
Distrust of vaccines may be almost as contagious as measles, according to medical anthropologist Elisa Sobo.
More than 100 people have been infected with measles this year, according to the Centers for Disease Control. Over 50 of those cases have occurred in southwest Washington state and northwest Oregon in an outbreak that led Washington Gov. Jay Inslee to declare a state of emergency on Jan. 25.
Some public health officials blame the surge of cases on low vaccination rates for this highly infectious disease.
Clark County, Wash. — the center of the current spate of cases — has an overall vaccination rate of 78 percent, but some schools in the county have rates lower than 40 percent.
Washington is one of 17 states that allows a parent to send his or her child to public school not completely vaccinated because of a “philosophical or personal objection to the immunization of the child.”
What makes some families reluctant to vaccinate their children? Sobo, a professor at San Diego State University, says it may be driven in part by the desire to conform in a community where many parents are skeptical of vaccines.
To better understand how parents decide not to vaccinate, Sobo interviewed families at a school with low vaccination rates in California. She found that skepticism of vaccines was “socially cultivated.”
Parents who believe that vaccines are dangerous persuaded other parents to believe the same thing by citing fears of “mainstream medicine” harming their children. Enrolling in the school even seemed to change the beliefs of some parents who had previously followed the state-mandated vaccine schedule: They started to refuse vaccines.
NPR’s Audie Cornish spoke with Sobo on All Things Considered. These interview highlights have been edited for clarity and length.
What are the common ideas that we have about families that don’t believe in vaccination?
One common idea would be that they’re all absolutely looney-tunes, crazy people wearing tinfoil hats and reading all these conspiracy theories on crazy blogs on the Internet. And that is absolutely not the case. What I found was that most of the people who are hesitating to vaccinate … They’re really smart people, and they’re highly, highly educated.
Back in 2012, you actually spoke to some parents in California, in a community where parents had their kids at a fairly progressive school. Half of kindergarteners had gotten exemptions from vaccines. What was going on in this community?
Often, the parents, the family didn’t arrive at the school having any hesitancy about vaccinations … As they acculturated or became part of the community, that’s when these kinds of beliefs and practices would take hold.
The longer the family had been in the community, … this practice of being hesitant about vaccinations evolved and it became part of that family’s medical practice.
[In areas where there are low vaccination rates], there tends to be a more open norm, where not vaccinating is accepted or sometimes even encouraged. When you have people surrounding you that move in that direction, to go in a different direction has social costs.
It’s not just the facts and the information that you’re going by. It’s: “What are the norms? What are people around me doing? And they seem to be OK, and everything’s working out for them.”
Think about yourself and the clothes that you wear to work. I’m guessing that you probably don’t have a formal dress code, but you kind of look around, and you see: “Oh, OK, this is what we’re expected to wear to work.” And you just do it.
Are you talking about a formal kind of peer pressure?
The peer pressure is not formal.
Informally, there becomes a sort of feeling in the community. It becomes known for not vaccinating.
There are parts of the country where there’s the opposite expectation, where someone who didn’t want to vaccinate their kids might be socially isolated for that decision.
And then their behaviors would be pushed underground. They might not feel comfortable telling other people.
When you see what’s going on in Washington State, what came to mind for you?
What is the media coverage going to do? Are they going to vilify these parents?
That witch hunt aspect is not helpful to have a good discussion about vaccination. It needs to be much more open and much less polarizing.
Are people ready to listen? Can there be convincing?
I think people are very ready to listen — if they’re heard. If you listen to them, and you allow them to say what they think without feeling judged, without pushing them into a corner, they’re absolutely ready.
Mara Gordon is a family physician in Washington, D.C., and a health and media fellow at NPR and Georgetown University School of Medicine.
'Church Of Safe Injection' Offers Needles, Naloxone To Prevent Opioid Overdoses

A man who goes by the name Dave Carvagio holds a packaged syringe in Pickering Square in Bangor, Maine. The Bangor chapter of the Church of Safe Injection sets up a table in the square and offers free naloxone, needles and other drug-using supplies.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
On a bitter cold afternoon in front of the central bus stop in Bangor, Maine, about a half-dozen people recently surrounded a folding table covered with handmade signs offering free clean syringes, coffee and naloxone, the drug also known as Narcan that can reverse an opioid overdose.
They’re with a group called the Church of Safe Injection that is handing out clean drug-using supplies in cities around the U.S.
Even though they could be arrested for doing so, volunteers say they have to step up because of the staggering number of opioid overdose deaths and because the public health system has failed.
“There are all these barriers to people getting well — like insurance and treatment rules,” said one of the Bangor volunteers who goes by the name Dave Carvagio, though it’s not his real name. “It’s to the point where, for some people, the only treatment options are in institutions like prison.”
Carvagio doesn’t want to be identified because it’s illegal in Maine to have more than 10 hypodermic syringes unless you’re a certified needle exchange. Police cars sometimes circle the park, but no one has been arrested — yet.
“I believe that there is not just like a moral duty to violate unjust laws, but in this circumstance a spiritual duty,” Carvagio said. On this day, they gave out 100 syringes, 10 naloxone kits and made one referral to treatment.
Bangor police Sgt. Wade Betters knows about the group. He says he’d like to sit down and meet with the volunteers, but he believes their focus should be on getting people into treatment.
“You know, if you’re committing a crime in the state of Maine, you could be subject to arrest or ticketed,” Betters said. “But in these cases, we use a lot of discretion because the goal is the same — to save lives.”
In Lewiston, Maine, police have taken a different position. They’ve warned the group not to give out clean syringes in a local park because it’s against state law. So the group members have arranged to meet with people and bring the supplies to different meeting spots.
Driving through Lewiston one night, in a car packed full of boxes of syringes and other drug-using equipment, Kandice Child met up with two young men standing near a convenience store.
“I’m going to give you 100 [syringes],” Child told one of the men. “What about alcohol wipes, you need any of those?”

A drug user in Lewiston, Maine, puts used needles into a sharps container to be exchanged for clean needles.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
Child gave them naloxone and test strips for the powerful opioid fentanyl. She says she only gives clean needles when someone returns their used ones so as to help keep syringes off the streets. Child says she does this because she has a family member who is struggling. She also says there are only six certified needle exchange programs in Maine, none in Lewiston.
“Why wait?” Child asked. “Should we all sit around and talk and point fingers or should we get off our a– and do something about it? This helps, it works, it saves lives, it reduces HIV, it reduces hepatitis, and it keeps syringes off the streets.”
Next stop was an apartment where three people were waiting to trade containers filled with used syringes for clean ones. Another volunteer demonstrated how to use naloxone as Child filled out paperwork keeping track of what she’s handed out.
A 36-year-old man — who didn’t want his name used because he’s using drugs — was uneasy. He says he’s glad to get the clean equipment but that he’s conflicted about whether getting these supplies makes it easier for him to use drugs.
“The only reason I struggle is the inner conflict, you know? It’s preventative maintenance yet at the same time it’s enabling, you know?” he said.
A woman in the apartment, who also didn’t want to be identified, chimed in: “I understand, but what are you supposed to do? If someone isn’t able or ready to go to treatment — should they die?”
Even the founder of the Church of Safe Injection, Jesse Harvey, 26, acknowledges that he’s struggled with the same questions. But he says working in addiction recovery has made him frustrated by the deaths and barriers to treatment. He says there are criteria to becoming a legitimate syringe exchange program that he’s not likely to meet, so he started this church.

Jesse Harvey, founder of the Church of Safe Injection, stands in a Denny’s parking lot in Auburn, Maine, alongside four sharps containers filled with used needles collected from drug users around the neighboring city of Lewiston.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
Harvey says there are now 18 chapters of the Church of Safe Injection in eight states — all of them funded by private, anonymous donations. Each one is independent but must abide by three rules: to welcome all people of all faiths, to serve all marginalized people and to support harm reduction.
But he says the group is not supporting legalizing drugs.
“We’re not saying it’s our religious belief to use heroin. No, not at all,” Harvey said. “We’re saying that it’s our sincerely held religious belief that people who use drugs don’t deserve to die when there are decades of solutions.”
Harvey plans to register the church as a nonprofit and then argue for a religious exemption from drug laws. He says the U.S. Supreme Court has already ruled that a religious group is allowed to use the illegal psychedelic ayahuasca in its rituals.
“I don’t think it’s illegal, and if it is, I think we have a religious exemption here,” Harvey said. “With the high rate of fatal opioid poisoning in Maine, why criminalize a group of people with lived experience who are trying to save lives? If the state is not going to do something about this, well guess what? We’re going to.”
Harvey says eventually he hopes to have a location for the church that will include a site where people could inject drugs under supervision. Such supervised injection sites are legal in some other countries, but Justice Department officials have warned that they will prosecute anyone operating one in the U.S. Nevertheless, at least a dozen U.S. cities are considering whether to open a site.
For now, Harvey says his congregants will continue to risk arrest to hand out supplies.
This story was produced in partnership with WBUR.
Doctor Weighs In On Supreme Court's Decision To Block Louisiana Abortion Law
NPR’s Michel Martin speaks with Dr. Willie Parker about the recent Supreme Court decision regarding abortion access in Louisiana.
An Overview Of State Abortion Laws
Scott Simon talks to Julie Rovner, chief Washington correspondent for Kaiser Health News, about new abortion laws in state legislatures across the country.
SCOTT SIMON, HOST:
This week, the U.S. Supreme Court blocked Louisiana from enforcing a restrictive abortion law. The court will likely hear a challenge to the merits of that law this fall. Many states are moving to pass a number of new abortion laws to prepare for the possible overturn of Roe v. Wade, that 1973 decision that legalized abortion in the United States. We’re going to turn now to Julie Rovner, chief Washington correspondent for Kaiser Health News. Jules (ph), thanks so much for being with us.
JULIE ROVNER: Thanks for having me.
SIMON: Chief Justice Roberts, of course, joined four liberal justices on the Supreme Court to temporarily block that abortion law from going into effect in Louisiana. What impact does that have in the state and other states?
ROVNER: Well, for the moment, that law will not be enforced while the case proceeds its way through the Supreme Court, which is now what we’re expecting. It was similar to a law in Texas that was actually struck down by the court in 2016 that required doctors who perform abortions to have admitting privileges at nearby hospitals. In 2016, the Supreme Court majority said that was not necessary. And then Louisiana passed this law anyway. It was sort of surprisingly upheld by the 5th Circuit Court of Appeals. And now the Supreme Court will have it as a possibility to either reverse or seriously undermine Roe v. Wade.
SIMON: Anti-abortion activists, of course, hope that Roe v. Wade will be overturned now that the balance of the Supreme Court may have shifted. A number of Republican-controlled legislatures are passing laws that would go into effect if that happens. What are those laws like?
ROVNER: Well, there are a whole number of different laws. There are what are called trigger laws. Those are laws that say if Roe v. Wade is struck down, then abortion would become illegal. There are other laws that states are passing that they are using to try and get the Supreme Court to either overturn Roe v. Wade or to undermine it. Those include not just the laws like the one in Louisiana, but there are bans on specific types of abortion procedures, particularly what’s called the D&E, which is the most common second trimester form of abortion.
There is an Indiana law that bans abortion for sex selection or in the case of fetal deformity. That one is near to getting a decision by the Supreme Court whether they will hear it. So there are a number of different ways that states are looking at trying to sort of make abortion either much more difficult to get or completely illegal.
SIMON: There are Democratic lawmakers in Virginia and New York state that have gotten attention for bills that would loosen abortion restrictions, especially in the third trimester. What else are some Democrats doing at the state level?
ROVNER: Well, mirroring what anti-abortion lawmakers are trying to do in more red states to make abortion illegal if Roe v. Wade was struck down, lawmakers in bluer states are trying to pass laws that would ensure that abortion remains legal. Remember; Roe v. Wade just said that states couldn’t ban abortion. So if it were struck down, it would be up to each individual state. So we’re seeing a number of states who are trying to either rewrite old laws or pass new laws that say if Roe v. Wade were to go away, abortion would remain legal in the state. There are other things that states are doing. In some of the blue states, they’re looking at ensuring that abortion is covered by insurance. That is not the case in some states; it is in others. They’re looking at making sure that women have easier access to other reproductive health services like birth control to make sure that abortions are not as necessary.
SIMON: The Trump administration is expected to soon announce its plan for funding family planning services. What do we expect from that?
ROVNER: We expect the administration to try and basically evict Planned Parenthood from the federal family planning program. This is a goal that goes back for anti-abortion activists to the 1980s. Planned Parenthood does not use federal funds for abortions. That is not allowed. But they do use their own private funds for abortions, and they also take federal money to provide family planning services. Basically, what these rules would do if they come out as we expect is they would say that if you are performing abortions, you must do it at a separate facility than one where you’re using federal funds to provide family planning services.
And also it would ban abortion referrals for women with unintended pregnancy. Currently, those are required if the woman seeks them, that counseling is also required, woman with an unintended pregnancy is to be given all of her options. And if she asks for an abortion referral, she is to be given one. That would basically be reversed under the new rules – at least as we expect them to come out.
SIMON: Julie Rovner is chief Washington correspondent for Kaiser Health News. Thanks so much for being with us.
ROVNER: You’re so welcome.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
How To Demand A Medical Breakthrough: Lessons From The AIDS Fight

AIDS activist group ACT UP organized numerous protests on Wall Street in the 1980s. The group’s tactics helped speed the process of finding an effective treatment for AIDS.
Tim Clary/AP
hide caption
toggle caption
Tim Clary/AP
In the summer of 1985, Mike Petrelis was savoring life as young, openly gay man in New York City. He’d landed a cool job working for a film publicist who mostly handled foreign art films. He’d found an affordable apartment — not far from the gay mecca of Greenwich Village.
Then one day, Petrelis noticed a sort of blotch on his arm.
He went to a doctor, who ran a new kind of test, and gave Petrelis the verdict: “You have AIDS.”
In the Other Side Of Anger, NPR explores the biology, psychology and cultural role of anger, shedding light on an emotion that can spur violence or become a force for good. Read the rest of the series here.
“He was saying that if I was going to be lucky I’d have six months to maybe two years of life left,” recalls Petrelis.
He was 26 years old.
Petrelis says he broke down crying. The doctor said he’d give Petrelis a moment to be alone, pull himself together.
And sitting in that pristine exam room, Petrelis made his first act of protest: “I took out a cigarette.”
He did it precisely because he knew it was forbidden.
“I was so mad with hearing this news — so angry at the doctor — I thought the one best way to protest would be to light up a cigarette and just smoke it with as much pleasure as I could find,” he says.
But in the months that followed Petrelis soon shifted the focus of his rage, as he began to learn just how little the government and medical establishment had done to address a crisis that, at the time, mostly afflicted gay men. This was four years after AIDS first made headlines. More than 6,000 Americans had already died. Yet the budget for AIDS research was a fraction of what the U.S. government spent on diseases that were far less threatening. President Ronald Reagan had yet to even say the word AIDS in public. And only one private pharmaceutical company was seriously pursuing a treatment.
“I mean, my anger just knew no limits,” says Petrelis.
Over the next decade, this rage would drive not just Petrelis but thousands of gay men and their supporters to form one of the most influential patient advocacy groups in history.
They called themselves AIDS Coalition to Unleash Power — or ACT UP. And they ultimately forced the government and the scientific community to fundamentally change the way medical research is conducted — paving the way for the discovery of a treatment that today keeps alive an estimated half-million HIV-positive Americans and millions more worldwide.
But as central as anger was to ACT UP’s success, it would also prove a force for division.
“It was a war zone”
All this was unimaginable to Petrelis back in 1985. As furious as he was with the government, he was just as indignant that so few other gay men around him seemed to echo his rage.
“I just thought because I was so angry that there should have been more angry people,” he recalls.
The gay and lesbian community had created a dynamic network of self-help groups in response to the crisis. But their focus was on providing comfort to the sick: buddies to take you to hospital, lawyers to help you write your will.
Petrelis remembers exploding at one of them: “I don’t want to write my will! I want a cure!”
One of the recruits to those self-help groups was a young lawyer named David Barr. Back then he felt too overwhelmed to give much thought to asserting his anger.
All around him fellow gay men were suddenly falling sick with horrific symptoms — skin cancer, extreme weight loss, incontinence. Hospitals were turning them away. Employers were denying them benefits.
“It was a war zone,” Barr recalls. So at first his overriding feeling was, “I don’t have time to go yell at politicians. I’ve got to diaper somebody. I’ve got to create a legal services program to keep people from being evicted.”
But Barr was also starting to grow restless. The work he was doing to set up support systems felt vital.
“But it was never satisfying,” he says. “Because whatever help we were providing was really temporary. We lost everybody.”
Boiling over
By early 1987, with the U.S. death toll topping 40,000 and worldwide HIV infections reaching 5 to 10 million, the threat was starting to feel apocalyptic. The gay community’s mounting frustration finally boiled over in an explosive show of anger.
Hundreds of gay men and their supporters took to New York City’s streets to vent their fury — first with a demonstration on Wall Street. Then a protest at city hall. Then an even bigger showdown on Wall Street.
Barr and Petrelis had been to gay rights demonstrations before — pride rallies, candlelight vigils for people who had died of AIDS. But this time, says Petrelis, “something felt different.”
People weren’t just chanting or carrying signs. They were blocking traffic with their bodies.
At the second Wall Street action, “over a hundred people got arrested,” Barr says. Many of them were people who had never contemplated civil disobedience before.
“It was such a terrific feeling to be arrested with my yoga teacher,” Petrelis recalls with a chuckle.
And it was profoundly affirming. “All those men and women screaming at the top of their lungs — I felt they were taking my anger and putting it out there to the world.”
For Barr, participating in the outpouring was galvanizing.
“Rallying together and expressing our anger was a really good replacement for just feeling scared all the time,” he says.
“It felt powerful. And it gave us a way of saying, ‘OK, we’ve got to do something more than just buy people groceries, and take them to the hospital, and plan memorial services.’ The anger is what helped us fight of a sense of hopelessness.”
Soon the group — which the New York demonstrators named ACT UP at an early planning meeting — was going national, with thousands of people across the country staging similar actions.
Getting strategic
ACT UP quickly made its name with tactics that were unapologetically confrontational, says David France, the author of a history of AIDS activism called How to Survive a Plague, as well as a 2012 documentary by the same name.
“ACT UP’s ethos was that they had united in anger,” he says.
“They would storm people’s offices with fake blood and cover people’s computers with [it],” he says. “They locked themselves to politicians’ desks. At one point, they barged into a meeting of a pharmaceutical company and turned over the shrimp cocktail tables.”

Demonstrators from the organization ACT UP protest in front of the headquarters of the Food and Drug Administration. The FDA opened up access to experimental drugs soon after.
J. Scott Applewhite/AP
hide caption
toggle caption
J. Scott Applewhite/AP
This made them extremely intimidating. “They were no longer invisible sufferers of a disease. They were terrifying sufferers of a disease,” says France.
But initially, says France, “the actions had the air of purposeless anger.”
That changed when ACT UP began to deploy its anger strategically.
Barr says the demonstrations started off as a simple release: “We were angry and we needed to express ourselves.”
But in doing so, he says, “we began to realize, ‘Oh, this is a tactic that we can put to good use.’ “
So they took it upon themselves to figure out the specific roadblocks in government policy and clinical trials that stood in the way of what ACT UP wanted most: a cure. Then they unleashed their rage to force the decision-makers to hear ACT UP’s solutions.
They kicked off the approach at a government building in suburban Maryland.
“Our goal was to seize control of the FDA,” says Barr.
ACT UP wanted the Food and Drug Administration to give AIDS patients access to an experimental drug. The FDA wouldn’t even discuss it.
So hundreds of activists converged on the FDA’s headquarters.
“One group were wearing lab coats that were stained with bloody hands,” recalls Barr. “Other people brought tombstones that they made and lied down in front of the building and held up the tombstones: ‘Dead from FDA red tape.’ “
The activists advanced in rows, blocking the entrances. The demonstration made national news.
Within days the FDA agreed to meet. In a couple months, officials opened up the policy on access to experimental drugs.
France says the two prongs of ACT UP’s strategy were equally important. The aggressive protests got them a foot in the door, but it wouldn’t have made a difference if they hadn’t done the homework needed to offer insightful and viable proposals once they did get a meeting.
“What made this work was not just the anger. But the anger coupled with the intelligence,” says France.
ACT UP came to call this approach its “inside-outside strategy.” And they deployed it over and over again — with the National Institutes of Health, and then with pharmaceutical companies, eventually becoming full partners with key scientists.
The upshot of all this: “What they were able to revolutionize was really the very way that drugs are identified and tested,” says France.
This included scrapping the prevailing practice of testing drugs on a small number of people over a long period of time in favor of testing a huge sample of people over a much shorter period — significantly speeding up the time it took to conduct drug trials.

December 1989: At left, members of ACT UP mount a protest outside St. Patrick’s Cathedral in New York. At right, activist Michael Petrelis inside the cathedral shouts “Stop killing us!” in the middle of the service.
Images from the documentary “How to Survive a Plague” by David France
hide caption
toggle caption
Images from the documentary “How to Survive a Plague” by David France
Similarly, ACT UP insisted that the researchers and pharmaceutical companies that were searching for a cure for AIDS also research treatments for the opportunistic infections that were killing off AIDS patients while they waited for a cure.
In the process, says France, “ACT UP created a model for patient advocacy within the research system that never existed before.”
Today it seems natural that people suffering from a disease — whether that’s breast cancer or diabetes — should have a voice in how it is researched and treated. But France says this was decidedly not the norm before ACT UP.
In 1996, scientists finally did find the treatment that would keep people alive. France says while scientists would probably have made the discovery eventually, there’s “no question” ACT UP made it happen sooner.
But an organization that uses anger as a tool also faces a challenge. Once you get people to tap into their rage — it’s hard to control it.
“Stop killing us!”
That contradiction came to a head for ACT UP one Sunday in December of 1989 at Manhattan’s St. Patrick’s Cathedral.
Outside the church, ACT UP was staging a massive demonstration to call out Archbishop John O’Connor for opposing the use of condoms.
Petrelis was part of a smaller group that decided to take the protest inside — to the mass.
He’d been raised Roman Catholic and had a lot of unresolved feelings toward the church.
“You know condemning me as gay, just all that Catholic guilt I had been raised with,” he says.
They didn’t want to disrespect parishioners, so the plan was to wait for O’Connor to begin his sermon, interrupt by reading a quick statement, then turn their backs on him in silent protest.
But as Petrelis watched his fellow activists begin, he says something inside of him stirred: “I felt there was just not enough anger that could be heard.”
Petrelis had a whistle with him — the kind for calling for help when you’re being attacked. He started blowing it.
“Loudly,” he recalls, “I stood up on the pew literally blowing the whistle on centuries of horrible treatment by the church toward gays and towards women.”
Even that didn’t feel like enough. Petrelis pointed his finger at the archbishop: “I started screaming, ‘Stop killing us! Archbishop O’Connor, Stop killing us!’ “
France’s documentary includes footage of the moment — Petrelis standing on the pew, other activists taking up the chant “Stop it! Stop it!” Still more leaping into the aisle and laying on the floor as police march in to cart them off.
O’Connor continued the service. An activist lined up for communion, then took the wafer the priest had given him, and crumpled it.
The aftermath
David Barr had opposed this protest. The result confirmed his fears.
“The next day the story on the front pages of the newspapers was not, ‘Look at all these horrible HIV policies the church is promoting.’ It was, ‘Gay guy spits body of Christ out on the floor.’ “
Barr was part of a contingent within ACT UP that felt the time had come for a new phase. He believed ACT UP’s inside-outside strategy had largely succeeded. Top policy makers and scientists were now giving ACT UP’s proposals a respectful hearing.
But AIDS activists had not yet convinced the political class to mobilize the full resources of the federal government behind the search for a cure. For that, ACT UP would need to build this into a movement of not thousands but hundreds of thousands — the kind that sways elections. And this would require reaching out to all sorts of other groups affected by AIDS, such as Latinos — who are Catholic.
“I just remember my first thought being, well that’s the end of our coalition building with the Latino community,” Barr says. “That’s it. Nobody’s going to talk to us.”
ACT UP continued to mount demonstrations — there are active chapters of the organization to this day. But to Barr it marked the beginning of the end of ACT UP’s effectiveness.
“It was a turning point where venting one’s anger took precedent over political strategy,” he says.
Within a year Barr and many others who had been central to the organization’s meetings with top researchers had parted ways — splitting off into groups with a more traditional style of lobbying and politicking.
As for Petrelis, he has no regrets.
In general, he disputes the notion that ACT UP became less strategic and effective from that point on. And while he concedes, what happened at St. Patrick’s Cathedral was unplanned and not in service of any tactical objective, he argues in the broader scheme it was deeply necessary.
“It was a catharsis finally happening,” he says.
And not just for the activists in the cathedral, he says. Petrelis has been in movie theaters when David France’s documentary has been shown.
When that scene comes on — of his younger self screaming at the archbishop — “people stand up,” he says, “and they applaud me.”
Former Rep. John Dingell Left An Enduring Health Care Legacy

Utah Voters Approved Medicaid Expansion, But State Lawmakers Are Balking

Republican lawmaker Allen Christensen is pushing a bill in the Utah Senate that would shrink the Medicaid expansion his state’s voters approved. “They are not obligated to balance the budget,” he argues. “We are.”
Cory Dinter/KUER
hide caption
toggle caption
Cory Dinter/KUER
Utah residents may have thought they were done fighting about Medicaid expansion last November. During the election, voters approved a ballot measure to expand the health program for low-income residents to cover 150,000 uninsured people in the state. But when Utah lawmakers opened a new legislative session in late January, they began pushing through a bill to roll back the scope and impact of that expansion.
“We voted for this on Nov. 6. We were very clear about what we wanted,” says Andrew Roberts, a spokesman for Utah Decides, the group that organized the Medicaid expansion referendum, known as Proposition 3.
“We are frustrated, and I think Utahns are frustrated,” he says.
He’s so frustrated that his group hired a billboard truck to drive in circles around the Capitol building and through the snowy streets of Salt Lake City and its suburbs. Signs on the sides of the truck flash phrases in LED lights, including “Support democracy. Support Utah’s vote.” A looping video advertisement urges residents to call lawmakers “who don’t respect the will of the people.”
After six years of talking about Medicaid expansion, voters approved the ballot measure on Nov. 6, by 53 percent. But the issue erupted again when the legislative session started Jan. 28.
Similar legislative efforts to curtail expansion are also happening in Idaho, where voters passed a Medicaid expansion initiative in November by a 60 percent majority. Idaho lawmakers are considering ways to scale that program back.
In politically and fiscally conservative Utah, legislators argue the 0.15 percent non-food sales tax that voters approved won’t be enough to pay for Medicaid expansion. So they’ll pass an expansion, but only a very limited one.
Voters “wanted Medicaid expansion and that’s what we’re doing,” says Republican state Sen. Allen Christensen. But, he adds, the voters “didn’t fill in the proper blanks. We are filling in those blanks for them. They are not obligated to balance the budget. We are.”

A billboard truck showing advertisements in support of expanded Medicaid has been parading past the state Capitol in Salt Lake City.
Cory Dinter/KUER
hide caption
toggle caption
Cory Dinter/KUER
Christensen is leading the rollback effort in Utah. His alternative proposal, SB 96, would cap the number of individuals who would qualify for Medicaid, add work requirements and lower the annual income limit. Prop. 3 supporters had wanted the coverage available for people who made up to 138 percent of the federal poverty level, or about $16,000 a year. But Christensen’s bill would offer Medicaid coverage only to people who made less than 100 percent of the federal poverty level, or about $12,000 for an individual.
Making those changes would require the state of Utah to get approval for two federal waivers from the federal Centers for Medicare and Medicaid Services. Proposition supporters point out that similar requests from other states have been denied.
“From the perspective of voters, I think voters have a right to be furious right now,” says Matt Slonaker, executive director of the Utah Health Policy Project, another group that has supported Medicaid expansion.
Slonaker says changing the scope of Prop. 3 would mean fewer people getting health coverage, and the state would receive less money from the federal government. He also fears it could make voters feel disillusioned.
“Why would voters ever want to pursue ballot initiatives and direct democracy if the legislature’s just going to repeal it anyway?” Slonaker asks.
While some Utah lawmakers, such as Christensen, describe being “philosophically opposed” to Medicaid expansion, much of the political debate in Utah is about how much expansion will cost, and whether the new sales tax will pay for it. Supporters point to the fiscal experience of other states.
“You should think of Medicaid expansion as no different than if you said, ‘Oh, hey, somebody’s going to go open up a factory,” says Bryce Ward, an economist at the University of Montana, in Missoula. “And that factory is going to bring, in the case of Montana, $600 million of outside money into the state that we’re going to pay to workers here.”
Ward recently published a report on the economic impacts of Medicaid expansion in Montana during the first two years of that program. He says it brought in about $600 million dollars in new funds to the state per year. That money supported about 6,000 jobs, he adds, or about $350 million in additional income for residents.
Ward says states like his also can take advantage of savings, because Medicaid expansion makes providing health care to certain groups, like prisoners, more affordable. While states do have to pay 10 percent of the cost of expanded Medicaid (the federal government covers 90 percent — a more generous “match” than traditional Medicaid), the combination of savings and economic growth meant that, in the case of Montana, the program basically pays for itself, Ward says.
“The benefits that people in Utah have is that people like me in other states have done the work trying to figure this out,” he says. “Or at least get some ballpark estimates of it.”
So far, Utah lawmakers remain unconvinced by studies like Ward’s. The bill to restrict Medicaid expansion is moving fast, and could reach the governor’s desk as soon as next week.
Avoiding The Ouch. Scientists Are Working On Ways To Swap The Needle For A Pill

A team of researchers in Boston has developed an insulin-delivery system that injects the medicine directly into the stomach wall, which is painless.
Felice Frankel/MIT
hide caption
toggle caption
Felice Frankel/MIT
Many vaccines and some medicines, such as insulin, have to be delivered by injection. That’s a pain, both for patients and for health care providers. But two groups of researchers are trying to put some of these medications in pill form to avoid the needle.
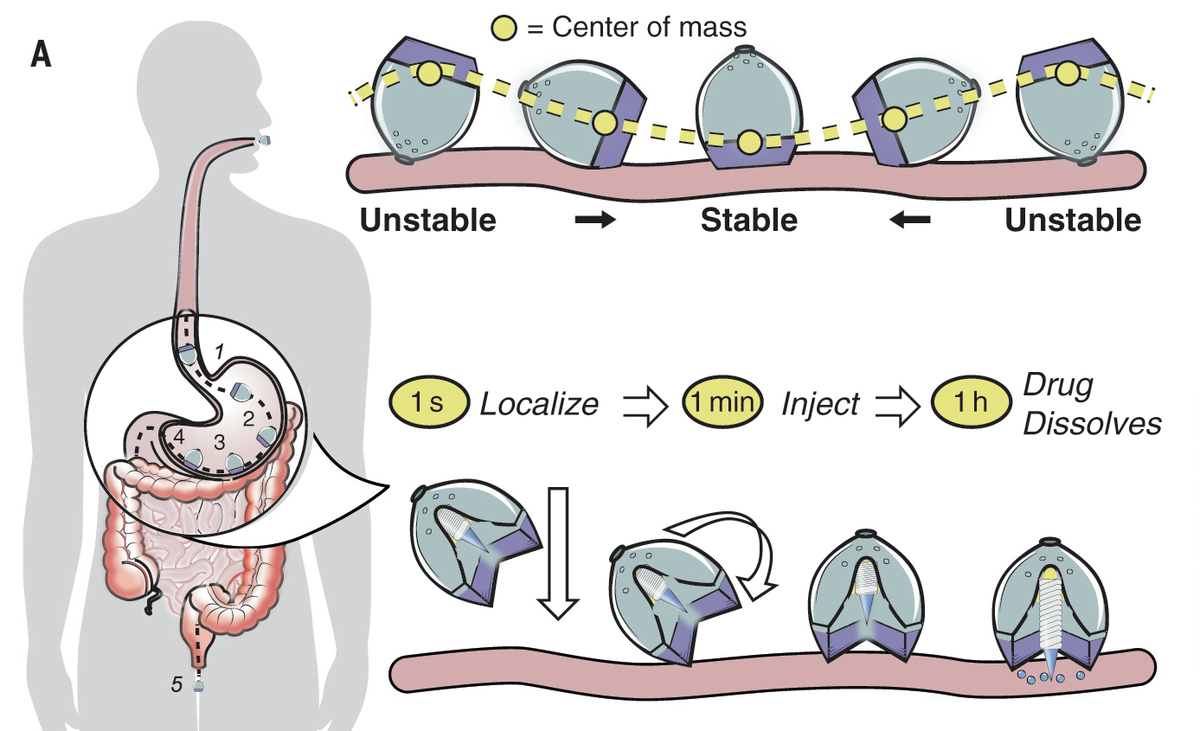
One team of scientists, from MIT’s Koch Institute for Integrative Cancer Research and Harvard’s Brigham and Women’s Hospital, developed a system to deliver insulin that actually still uses a needle — but is so small you can swallow it and the injection doesn’t hurt.
They built a pea-size device containing a spring that ejects a tiny dart of solid insulin into the wall of the stomach, says gastroenterologist Carlo Giovanni Traverso, an associate physician at Brigham and Women’s Hospital.
“We chose the stomach as the site of delivery because we recognized that the stomach is a thick and robust part of the GI tract,” Traverso says.
Once the device gets into the stomach, the humidity there allows the spring to launch the insulin dart.
So far so good, but Traverso says there was a problem the team had to overcome: “How do we get these devices to self-orient such that the end that is doing the injecting part is in direct contact with a tissue?”
To get it to roll into the right position all on its own, they turned to nature.
“Leopard tortoises happened to have evolved a way of doing this,” Traverso says. The shape of the tortoise shell helps the turtle flip over if it happens to wind up on its back.
And there was another source of inspiration: Weebles, those egg-shape toys that wobble but don’t fall down.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The self-righting capsule orients itself inside the stomach and ejects a tiny dart of solid insulin that’s about a quarter of an inch long.
Ania Hupalowska, Alex Abramson, Muhammad Mahdi Karim/Science
hide caption
toggle caption
Ania Hupalowska, Alex Abramson, Muhammad Mahdi Karim/Science
As the researchers report in the journal Science, they’ve tested the device on pigs, and it can deliver a therapeutic dose of insulin provided the pig has an empty stomach.
Traverso and his colleagues have been working with the global health care company Novo Nordisk to ready the device for human testing. He has received consulting fees from the company and is a co-inventor on patent applications describing oral biologic delivery. Traverso hopes their device will be ready for human tests in a few years.
On the other side of the U.S., nanoengineer Ronnie Fang of the University of California, San Diego and his colleagues have a different delivery system. Theirs is a kind of ingestible microrocket, about the size of a grain of sand, that is designed to zip past the stomach and into the small intestine.
“It actually propels [itself] using bubbles in a reaction of magnesium with biological fluids,” Fang says.
The rocket has a coating that protects its payload from the acidic and enzyme-filled environment of the stomach. Once the rocket enters the small intestine, the change in acidity causes the coating to dissolve and lets the rocket stick to the intestinal wall to release its payload, in this case a vaccine protein.
Much like Traverso’s design was inspired by the shape of a tortoise shell, the bubble-propelled microrocket travels like a bacterium.
“If you had bacteria invade your gut, they’re not just going to be sitting around statically, they’re going to be swimming around, and they’re going to make it to the intestinal wall,” Fang says.
As Fang and his colleagues report in Nano Letters, their delivery system works in mice, but human testing is probably many years off.