2 Nurses In Tennessee Preach ‘Diabetes Reversal’
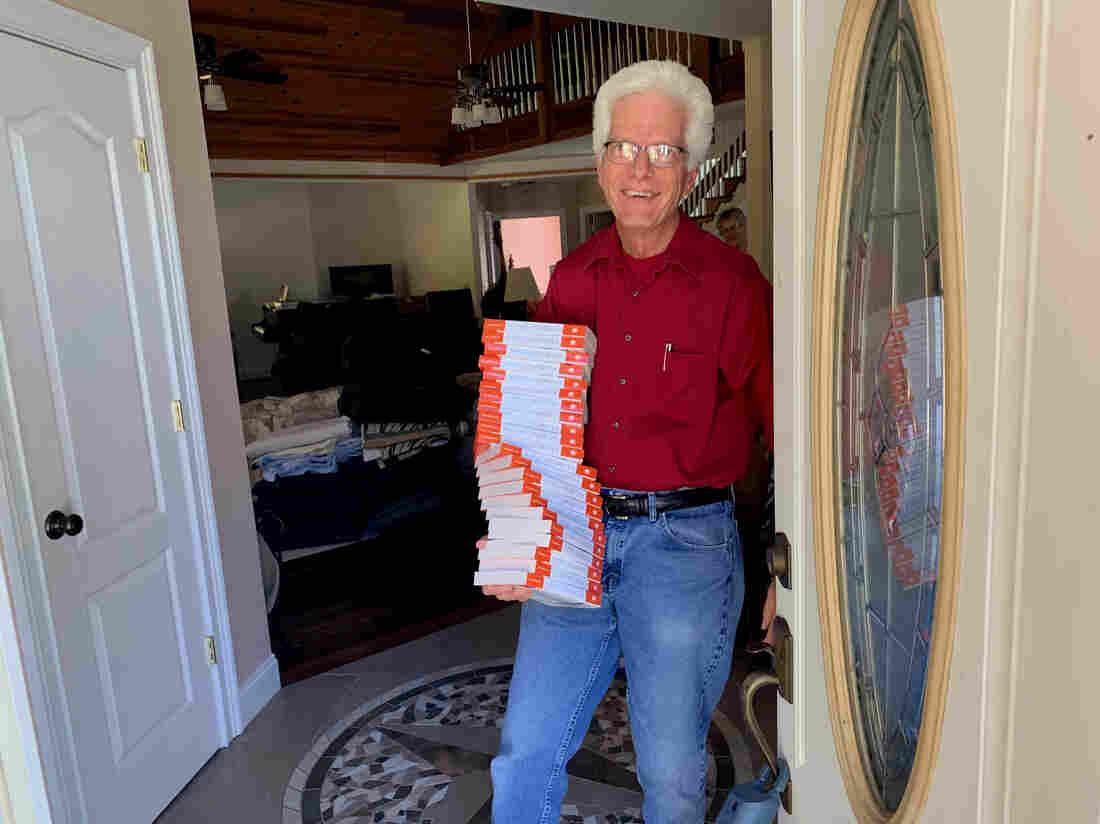
Steve Wickham, at home in Grundy County, Tenn., has developed an educational seminar with his wife, and fellow nurse, Karen, that they are using to help people with Type II diabetes bring blood sugar under control with less reliance on drugs.
Blake Farmer/WPLN
hide caption
toggle caption
Blake Farmer/WPLN
Chains, saws and old logging equipment litter the back field of Wendy Norris’ family farm, near the county seat of Altamont, Tenn. Norris used to be part of the local timber industry, and the rusted tools are relics from a time when health woes didn’t hold her back from felling hardwoods.
“I was nine months pregnant,” Norris says. “Me and my husband stayed about 10 or 15 miles in the middle of nowhere, in a tent, for a long time.”
Those outdoor adventures are just a memory now. A few years ago, as Norris turned 40, her feet started going numb. She first assumed it was from standing all day at her job at a nursing home.
“But it wasn’t,” she recalls now. “It was that neuropathy, where my [blood] sugar was high and I didn’t know it.” Norris had developed Type 2 diabetes.
Grundy County, Tenn., has a long list of public health challenges, and Type 2 diabetes tops the list. The county is stunningly scenic; it also has one of the lowest life expectancy rates in the region.
Norris was relatively active. She also enjoyed sodas, sweets and frozen dinners. Meanwhile, diabetes runs in her family. So, when her diabetes diagnosis came down, her doctor prescribed insulin shots and told her to watch what she ate.
“You’re sitting there thinking, ‘Well, what does that mean?’ ” Norris says.
Type 2 diabetes can be reversed with weight loss and exercise; but research shows that people need lots of help to achieve control of blood sugar with just a change in diet and lifestyle, and they rarely get enough support. It’s easier for doctors and patients to rely primarily on medication.
Norris says trying to overhaul her diet by herself was confusing and difficult. And when things didn’t change, the doctor just kept increasing her dosage of insulin.
But then Norris lost her health insurance. The injectable insulin cost her hundreds of dollars a month — money she simply didn’t have.
Fortunately, that’s when a couple of nurses who were members of her community stepped in to help — not with cash, but with crucial support of a different sort.
At the nonprofit Beersheba Springs Medical Clinic, a nonprofit clinic founded in 2010 to bring free or low-cost health care to the area, Norris was introduced to an alternative approach to taming her Type 2 diabetes — and the prospect of reversing her diagnosis altogether.
Retired nurses on a mission
In a former parsonage near the clinic, Karen Wickham ladles out lentil stew as a handful of participants in the evening’s health education session arrive.
She and her husband, Steve, are white-haired, semiretired nurses who have dedicated their lives to what they call “diabetes reversal.” They offer six-week seminars to Type 2 patients like Norris, who has also brought along her father and daughter.
“It’s our purpose,” Karen says. “Our purpose in life is to try to help make a difference — first in our community.”
With slide presentations, the Wickhams explain the difference between sucrose and glucose and the science behind the fact that foods like potatoes spike blood sugar, while sweet potatoes don’t. They preach eating as much fiber as a stomach can stand and dropping almost every kind of sweetened beverage.

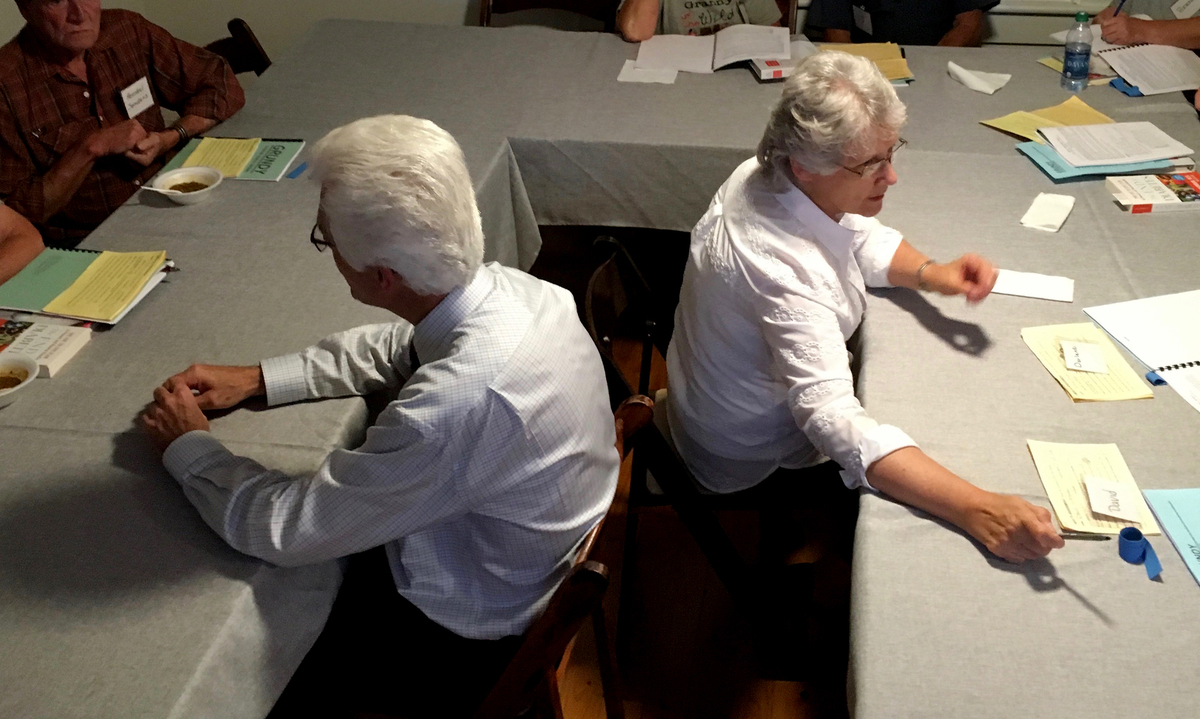
Steve and Karen Wickham explain course materials to participants in their seminar on Type 2 diabetes in Grundy County, Tenn. The six-week seminar offers detailed instruction on the biology of diabetes, diet and exercise — and provides plenty of individualized support.
Blake Farmer/WPLN
hide caption
toggle caption
Blake Farmer/WPLN
Then they demonstrate ways to burn all those calories. On one evening, Steve invents the “Beersheba Boogie” on the spot, asking participants to raise their knees and pump their fists in place.
All these people will have to find a way to get active at home, because there’s no gym anywhere close. There’s not a proper grocery store nearby either, so healthy cooking can become a real chore. These communitywide obstacles reveal why it can be a struggle for people to maintain their health in rural America. But the Wickhams are working to overcome those barriers.
Steve calls out for applause as participants share their latest health stats — “Her blood sugar is going down! Give her a hand.”
If it sounds like a revival meeting, it kind of is. Steve and Karen Wickham feel compelled to do this work as part of their Christian faith as Seventh-day Adventists — members of a denomination known for a focus on health.
“I think God holds us responsible for living in the middle of this people and doing nothing,” Steve says.
The Wickhams originally moved to Grundy County to take care of ailing parents, and they ended up building their dream home there. They planted vast orchards, vegetable gardens and berry patches to help satisfy their vegetarian diet — a diet common among Seventh-day Adventists.
But once settled in their mountain retreat, the Wickhams grew disturbed by Grundy County’s national health ranking: The county of 13,000 people ranks as the least healthy in Tennessee, by one annual measure. Grundy County has the shortest life expectancy in the state and an elevated rate of diabetes (16 percent of adults), which can eventually result in blindness, kidney failure and amputations.
“I had taken care of diabetic patients for so long, and I knew the progression,” Karen says. “If you truly want the people to get better, you have to treat it with lifestyle interventions.”
Overhauling one’s diet and activity level is the obvious answer, but those changes are hard to start and even harder to maintain.
“Nobody, actually, will make all of the lifestyle changes that we recommend,” Steve says. “But if you’re making the kind of choices that lead you to a healthier lifestyle, then you get better.”
A more hopeful message
Along with their lifestyle counseling, the Wickhams always give a disclaimer, advising people to consult with their doctors about their condition and its treatment. They also acknowledge that their seminars are not yet “evidence based” or backed by peer-reviewed scientific literature. It’s one of the reasons they haven’t been able to get government grants to fund their program directly.
But there are studies showing that people with blood sugar levels in the “prediabetes” range can get back to normal blood sugar by losing 5% of their body weight.
And weight loss and exercise have already been shown to lower hemoglobin A1c levels, which physicians use to monitor a patient’s blood sugar over two to three months.
In addition, new research from Dr. Roy Taylor of Newcastle University in the United Kingdom shows promise for true remission.
“There just hasn’t been the information about the possibility of reversing diabetes,” Taylor says.
Most studies do show Type 2 diabetes, in most patients, marching in pretty much one direction. But Taylor says those studies also involve people who continue to gain weight, which is typical among diabetics.
“Doctors tell their patients, ‘You’ve got a lifelong condition. We know it’s going to steadily get worse.’ Then they turn around, and their patients aren’t losing weight or doing exercise, but they’ve given them this utterly depressing message,” he says.
Taylor’s research finds that if a patient loses 30 pounds or so, diabetes can be reversed in its early stages. Taylor prescribes a strict liquid diet and limited exercise — at first — so as not to stimulate the appetite. People with Type 2 diabetes need to lose fat from the liver and pancreas.
Ultimately, Taylor hopes better nutrition will become the preferred response to high blood sugar in the next decade.
“I think the main headwinds [against progress] are just conceptual ones — of scientists and doctors believing this is an irreversible condition because of what we’ve seen,” he says.
Even the American Diabetes Association has been changing its views. The advocacy group has a new position on Type 2 reversal: “If a patient wishes to aim for remission of type 2 diabetes, particularly within 6 years of diagnosis, evidence-based weight management programs are often successful.”
John Buse, chief of endocrinology at the University of North Carolina medical school, helped write the American Diabetes Association’s revised guidance. “We’ve known, literally since the 17th century, that diet is the key to managing diabetes,” he says.
But it’s hard to write a prescription for lifestyle change.
“Doctors don’t have the time to do it well, so we have often used the sort of short shrift,” he says. ” ‘Eat less carbohydrates and walk every day.’ That has basically no impact.”
The Wickhams are doing their part to add to the scientific data, tracking the blood sugar of the participants in their program. And even the anecdotal, short-term evidence they’ve gathered so far is resonating far beyond Grundy County, and they’ve been traveling more and more lately.

Steve Wickham, who is a nurse, draws blood at the midpoint of his and his wife Karen’s six-week diabetes seminar. The hemoglobin A1c levels measured by the lab test help patients monitor whether the diet and exercise changes they’re engaged in are making a difference in their blood sugar levels.
Blake Farmer/WPLN
hide caption
toggle caption
Blake Farmer/WPLN
The couple just sold their retirement home so they can say yes to all the invitations they’ve received, mostly through Seventh-day Adventist groups, to present their program to other communities around the United States.
Meanwhile, Wendy Norris says the prospect of turning back Type 2 diabetes already has changed her entire outlook on health.
“I felt like I was stuck having to take three or four shots a day the rest of my life,” she says. “I’ve got it down to one already.”
This story is part of NPR’s reporting partnership with Nashville Public Radio and Kaiser Health News.
First Came Kidney Failure, Then There Was The $540,842 Bill For Dialysis

Sovereign Valentine and his wife, Jessica, wait as a dialysis machine filters his blood. Before finding a dialysis clinic in their insurance network, the Valentines were charged more than a half-million dollars for 14 weeks of treatment.
Tommy Martino/Kaiser Health News
hide caption
toggle caption
Tommy Martino/Kaiser Health News
For months, Sovereign Valentine had been feeling progressively run-down. The 50-year-old personal trainer, who goes by “Sov,” tried changing his workout and diet to no avail.
Finally, one Sunday, he drove himself to the hospital in the small town of Plains, Mont., where his wife, Jessica, happened to be the physician on call. “I couldn’t stop throwing up. I was just toxic.”
It turned out he was in kidney failure and needed dialysis immediately.
“I was in shock, but I was so weak that I couldn’t even worry,” he said. “I just turned it over to God.”
He was admitted to a nearby hospital that was equipped to stabilize his condition and to get his first dialysis session. A social worker there arranged for him to follow up with outpatient dialysis, three times a week. She told them Sov had two options, both about 70 miles from his home. They chose a Fresenius Kidney Care clinic in Missoula.
Share Your Story And Bill With Us
If you’ve had a medical-billing experience that you think we should investigate, you can share the bill and describe what happened here.
A few days after the treatments began, an insurance case manager called the Valentines warning them that since Fresenius was out-of-network, they could be required to pay whatever the insurer didn’t cover. The manager added that there were no in-network dialysis clinics in the state, according to Jessica’s handwritten notes from the conversation.
Jessica repeatedly asked both the dialysis clinic staff and the insurer how much they could expect to be charged, but couldn’t get an answer.
Then the bills came.
Patient: Sovereign Valentine, 50, a personal trainer in Plains, Mont. He is insured by Allegiance, through his wife’s work as a doctor in a rural hospital.
Total bill: $540,841.90 for 14 weeks of dialysis care at an out-of-network Fresenius clinic. Valentine’s insurer paid $16,241.72. The clinic billed Valentine for the unpaid balance of $524,600.17.
Service provider: Fresenius Medical Care, one of two companies (along with rival DaVita) that control about 70% of the U.S. dialysis market.
Medical treatment: Hemodialysis at an outpatient Fresenius clinic, three days a week for 14 weeks.
What gives: As the dominant providers of dialysis care in the U.S., Fresenius and DaVita together form what health economists call a “duopoly.” They can demand extraordinary prices for the lifesaving treatment they dispense — especially when they are not in a patient’s network. A 1973 law allows all patients with end-stage renal disease like Sov to join Medicare, even if they’re younger than 65 — but only after a 90-day waiting period. During that time, patients are extremely vulnerable, medically and financially.

“To me, it’s so outrageous that I just have to laugh,” said Sov Valentine about the huge bill for dialysis treatments he received.
Tommy Martino/Kaiser Health News
hide caption
toggle caption
Tommy Martino/Kaiser Health News
Fresenius billed the Valentines $524,600.17 — an amount that is more than the typical cost of a kidney transplant. It’s also nearly twice Jessica’s medical school debt. Fresenius charged the Valentines $13,867.74 per dialysis session, or about 59 times the $235 Medicare pays for a dialysis session.
When Jessica opened the first bill, she cried. “It was far worse than what I had imagined would be the worst-case scenario,” she said.
Sov had a different reaction: “To me, it’s so outrageous that I just have to laugh.”
Dialysis centers justify high charges to commercially insured patients because they say they make little or no money on the rates paid for their Medicare patients, who — under the 1973 rule — make up the bulk of their clientele. But nearly $14,000 per session is extraordinary. Commercial payers usually pay about four times the Medicare rate, according to a recent study.
Dialysis companies are quite profitable. Fresenius reported more than $2 billion in profits in 2018, with the vast majority of its revenue coming from North America.
The discrepancy in payments between Medicare and commercial payers gives dialysis centers an incentive to treat as many privately insured patients as possible and to charge as much as they can before dialysis patients enroll in Medicare. It may also give dialysis centers an incentive to charge the few out-of-network patients they see outlandish prices.
“The dialysis companies may think they can get closer to what they want from the health plans by staying out-of-network and charging these prices that are totally untethered to their actual costs,” said Sabrina Corlette, a professor at Georgetown University’s Health Policy Institute. “They have the health plans over a barrel.”
One potential way to save costs on dialysis is to switch to a type that can be done at home, which involves infusing fluid into the abdomen. Called peritoneal dialysis, it is common in Europe but relatively rare in the U.S. In an executive order this month, President Trump announced new incentives to increase uptake of those options.
Brad Puffer, a spokesman for Fresenius Medical Care North America, said the company would not comment on any specific patient’s situation.
“This is one example of the challenges that can arise from a complex healthcare system in which insurers are increasingly shifting the financial burden to patients,” Puffer said in a written statement. “The insurance company should accurately advise patients of in- and out-of-network providers. It is the patient’s choice when they receive that information as to which provider they select.”
Resolution: As a physician, Jessica Valentine is savvy about navigating the insurance system. She knew it was important to find an in-network provider of dialysis. She and the insurance company case manager both searched on the insurer’s online provider directory, she said, and were unable to find one. She even wrote to the Montana insurance commissioner to inquire if the lack of a dialysis provider violated a requirement that insurers maintain an “adequate network” of providers.
With help from the state insurance commissioner, she learned that there was, in fact, an in-network dialysis clinic run by a nonprofit organization that had not turned up in her insurer’s online search or the directory. She immediately arranged for Sov to start getting further dialysis there. But the bills with Fresenius, meanwhile, were adding up.
After a reporter made inquiries, a financial counselor at Fresenius told Jessica that the Valentines qualified for a discount of 50%, based on their income. That would still leave them a bill of $262,400.08.
“It’s still a completely outrageous charge,” Jessica said. “I want to pay what we owe and what’s reasonable and what his care actually cost.”
Unwilling to pay Fresenius more, Allegiance said Jessica should have found the in-network facility earlier. “There is always the potential for customers to misunderstand information about how their health plan works, especially in stressful situations,” a spokesperson for Allegiance wrote.
Jessica is considering contacting a lawyer. If all else fails, the Valentines will consider filing for bankruptcy. A family doctor who works at a rural hospital, Jessica now understands why some of her patients avoid testing and treatment for fear of the cost. “It’s very, very frustrating to be a patient, and it’s very disempowering to feel like you can’t make an informed choice because you can’t get the information you need.”
The takeaway: Dialysis is a necessary, lifesaving treatment. It is not optional — no matter a patient’s financial situation.
Insurers are obligated to have adequate networks for all covered medical services in their plans, though “adequacy” is poorly defined.
So, if it looks like there isn’t an in-network option within a reasonable distance — for dialysis or more basic services from orthopedists or dermatologists — keep digging. Keep in mind that dialysis clinics may be listed as “facilities” rather than “providers” in your directory.
If none are available, seek help from your state’s insurance commissioner. Report your experiences — that’s one way the commissioner can learn that the names listed in the directory aren’t taking patients or are 50 miles away, for example.
If you have insurance through an employer, you can contact your benefits department to go to bat for you. If there is no in-network option, you should get a dispensation to go out-of-network at in-network rates and with in-network copayments.
If you receive a bill for out-of-network care, don’t merely write the check. Ask for an itemized bill and review the charges. You can also ask your insurance company to negotiate with the provider on your behalf. See if the bill counts as a “surprise bill” under your state’s law, in which case you could be “held harmless” from excessive charges.
And when all else fails, try to negotiate directly with the provider. They might have a financial assistance policy, or be willing to lower the cost significantly to avoid turning you over to a debt collector that would pay them pennies on the dollar.
NPR produced and edited the interview with Kaiser Health News’ Elisabeth Rosenthal for broadcast. Nick Mott of Montana Public Radio provided audio reporting.
Bill of the Month is a crowdsourced investigation by Kaiser Health News and NPR that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it here.
What’s Happening With New Abortion Regulations Under Title X

Clare Coleman, CEO of the National Family Planning and Reproductive Health Association, talks with NPR’s Sarah McCammon about recent changes to Title X regulations.
Ireland’s Shane Lowry Wins British Open In His First Major Title

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examining Biden’s Health Care Pitch
New York Times health reporter Sarah Kliff tells NPR’s Lulu Garcia-Navarro about Joe Biden’s health care plan and how it differs from “Medicare for All.”
LULU GARCIA-NAVARRO, HOST:
We’re going to talk policy now – health care policy. That’s because there’s another prescription for the American health care system in the mix among the Democratic presidential field. And it doesn’t call for as sweeping a change as other plans do.
(SOUNDBITE OF ARCHIVED RECORDING)
JOE BIDEN: I understand the appeal of “Medicare for All.” But folks supporting it should be clear that it means getting rid of Obamacare. And I’m not for that.
GARCIA-NAVARRO: That’s former Vice President Joe Biden announcing his plan on Monday. Let’s take a look at his idea and other plans not calling for expanding Medicare to cover everyone with Sarah Kliff. She covers health care for The New York Times. And she joins us now. Good morning.
SARAH KLIFF: Good morning.
GARCIA-NAVARRO: Biden’s pitch is for Obamacare plus. What does that mean?
KLIFF: Yeah. This is a really key divide you’re seeing shape up in the Democratic field. What Biden and a number of other candidates are suggesting is something called the public option, keeping the private insurance that we have now but adding in a government-run option that is going to compete against the profit-motivated plans. And if things go as you think in theory, it will have lower premiums. People will sign up for it. And that should encourage other health care plans to lower their premiums, as well, essentially creating more competition in the private-insurance market.
GARCIA-NAVARRO: Where does this fit on the spectrum of plans you’re seeing from the Democrats? I imagine you put Bernie Sanders on one end because he wants a single-payer system that eliminates private health insurance in favor of the government covering everyone. Does this put Biden squarely in the middle?
KLIFF: It’s almost to the right of the spectrum at this point, which is a really wild thing to think about, about how the public option used to be a pretty far-left position, that this is where the liberals in Congress would land. Now the left is really focused on Medicare for All, like Senator Sanders says, eliminating private health insurance, moving everyone to a government plan. The more moderate position has become, let’s build on Obamacare. Let’s add in this public option. So I almost see this as the benchmark that’s being suggested in the Democratic primary. And you wouldn’t have seen that even five, 10 years ago.
GARCIA-NAVARRO: Speaking as someone who’s been reporting on health care in the U.S. for a long time now, what are the obvious advantages and disadvantages in a plan like Biden’s?
KLIFF: So I think one of the obvious advantages is that it’s a lot less of a transition, that it would be a huge, huge undertaking to move all of us onto a government health care plan and do it in four years, which is what Senator Sanders’ plan envisions, whereas the Biden plan would not be quite as disruptive. It can advertise choice. You could decide if you want private insurance, if you want the new public plan. But, you know, the things that are the advantage are the exact same things that are the disadvantage. It will not disrupt as many of the things that people don’t like about their health insurance. It won’t, for example, regulate all the health care prices in the United States, which is something the Sanders plan would do. It would probably eliminate a lot of the big surprise bills that I see a lot of my readers sending me. So the fact that it’s less disruptive – that has its advantages – also has its disadvantages, as well.
GARCIA-NAVARRO: So where is the public on this now?
KLIFF: Yeah. So they are warming up to Medicare for All, is what I would say. If you look at the trajectory of polling over the past 20 years, it’s not like there’s some groundswell of support for Medicare for All. Instead, you see a slow, steady, incremental increase in those who think it’d be a good idea for the government to provide health insurance to everybody. But what I find most interesting about the Medicare for All polling is that people really change their minds when they hear different things about it. When people learn Medicare for All would get rid of the insurance they have at work, they get much more negative. When they hear it would get rid of deductibles, they get a lot more positive. So I don’t think the country’s really made up their mind at this point. And that’s why you see this fight in the Democratic Party – is because people are trying to sell their pitch for what would be best for our health care system.
GARCIA-NAVARRO: In the 2018 election, health care became a really strong issue for the Democrats. On the other side of the aisle, what are the Republicans offering? What can President Trump bring to the table?
KLIFF: So President Trump – he does like to talk a lot about having a great, new health care plan. But we haven’t really seen the Republican Party unify around their vision of health care. We spent most of 2017 watching them try and repeal and replace Obamacare. And they were unable to come up with a plan that their caucus agreed on that could pass through Congress. Right now, Republicans are pursuing this lawsuit in Texas that would overturn the Affordable Care Act. And you’ll see Democrats talking a lot about that lawsuit – the Trump administration supporting Obamacare repeal in that particular legal battle. So, you know, you have President Trump discussing a lot of big promises for a good health care plan. You also have the Department of Justice supporting a lawsuit that would end protections for pre-existing conditions. And that’s something I think you’re going to see come up a lot as we get into the election cycle.
GARCIA-NAVARRO: That’s Sarah Kliff of The New York Times, speaking via Skype. Thanks so much.
KLIFF: Thank you.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Former Planned Parenthood CEO On Leadership Upheaval
NPR’s Sarah McCammon talks to Pamela Maraldo, former CEO of Planned Parenthood. She left the organization under similar circumstances as Dr. Leana Wen, who was ousted from her position this week.
Sports Roundup: Previewing Sunday’s Baseball Hall Of Fame Induction
NPR’s Scott Simon speaks with ESPN’s Howard Bryant about the 2019 baseball season so far and about Mariano Rivera, baseball’s first unanimous Hall of Famer.
SCOTT SIMON, HOST:
Now, time for sports.
(SOUNDBITE OF MUSIC)
SIMON: The 2019 baseball season heats up the summer – the first unanimous Hall of Famer – joined now by Howard Bryant of ESPN, who gets a vote in the Hall of Fame ballot. Howard, thanks so much for being with us.
HOWARD BRYANT: Good morning, Scott. How are you?
SIMON: I’m fine, thank you, sir. I saw two games at Wrigley Field this week. I’m great.
BRYANT: (Laughter).
SIMON: Three teams, now with more than 60 wins in Major League Baseball – the Yanks in the AL East, the Dodgers in the NL West, the Astros in the AL West – they’re scorching, aren’t they?
BRYANT: Yeah, they are. And once again, this is my second-favorite time of the year where you come out of the All-Star break and you start looking at teams and wondering, OK, who’s built for the entire season, and who’s going to wilt as the dog days of August commence?
And I kind of feel like these three teams are great. They’re really, really good. I mean, I – you look at the Dodgers. They’re an incredibly hungry team. They went to the World Series back-to-back years. They got beat twice. The Astros got them in 2017. The Red Sox got them last year.
You look at the Astros, who, of course, won the World Series two years ago and then, of course, the Yankees, who have been building and building for this for the last couple years. They sort of surprised everyone a couple years ago. The Red Sox got them last year. And now they are just an amazing offensive team, and they’re doing it with a lot of – well, a lot of their best players have been injured. Giancarlo Stanton isn’t even on the field right now, and the Yankees are just steamrolling everybody.
SIMON: Washington Nationals have really caught fire, too – haven’t they? – without Bryce Harper.
BRYANT: Exactly, and that’s the team that – they were, I think, 11 or 12 games under 500 earlier in the season, and now they’re in second place. They lost a tough one last night to the Braves. But I feel like this is another team that – they’ve got something to prove, as well. And especially, you’ve got those two pitchers – you’ve got Scherzer, you’ve got Strasburg – and that’s a pretty good start. I think any team in baseball would like their chances when you start the rotation with those two guys.
SIMON: And…
BRYANT: So – and let’s not forget the Twins in…
SIMON: Yep.
BRYANT: …The American League Central. And right behind them is Cleveland. There’s – and of course, the team that I used to cover, the Oakland A’s, are probably the second-hottest team in baseball. So it’s really funny, Scott. You have so many times that people talk about baseball and – oh, there’s no salary cap, and no one’s got a chance to win. And look at all of these teams that are out there who are – exactly. And by the way, they say it in that accent, as well. They say…
SIMON: I know.
BRYANT: …It just like that, right? But it’s true.
SIMON: NL Central, I just want to mention, ’cause you have a great three-way race between the Cubs…
BRYANT: And I didn’t even mention your Cubs. Exactly.
SIMON: …Who aren’t first, but the Brew Crew from Milwaukee and the Cards are close. And even the Bucs have a chance.
BRYANT: Well, and let’s not forget that last year, the Brewers were in the NLCS. So they’re close, as well. There’s a lot of teams that could win this thing, so instead of just talking about baseball being, you know, one team or two teams that can’t win – baseball actually has the most parity of all the sports.
SIMON: Baseball’s Hall of Fame abduction – abduction (laughter) – Area 51 stuff…
BRYANT: (Laughter) Baseball’s induction.
SIMON: …Induction is tomorrow. I know you get a Hall of Fame vote. Mariano Rivera, the great Yankee, is the Hall’s first unanimous inductee.
BRYANT: Indeed. And I had been withholding my vote for a couple of years because I was conflicted about steroids and conflicted about the commissioner and company inducting themselves into the Hall of Fame while allowing us the players – the voters to punish the players. And I hadn’t been a fan of that. But when it came to Rivera and also the death of Roy Halladay, I felt like I needed to vote. And so I voted this year.
And Mariano Rivera – I covered Mariano and Mike Mussina, who are both getting in. I covered both of them in the – with the Yankees in the early 2000s. And it should have happened before, but the fact that it’s Rivera – you can’t argue that. Edgar Martinez – everybody in Seattle would be very happy about that. And, Scott, you should be – what should I say? – ashamed that you’ve never been to Cooperstown. You got to go.
SIMON: Yeah. All right. Well, we’ll go together sometime. Howard Bryant of ESPN. Thanks so much.
BRYANT: Thank you.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Radical or Incremental? What’s Really In Joe Biden’s Health Plan
{kind=link}
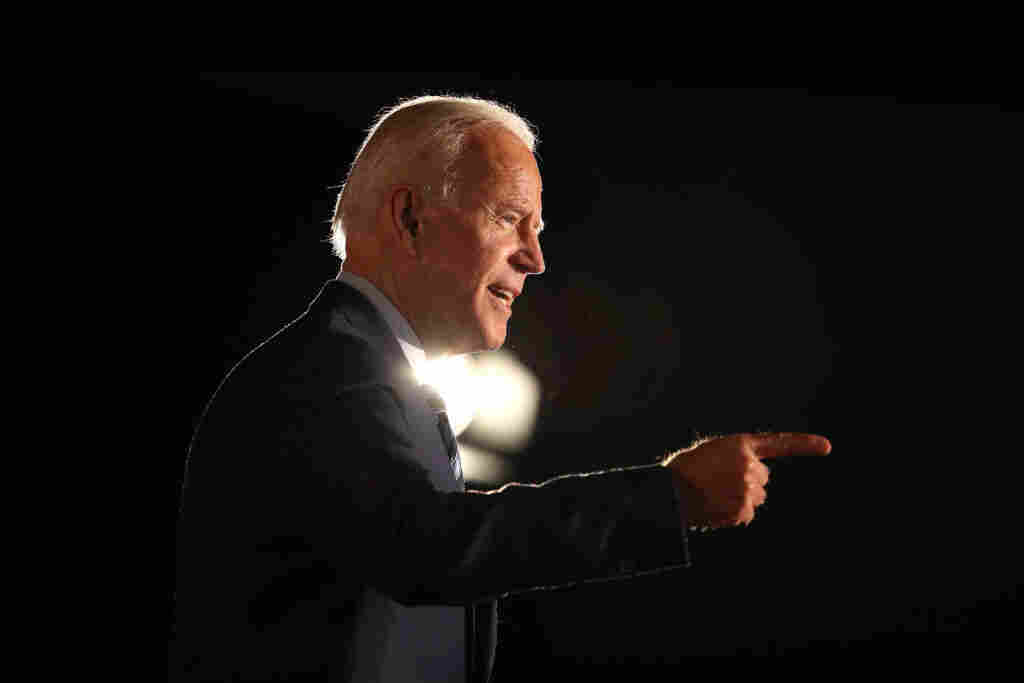
Opponents running to Joe Biden’s left say his health plan for America merely “tinkers around the edges” of the Affordable Care Act. But a close read reveals some initiatives in Biden’s plan that are so expansive they might have trouble passing even a Congress held by Democrats.
Justin Sullivan/Getty Images
hide caption
toggle caption
Justin Sullivan/Getty Images
The headlines about presidential candidate Joe Biden’s new health care plan called it “a nod to the past” and “Affordable Care Act 2.0.” That mostly refers to the fact that the former vice president has specifically repudiated many of his Democratic rivals’ calls for a “Medicare for All” system, and instead sought to build his plan on the ACA’s framework.
Sen. Bernie Sanders, one of Biden’s opponents in the primary race and the key proponent of the Medicare for All option, has criticized Biden’s proposal, complaining that it is just “tinkering around the edges” of a broken health care system.
Still, the proposal put forward by Biden earlier this week is much more ambitious than Obamacare – and despite its incremental label, would make some very controversial changes.
“I would call it radically incremental,” says Chris Jennings, a political health strategist who worked for Presidents Bill Clinton and Barack Obama and who has consulted with several of the current Democratic candidates.
Republicans who object to other candidates’ Medicare for All plans find Biden’s alternative just as displeasing.
“No matter how much Biden wants to draw distinctions between his proposals and single-payer, his plan looks suspiciously like “SandersCare Lite,” writes former congressional aide and conservative commentator Chris Jacobs in a column for The Federalist.
Biden’s plan is built on the idea of expanding the ACA to reduce costs for patients and consumers — similar to what Hillary Clinton campaigned on in 2016. It would do things Democrats have called for repeatedly since the ACA was passed. Among Biden’s proposals is a provision that would “uncap” federal help to pay for health insurance premiums — assistance now available only to those with incomes that are 400% of the poverty level, or about $50,000 for an individual.
Under Biden’s plan, no one would be required to pay more than 8.5 percent of their income toward health insurance premiums.
But it includes several proposals that Congress has failed repeatedly to enact, including some that were part of the original debate over the ACA. Plus, Biden’s plan has some initiatives that are so expansive, it is hard to imagine them passing Congress — even if Democrats sweep the presidency and both houses of Congress in 2020.
Here are some of the more controversial pieces of the Biden health plan:
Public option
Although many of the Democratic presidential candidates have expressed varying degrees of support for a Medicare for All plan, nearly all have also endorsed creating a government-sponsored health plan, known colloquially as a “public option,” that would be available to people who buy their own health insurance. That eligible group would include anyone who doesn’t get insurance through their job or who doesn’t qualify for other government programs, like Medicare or Medicaid.
A public option was included in the version of the ACA that passed the House in 2009. But its proponents could not muster the 60 votes needed to pass that option in the Senate over GOP objections — even though the Democrats had 60 votes at the time.
Biden’s public option, however, would be available to many more people than the 20 million or so who are now in the individual insurance market. According to the document put out by the campaign, this public option also would be available to those who don’t like or can’t afford their employer insurance, and to small businesses.
Most controversial, though, is that the 2.5 million people currently ineligible for either Medicaid or private insurance subsidies because their states have chosen not to expand Medicaid would be automatically enrolled in Biden’s public option, at no cost to them or the states where they live. Also included automatically in the public option would be another 2 million people with low incomes who currently are eligible for ACA coverage subsidies – and who would also be eligible for expanded Medicaid.
That part of Biden’s proposal has prompted charges that the 14 states that have so far chosen not to expand Medicaid would save money, compared with those that have already expanded the program, because expansion states have to pay 10% of the cost of that new population.
Jennings, the Democratic health strategist, argues that extra charge to states that previously expanded Medicaid would be unavoidable under Biden’s plan, because people with low incomes in states that haven’t expanded Medicaid need coverage most. “If you’re not going to have everyone get a plan right away, you need to make sure those who are most vulnerable do,” Jennings says.
Abortion
The Biden plan calls for eliminating the “Hyde Amendment,” an annual rider to the spending bill for the Department of Health and Human Services that forbids the use of federal funds to pay for most abortions. Biden recently ran into some difficulty when his position on the Hyde ammendment was unclear.
Beyond that, Biden’s plan also directly calls for the federal government to fund some abortions. “[T]he public option will cover contraception and a woman’s constitutional right to choose,” his plan says.
In 2010, the Affordable Care Act very nearly failed to become law after an intraparty fight between Democrats who supported and opposed federal funding for abortions. Abortion opponents wanted firm guarantees in permanent law that no federal funds would ever be used for abortion; abortion-rights supporters called that a deal breaker. Eventually a shaky compromise was reached.
And while it is true that there are now far fewer Democrats in Congress who oppose abortion than there were in 2010, the idea of even a Democratic-controlled Congress voting for federal abortion funding seems far-fetched. The current Democratic-led House has declined even to include a repeal of the Hyde Amendment in this year’s HHS spending bill, because it could not get through the GOP-controlled Senate or get signed by President Trump.
Undocumented immigrants
When Obama said in a speech to Congress in September 2009 that people not in the U.S. legally would be ineligible for federal help with their purchase of health insurance under the ACA, it prompted the infamous “You lie!” shout from Rep. Joe Wilson, R-S.C..
Today, all the Democratic candidates say they would provide coverage to undocumented residents. There is no mention of them specifically in the plan posted on Biden’s website, although a Biden campaign official told Politico this week that people in the U.S. who are undocumented would be able to purchase plans on the health insurance exchanges, but would not qualify for subsidies.
Still, in his speech unveiling the plan at an AARP-sponsored candidate forum in Iowa, Biden did not address this issue of immigrants’ health care. He said only that his plan would expand funding for community health centers, which serve patients regardless of their ability to pay or their immigration status, and that people in the U.S. without legal authority would be able to obtain coverage in emergencies. That is already law.
U.S. Overdose Deaths Dipped In 2018, But Some States Saw ‘Devastating’ Increases

{kind=link}
Nationally, drug overdose deaths reached record levels in 2017, when a group protested in New York City on Overdose Awareness Day on August 31. Deaths appear to have declined slightly in 2018, based on provisional numbers, but nearly 68,000 people still died.
Spencer Platt/Getty Images
hide caption
toggle caption
Spencer Platt/Getty Images
Good news came out from the Centers for Disease Control and Prevention Wednesday: Preliminary data shows reported drug overdoses declined 4.2% in 2018, after rising precipitously for decades.
“It looks like this is the first turnaround since the opioid crisis began,” says Bertha Madras who served on President Trump’s opioid commission, and is a professor of psychobiology at Harvard Medical School.
She says it won’t be entirely clear until the CDC finalizes the numbers but, “I think the tide could be turning.”
But not everyone was celebrating. Some states actually saw double-digit increases.
“It’s deflating,” Rachel Winograd says. She’s an associate research professor at the University of Missouri-St. Louis. “It’s incredibly discouraging to see the increase in Missouri in 2018 that happened at the same time as we really ramped up so many efforts to save lives and improve lives in our state.”
The provisional data shows Missouri deaths increased by 17% — one of 18 states that saw a year-over-year increase.
Loading…
Don’t see the graphic above? Click here.
Over the last several years, Missouri has received $65 million in federal grants to address the opioid crisis, Winograd says, and she has helped the state decide where and how to spend that money. They’ve focused on expanding access to medication-assisted treatment, and “saturating our communities with naloxone — the opiate overdose antidote,” she says.
“Any scholar who’s been studying this epidemic will tell you that those are effective tools at saving lives. We’ve drastically increased access to those services and we know we’ve saved thousands of lives.
“The fact that the numbers didn’t go down and that people were dying at an even higher rate — it was devastating,” Winograd says.
The numbers out Wednesday are not final, notes Farida Ahmad, mortality surveillance lead of the National Center for Health Statistics at the CDC. She says they should be close to the final numbers, though. For provisional data, “our threshold is for 90% completeness,” she says.
Michael Botticelli, the executive director of the Grayken Center for Addiction at Boston Medical Center and formerly President Obama’s drug czar, says the geographic variation in drug deaths is troubling.
“I think it’s important to pay attention to and really understand what is happening in each of these states, and why are some states seeing dramatic increases versus those seeing dramatic decreases?” he says.
The reasons for this geographic variation are numerous. For one, this data only reflects the difference from one year to the next, so states that had a bad year in 2017, can show an improvement in 2018, even if the overall picture is still grim.
Another variable is fentanyl, the highly potent synthetic opioid that’s been responsible for a rising number of overdoses in recent years. Some states have a lot of fentanyl in their drug supply, and others do not.
“We saw increases all along the Mississippi river, and I would not be surprised if that was due to an increase in the proportion of fentanyl in their drug supply,” Winograd says. Deaths from fentanyl continue to rise, according to Ahmad from the CDC.
Other variations in the drug supply could contribute to the differences from state to state, says Christopher Ruhm, a professor of public policy at the University of Virginia. He notes stimulants have a different geographic spread than fentanyl, and those deaths are also on the rise.
“Some of this may be due to the nature of the drug epidemic in different places, some of it may also be due to how much we are providing medication-assisted treatment, and engaging in other policies to try to address this problem,” Ruhm says.
The social safety net also plays a role, says Winograd. In Missouri, “we just have fewer resources to help people in need,” she says.
“We have a lack of housing, incarceration rates are increasing — these are all connected and making the most vulnerable people in our society at highest risk of overdose deaths.”
Missouri was among five states that showed increased overdose numbers and had not expanded Medicaid, Winograd notes. Medicaid expansion means more people have coverage for addiction treatment, and research shows it’s making a difference.
Ohio was a bright spot on the 2018 map, showing a 22% decrease in 2018, although in raw numbers, it still had 4,000 reported deaths.
“It is still a nightmare. And the danger in media over-portraying this is actually quite substantial,” says Shawn Ryan, an addiction doctor in Ohio and past-president of the Ohio Society of Addiction Medicine. “If we look at just that decrease nationally — which is not that big — we’re missing the point. In order to get back to baseline, we have a very long way to go.”
In the CDC’s preliminary national numbers, 67,744 people are reported to have died from drug overdoses in 2018. Even though that’s several thousand less than died from drug overdoses in 2017, it’s still many, many more people than died of AIDS in the worst years of the crisis.
The decline should not be a signal to slow down efforts — or funding — to combat the epidemic, Ryan says.
He cites the proposed CARE Act, a legislative effort led by Senator Elizabeth Warren, D-Mass., and Representative Elijah E. Cummings, D-Md., which would allocate $100 billion over 10 years for addiction and recovery services. The CARE Act is modeled on the Ryan White Act, put in place to combat the AIDS epidemic.
“That’s actually much more in line with what’s needed,” says Ryan.
$100 billion would dwarf past federal funds for the epidemic. Grants from the State Targeted Response to the Opioid Crisis program, authorized by the 21st Century Cures Act, totaled $1 billion. In 2019, State Opioid Response federal grants are set to total $1.4 billion.
“If you look at the dollars spent to date, the fact that we’ve had the impact we’ve had is actually because of people being invested and working very hard for not that many dollars,” says Ryan.
Boticelli agrees that the only way to ensure the national trend continues is to adequately fund it. “We can’t look at a 5% reduction and say our work is done. I think it basically shows us that we have to redouble our efforts,” he says. “How are we going to ensure that states have the resources that they need to continue to focus energy on this epidemic?”
In a statement Wednesday, Health and Human Services Secretary Alex Azar celebrated the decline and indicated that federal funding won’t be going away. “By no means have we declared victory against the epidemic or addiction in general. This crisis developed over two decades and it will not be solved overnight,” Azar wrote.
Rachel Winograd says for her, the increase in deaths in Missouri is an indication that there’s much more to do.
“I am very proud of what Missouri has done. I don’t think we should have done anything differently,” she says. “And I do think that we’ve been even more aggressive than many of the states that saw decreases, in terms of our focus on evidence-based solutions.
“It’s not that we did the wrong thing — it’s that we didn’t do enough of the right thing,” she adds. “And we need more sustainable funding to do that.”
Carmel Wroth contributed reporting to this story.
Frenchman Julian Alaphilippe Leads Tour De France As Race Enters Second Half
NPR’s Ari Shapiro speaks with Damian McCall, a reporter for the Agence France-Presse, about this year’s Tour de France and the Frenchman currently in the lead, Julian Alaphilippe.