
Thor Ringler (right) interviewed Ray Miller (left) in Miller’s hospital room at the William S. Middleton Memorial Veterans Hospital in Madison, Wis., in April. Miller’s daughter Barbara (center) brought in photos and a press clipping from Miller’s time in the National Guard to help facilitate the conversation.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Bob Hall was recovering from yet another surgery when the volunteer first walked into his hospital room. It was March 2014, and unfortunately Hall had been in and out of the hospital quite a bit. It had been a rocky recovery since his lung transplant, three months earlier, at the William S. Middleton Memorial Veterans Hospital in Madison, Wis.
But the volunteer wasn’t there to check on his lungs or breathing. Instead she asked Hall if we wanted to tell his life story.
Hall was being treated at the VA because he had served in the Marine Corps during the Vietnam War. After the war, he had a political career as a Massachusetts legislator, and then led professional associations for 30 years.
Hall, who was 67 at the time, welcomed the volunteer and told her he’d be happy to participate.
“I’m anything but a shy guy, and I’m always eager to share details about my life,” Hall says, half-jokingly.
He spoke to the volunteer for more than an hour about everything — from his time as “a D student” in high school (“I tell people I graduated in the top 95 percent of my class”) to his time in the military (“I thought the Marines were the toughest branch and I wanted to stop the communists”). He finished his story with a description of his health problems — those that that finally landed him in the hospital, and many that continue to the present day.
The interview was part of a program called My Life, My Story. Volunteer writers seek out vets like Hall in the hospital, and ask them about their lives. Then they write up this life story, a 1,000-word biography, and go over it with the patient, who can add more details or correct any mistakes.
“Of course, being a writer I rewrote the whole thing,” Hall confesses with a smile.
Once the story is finished, it’s entered into to the patient’s electronic medical record, so any doctor or nurse working anywhere in the VA system who opens the medical record can read it.
Hall was one of the earliest patients interviewed for the project, back in 2014. Today more than 2,000 patients at the Madison VA have shared their personal life stories.
Project organizers say My Life, My Story could change the way providers interact with patients at VA hospitals around the country.
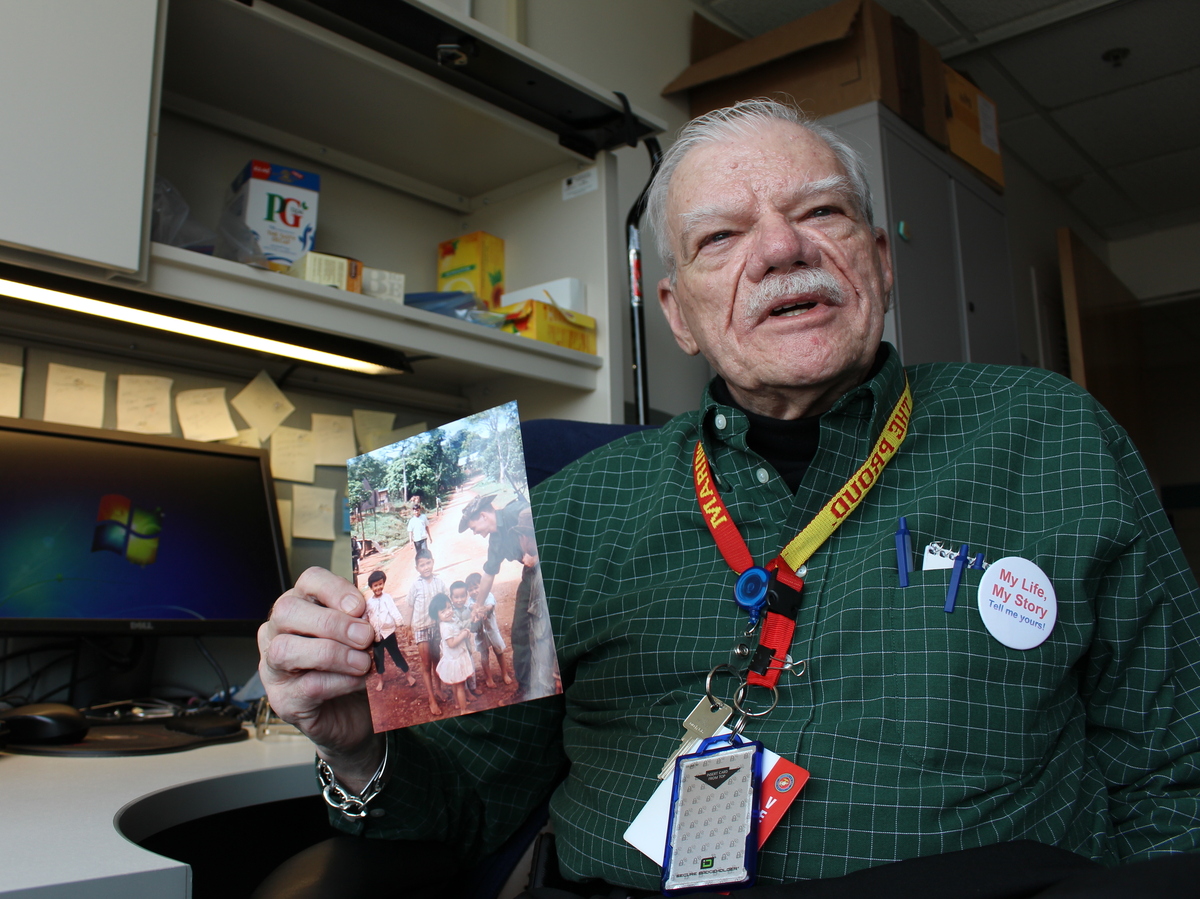
Bob Hall was one of the earliest patients to be interviewed for the My Life, My Story program at the VA hospital in Madison, Wisc. “I’d never experienced something like that in a hospital before,” Hall says.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
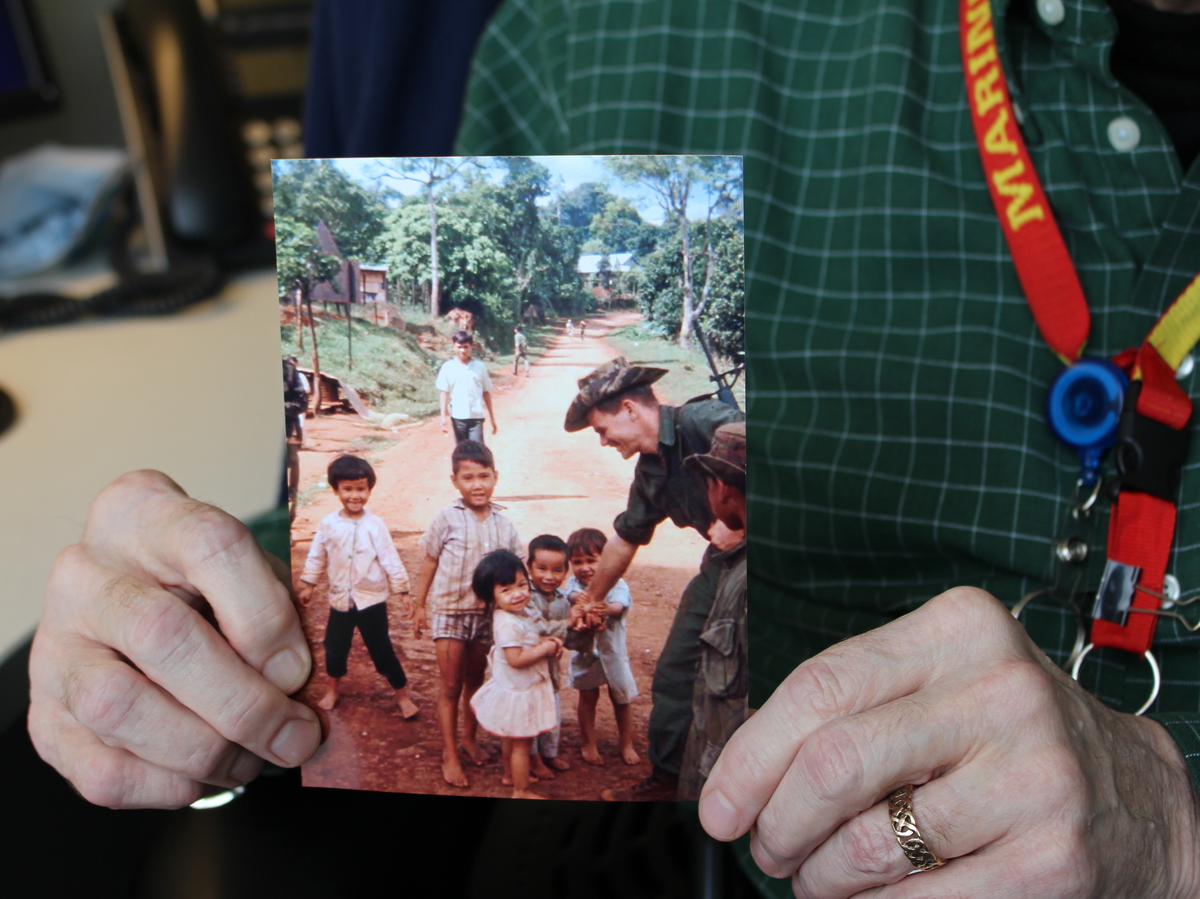
A close-up of Hall’s photograph of his conversation with children in a Vietnamese village. He served in the Marine Corps during the Vietnam War — an important part of his personal story.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Personalizing impersonal records
“If you’re a health care person, if you’re someone who is in the [electronic medical] record all the time, you’ll know that the record is a mess,” says Thor Ringler, who has managed the My Life, My Story project since 2013.
Clinicians can get access to a lot of medical data through a patient’s electronic medical record, but there’s nowhere to learn about a patient’s personality, or learn about her career, passions or values, Ringler says.
“If you were to try to get a sense of someone’s life from that record, it might take you days,” Ringler says.
The idea for My Life, My Story came from Dr. Elliot Lee, a medical resident who was doing a training rotation at the Madison VA in 2012. The typical rotation for medical residents lasts only about a year, so Lee wanted to find a way to bring these new, young doctors quickly up to speed on the VA patients. He wanted a way for them to absorb not just their health histories, but more personal information, like their hobbies, and which hospital staffers knew them best.
“It seemed to make sense that the patient might know a lot about themselves, and could help provide information to the new doctor,” Lee recalls.
But the question remained: What was the best way to get patients to share these details, to get their life stories into the records? Lee says he and some colleagues tried having patients fill out surveys, which were useful but still left the team wanting more. Next, they tried getting patients to write down their life stories themselves, but not many people really wanted to. Finally, an epiphany: Hire a writer to interview the patients, and put what they learned on paper.
It wasn’t hard to find a good candidate: A poet in Madison, Thor Ringler, had also just finished his training as a family therapist. He was good at talking to people, and also skilled at condensing big thoughts into concise, meaningful sentences.
“Of course!” Ringler remembers thinking. “I was made for that!'”
Thor Ringler has run the My Life, My Story program at the the William S. Middleton Memorial Veterans Hospital in Madison since 2013. In that time the program has recorded life stories of more than 2,000 veterans — and placed the short biographies in each vet’s’ electronic medical record.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Under Ringler’s guidance, the project has developed a set of training materials to allow other VA hospitals to launch their own storytelling programs. About 40 VA hospitals around the U.S. are currently interested, according to Ringler.
Based on his experience building the program in Madison, Ringler estimates hospitals would need to hire just one writer — working half- or full-time, depending on the hospital’s size — to manage a similar storytelling program. That means the budget could be as low as $23,000 a year. That relatively small investment can pay huge dividends in terms of patient satisfaction, Ringler says, by restoring personal connections between patients and the medical team.
“If we do good stories, people will read them, and they will want to read them,” he adds.
In addition to the interest from within the VA system, the idea has spread farther — to hospitals like Brigham and Women’s Hospital in Boston, and Regions Hospital in St. Paul, Minn.
A ‘gift’ to doctors and nurses
There is also research suggesting that when caregivers know their patients better, those patients have improved health outcomes.
One study, for example, found that doctors who scored higher on an empathy test had patients with better-controlled blood sugar. Another study found that in patients with a common cold, the cold’s duration was reduced by nearly a full day for those patients who gave their doctor a top rating for empathy.
University of Colorado professor Heather Coats studies the health impact of biographical storytelling. She notes a 2008 study found that radiologists did a more thorough job when they were simply provided a photo of the patients whose scans they were reading.
“They improved the accuracy of their radiology read,” Coats says. “Meaning [fewer] misspelled words; a better report that’s more detailed.” Current research is investigating whether storytelling might have a similar effect on clinical outcomes.
And, Coats adds, the benefits of the kind of storytelling happening at the VA don’t just accrue to the patients.
“I consider it a gift to the nurses and the doctors,” Coats says.
A survey of clinicians conducted by the Madison VA backs that up: It showed 85 percent of them thought reading the biographies of patients produced by Thor Ringler’s team of writers was “a good use” of clinical time and also helped them improve patient care.
“It gives you a much better understanding about the entirety of their life and how to help them make a decision,” says Dr. Jim Maloney, a VA surgeon who performed Bob Hall’s lung transplant in 2013.
That’s critical for doctors like Maloney, because only about half the people who undergo a lung transplant are still alive after five years. Maloney believes knowing more about a patient’s life story makes it easier for the doctor to have difficult but necessary conversations with a patient — to learn, for example, how aggressively to respond if a complication occurs.
Jim Maloney, a transplant surgeon at the Madison VA, says being able to read a patient’s personal story, along with their medical story, helps him help them through difficult decisions. “It gives you a much better sense of the entirety of their lives,” Maloney says.
Bram Sable-Smith for NPR
hide caption
toggle caption
Bram Sable-Smith for NPR
Maloney says the stories generated by My Life, My Story give the entire transplant team near immediate access to a valuable tool, one that helps them connect quickly with patients and family members, and start conversations about sensitive issues or difficult choices about end-of-life care.
Dr. Tamara Feingold-Link has also experienced the power of being able to read a patient’s life story. Now a second-year medical resident at Brigham and Women’s Hospital in Boston, Feingold-Link first encountered one of the biographies generated by My Life, My Story when she was on rotation at a Boston-area VA. Her attending physician asked her to run a meeting with a patient’s family.
“I barely knew the patient, who was so sick he could hardly talk,” Feingold-Link recalls.
She noticed his medical record included the patient’s life story, something she had never seen before. She immediately read the story.
“It brought me to tears,” she remembers. “When I met his family, I could connect with them immediately.”
“It made his transfer to hospice much smoother for everyone involved,” she says.
Now Dr. Feingold-Link has started a similar program at Brigham and Women’s Hospital.
Meaningful stories go beyond medical care
Bob Hall has learned the stories can be meaningful to caregivers even when they’re not working. During one of his stays at the Madison VA, a nursing aide came into his room after she read his life story in his medical record.
“She came in one night and sat down on my bed just to talk to me for a while, because she’d read my story,” Hall says. “I found out later she wasn’t on the clock. She just came in after her shift ended to chat for a while.”
It’s been 5 years since Hall’s lung transplant, and he’s doing well. He even found a part-time job putting his writing skills to work as part of the My Life, My Story team. In just two years, Hall has written 208 capsule biographies of veterans who come to this hospital for care, just like he did.
“Dr. Maloney came to me one day recently, and I was telling him how many stories I’d done,” Halls says, “and he says, ‘You know I think you’ve given more back to the VA with these stories than they gave to you.'”
“I said, ‘Doctor, I don’t think that’s true, but it’s very kind of you to say so.’ It made me feel good.”
This story is part of NPR’s reporting partnership with Kaiser Health News.
Let’s block ads! (Why?)












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}