Mosquito-Borne Diseases Found In U.S. Athletes And Staff At Rio Olympics

Health workers spray insecticide to combat Zika-carrying mosquitoes under the bleachers of the Sambódrome in Rio de Janeiro in January 2016.
Leo Correa/AP
hide caption
toggle caption
Leo Correa/AP
In the spring of 2016, there was a frenzy over the threat of Zika virus at Brazil’s Olympic Games. As infections reached their peak, a group of scientists called for the games to be moved somewhere else. A number of athletes, worried about sexually transmitting the virus to pregnant partners, chose to stay home.
But a group of researchers with University of Utah and the United States Olympic Committee announced Saturday that they weren’t able to find any evidence that U.S. Olympians, Paralympians or staff got Zika virus at all.
The group took blood samples from 457 athletes and staff before and after they traveled to the Olympics in Rio de Janeiro. They tested the blood for antibodies for Zika virus, along with other viruses carried by mosquitoes in the area: chikungunya, West Nile virus and dengue.Antibodies show that a person’s immune system has fought off a virus.
Out of those 457 people tested, 32 people came back with antibodies to mosquito-borne viruses they hadn’t had in their blood before: Three for chikungunya, two for dengue and 27 for West Nile virus.
“Because everyone was concentrating on Zika, we were all surprised that we detected other [mosquito-borne] viruses,” says Dr. Krow Ampofo, a specialist in pediatric infectious diseases with the University of Utah who worked on the study. He presented the findings at a conference Saturday.
But when it comes to which viruses the athletes and staffers actually got, the results can sometimes be hazy. The viruses are so closely related that antibodies for one can look a lot like antibodies for another, yielding false positives and sometimes false negatives.
But, says Dr. Benjamin Pinsky, a clinical pathologist at Stanford University Medical Center, the results are “pretty good evidence” that the athletes and staff weren’t exposed to Zika virus.
Usually, he says, the problem with the Zika virus antibody test is that it yields false positives, not false negatives. And it makes sense when you look at the chart of known Zika cases over time — by the time the Olympics started, the peak of the epidemic had passed.
For Pinsky, the takeaway was that despite all the precautions people took to protect themselves against Zika, people still got bitten by mosquitoes.
“Because of all the concern about Zika, most folks did use mosquito repellent. However, that was not good enough,” he says. “That was my take-home. There was still exposure. And had Zika been more prevalent, there would have likely been many more infections.”
Amir Attaran, a professor of public health and law at the University of Ottawa, is less convinced by the study’s results. He was one of the scientists who wrote a letter calling on the Olympics to be moved somewhere else.
“Their results are conclusive for the following proposition: During the Olympics, people got exposed to new infections,” he says. But because antibodies against the virus can be so similar, he says, “we’re unable to say which ones.”
But the fact that athletes and staff got viruses at all, he says, is something to think about.
After all, they were probably the most protected from mosquitoes of almost anyone at the Rio Games. They slept in air-conditioned rooms with screens on the windows, in areas that had been extensively sprayed with insecticides before the Olympics and Paralympics started. And they had been advised to wear long sleeves, to use repellent and to not spend time outside at dawn and dusk, when the mosquitoes that carry the viruses are most active.
“If you think about it, the athletes are likely the least affected. They and their support crew stayed in the Olympic village — and that’s as good as mosquito control got,” he says. “So, if you’re picking up in this study 32 cases of some mosquito-borne illness among the most coddled group during the Olympics, what does that tell you about the rest?”
At the very least, it shows that mosquitoes are cunning little beasts.
The Critical Needs Of Hospitals In Puerto Rico

Scott Simon talks to Edgar Crespo, an administrator at the Hospital de la Concepcion in San German, Puerto Rico, about receiving patients from other hospitals.
SCOTT SIMON, HOST:
Hospitals in Puerto Rico are grappling with dwindling supplies, power outages and the basic challenge of keeping their patients alive. The Hospital de la Concepcion in San German, southwestern Puerto Rico, has been taking in patients from other hospitals around the island. Edgar Crespo is an administrator of the hospital and joins us now.
Mr. Crespo, thanks so much for being with us.
EDGAR CRESPO: Oh, thank you for having me here in your program.
SIMON: How many patients have you had to take in, sir?
CRESPO: We have been receiving patients from other parts of the region. We have taken close to 150 to 160 patients in our emergency department. We had a record of admitted patients around 170 or 180.
SIMON: So are you over capacity?
CRESPO: Yes, we were. One to two days after Hurricane Maria hit us, we were over capacity.
SIMON: And your hospital is over 500 years old, right?
CRESPO: Yes, that’s correct. It was the first hospital in the island from the Spaniard time.
SIMON: And how are you doing?
CRESPO: We were really well-prepared. We had good emergency preparedness plans that we put in place. We produce our own electricity on site. And also it is more reliable since we don’t have electrical lines, transmission lines or all of that losses that you have in a regular system from the utility grid.
SIMON: And what do you hear from other hospitals? What are their challenges?
CRESPO: Right now, a lot of hospitals are having problems with diesel fuel for their generators. Most of the hospitals are running with backup generators. You know, backup generators are not designed to run extended period of time, and that’s what’s happening right now. You have near – I would that more than 80 percent of the hospitals are still running their emergency backup generators since they don’t have utility power yet.
SIMON: And what do you need in the future, in the next few days and weeks?
CRESPO: Right now, here in Puerto Rico, we have two companies that provide oxygen and medical gases. One of them are running out of – they are having problems. The other issue is to – that the medical supplies, like IV solutions and some medicines, like antibiotics – as the time goes on, we can run out about those types of supplies.
SIMON: So you’re concerned about oxygen, which people need to breathe, and concerned about antibiotics and other medications, I guess – basics.
CRESPO: Yes. Basics, yes.
SIMON: Well, you are important to a lot of people.
Thank you very much, Mr. Crespo.
CRESPO: Thank you very much, people. Please pray for us here.
SIMON: Yes, sir.
Edgar Crespo is an administrator of the Hospital de la Concepcion in southwestern Puerto Rico. Thanks so much, sir.
CRESPO: Thank you.
Copyright © 2017 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Idle Pharmaceutical Factories In Puerto Rico Raise Concerns Of Drug Shortages
NPR’s Robert Siegel talks with reporter Katie Thomas of The New York Times about how Hurricane Maria may cause shortages of essential drugs due to idled factories.
Trump Guts Requirement That Employer Health Plans Pay For Birth Control

Demonstrators in Washington, D.C., argued for upholding the Affordable Care Act’s birth control provision in 2015. The rollback of the rule is likely to spur further lawsuits, analysts say.
Charles Dharapak/AP
hide caption
toggle caption
Charles Dharapak/AP
Updated 4:52 pm
The Trump administration is rolling back the Obama-era requirement that employer-provided health insurance policies coverbirth control methods at no cost to women.
According to senior officials with the Department of Health and Human Services, the goal of the new rule is to allow any company or nonprofit group to exclude the coverage for contraception if it has a religious or moral objection.
“This provides an exemption, and it’s a limited one,” said Roger Severino, director of the HHS Office of Civil Rights. “We should have space for organizations to live out their religious identity and not face discrimination.”
He said he expects that most companies will continue to provide coverage for birth control and that the changes will only affect a tiny percentage of U.S. women. The new rules are being published Friday in the Federal Register and go into effect immediately.
But some health policy analysts say the new rule creates a huge opening that lets any employer claim an exemption, leaving their female workers to pay the full cost of any birth control out of pocket.
“It is a huge loophole for any employer that does not want to provide birth control coverage to their employees,” says Dania Palanker, a professor at Georgetown University’s Center on Health Insurance Reform.
The change fulfills a promise President Trump made in May to the Catholic religious order The Little Sisters of the Poor in a ceremony in the White House Rose Garden. The nuns had sued the Obama administration over the birth control requirement.
It also sets up a fight between advocates of religious freedom and those of equal rights for women. The American Civil Liberties Union sued the Trump Administration within hours of the rule being published, claiming it violated the 14th Amendment’s Equal Protection Clause, which ensures that all people receive equal protection under the law.
“The Trump Administration is forcing women to pay for their boss’s religious beliefs,” said ACLU senior staff attorney Brigitte Amiri, in a statement.
The Affordable Care Act, also known as Obamacare, requires employer-provided health insurance policies to include coverage for preventive health care. After the law passed, HHS used its regulatory authority to specify what has to be included in those preventive services and birth control, including “all Food and Drug Administration approved contraceptive methods, sterilization procedures, and patient education and counseling for all women with reproductive capacity.”
But the policy was controversial from the start.
Several companies and religious groups sued, saying the rule infringed on their religious freedom.
The Obama administration created an exemption for churches and allowed other “religious employers” to opt out by notifying the government. When they did so, the administration would arrange with their insurance companies to provide the coverage directly, without the employers’ involvement.
But the Little Sisters of the Poor weren’t happy with that workaround and sued.
The group’s case, and a second one involving private businesses including the Hobby Lobby chain of craft stores, which has 32,000 employees, went to the Supreme Court.
The court ruled in favor of Hobby Lobby in 2014, saying privately held companies could object on religious grounds. And then, last year, the court issued a split ruling in the Little Sisters case, saying the government shouldn’t fine the nuns but ordering the two sides to work out an arrangement that accommodates their religious beliefs.
Before a deal was reached, Trump became president.
At the Rose Garden ceremony in May, he told the Little Sisters of the Poor that he planned to change the rules. “Your long ordeal will soon be over,” he promised.
Under the new rule, women who work for Hobby Lobby or the religious group may no longer have access to birth control coverage through the Obama-era workaround. A Hobby Lobby spokesman said the company would have no comment on Friday, and the Little Sisters of the Poor didn’t respond to NPR’s emails seeking comment.
Hobby Lobby’s founder and CEO David Green told reporters in 2013, “Our family is now being forced to choose between following the laws of the land that we love or maintaining the religious beliefs that have made our business successful and have supported our family and thousands of our employees and their families.”
HHS officials said they don’t expect many companies to seek waivers. They said the group seeking waivers will likely be limited to those about 200 companies and nonprofits that have already sued.
But Palanker says the impact could be a lot bigger. There are a lot of large private companies, she says, whose owners may hold strong religious beliefs but did not want the publicity and expense of suing the federal government.
“A lot of women will retain birth control coverage,” Palanker says, “but there will be a lot of women who will lose that coverage.”
That means they’ll find themselves paying out of pocket. A one-month supply of birth control pills can cost anywhere from $4 to $55 or more, according to GoodRX.com.
Longer-acting contraception, like an intrauterine device, can cost more than $1,000, says Sarah Lipton-Lubet, a vice president at the National Partnership for Women and Families. She says the new rule is a tool for discrimination against women.
“Women shouldn’t be denied access to basic health care based on their employers’ religious beliefs,” she says. “We all have the right to our religious beliefs. But the way that this rule treats religion is really an excuse to discriminate.”
HHS officials say they also plan more stringent enforcement of a provision in the Affordable Care Act that prohibits federal subsidies from being used for insurance policies that cover abortion. The agency will issue guidelines for insurers Friday on how they have to charge women who want abortion coverage at least $12 a year more for such a policy, and they have to keep that money in a separate fund to be used only to pay for abortions.
In addition to the ACLU, Massachusetts Attorney General Maura Healey, and California Attorney General Javier Becerra announced they too plan to file suit opposing the new rule.
Neanderthal Genes Help Shape How Many Modern Humans Look

An employee of the Natural History Museum in London peeks at a model of a Neanderthal male in his 20s on display for a 2014 exhibition.
Will Oliver /PA Images via Getty Images
hide caption
toggle caption
Will Oliver /PA Images via Getty Images
Neanderthals died out some 30,000 years ago, but their genes live on within many of us.
DNA from our shorter, stockier cousins may be influencing skin tone, ease of tanning, hair color and sleeping patterns of those of present-day Europeans, according to a study from the Max Planck Institute for Evolutionary Anthropology published Thursday in the American Journal of Human Genetics.
Scientists estimate that more than a few Homo sapiensran into Neanderthals tens of thousands of years ago in Eurasia. They liked each other well enough to mate, and now Neanderthal DNA is thought to make up between 1 and 3 percent of the genetic code of most people who aren’t indigenous Africans.
African people have very little Neanderthal DNA because their ancestors didn’t make the trip through Eurasia, scientists think.
Computational biologist Michael Dannemann, the lead author on the latest paper looking at the Neanderthal DNA that persists in modern humans, says that he wondered, well, does it do anything?
He and his colleagues looked for associations between Neanderthal DNA and human appearance and behavioral traits. The researchers analyzed information from over 100,000 people in the UK Biobank, a database that contains genetic information and people’s answers to an extensive questionnaire, including questions about physical appearance and behavior.
Dannemann and co-author, Janet Kelso, also at the Max Planck Institute for Evolutionary Anthropology, found genetic material from Neanderthals associated with traits like skin tone, hair color and sleeping patterns.
Interestingly enough, many of the traits have something to do with sun exposure. Dannemann says it’s speculative still, but there may be some logic to it. The paper explains that Neanderthals lived in Eurasia for about 100,000 years before some modern humans arrived, giving them more time to get used to a wider range of daylight and lower UVB levels. According to the paper, skin, hair color, and circadian rhythm — all traits associated in the study with Neanderthal DNA — are linked to light exposure.
But, before making a leap and blaming your Neanderthal genes for your hair color, there’s more to the story.
Dannemann points out that you can look at someone’s genes and have a hard time telling if she’s tall or short — most human traits are determined by multiple genes working together. When it comes to skin tone, he says, several different parts of genetic material impact it, only some of which come from Neanderthals.
“It’s not any single gene that makes a huge difference … It’s not like morning people have one thing and evening people have another,” says anthropologist John Hawks, of the University of Wisconsin–Madison. “It’s many genes. Each of them has some small effect. This study is pointing out that, hey, there’s one of these [genes] that has a small effect coming from Neanderthals.”
Dannemann says they found multiple Neanderthal genes that affected hair and skin tone, some lighter and some darker. He says this suggests that Neanderthals themselves may have had variation in those traits too, meaning, maybe they too had a range of skin and hair tones.
Hawks say that this study reminds us that Neanderthals weren’t so different from us. “My take on this is that it’s showing the ways in which Neanderthal genetics, the genes we inherited from Neanderthals, are part of normal human variation,” he says. “They’re not super weird things that make people different. They’re part of these normal phenotypes.”
He also points out some limitations in the latest work: All the data are from the U.K. Dannemann also says that much of the previous research studied people of European ancestry.
He adds that there’s an increasing number of biobanks and databases like the one in the U.K. that include genetic information along with traits, “I think mining those and learning more about the contribution of Neanderthals to human traits is certainly something that’s still interesting.”
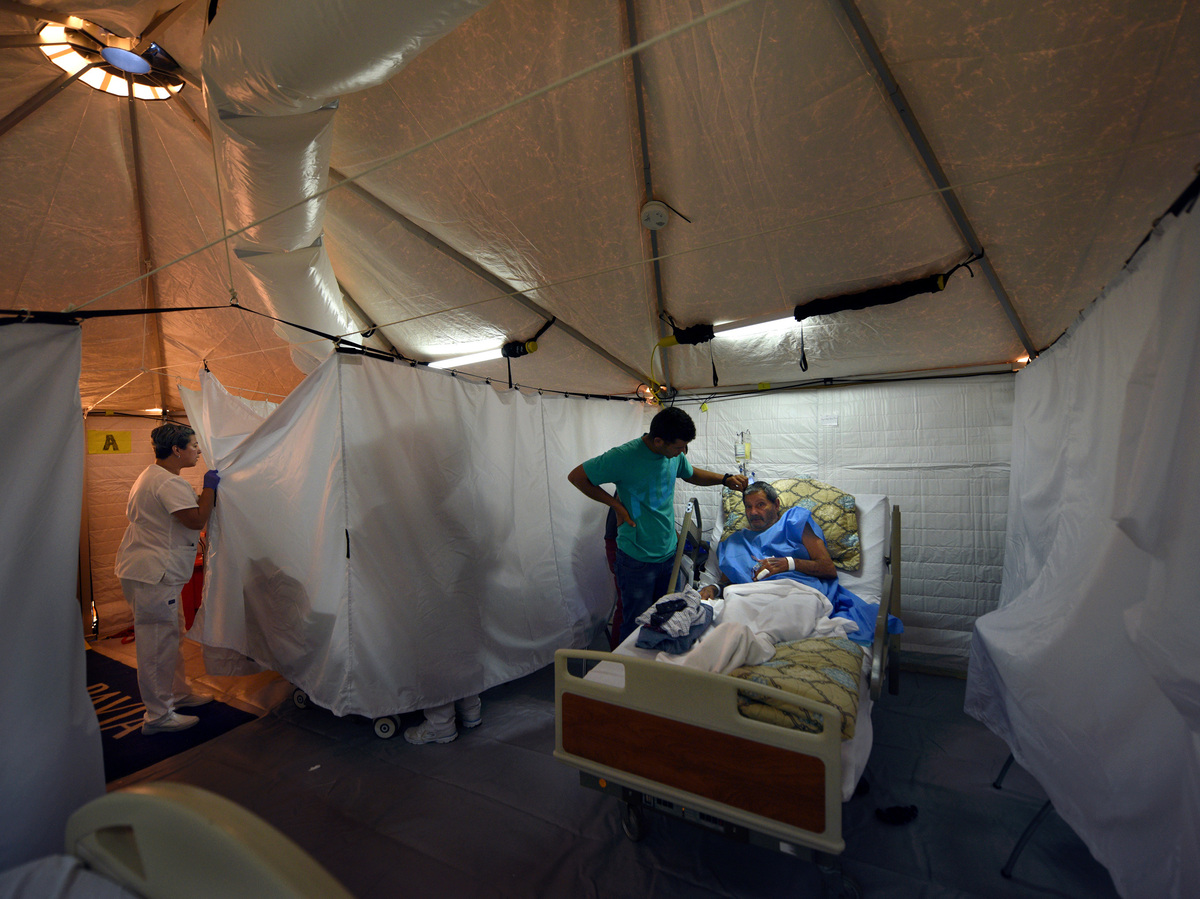
112 Degrees With No Water: Puerto Rican Hospitals Battle Life And Death Daily

The hospital in Arecibo, Puerto Rico, evacuated its coronary floor this week and moved those patients into cooled tents erected by an American disaster medical team.
Carol Guzy for NPR
hide caption
toggle caption
Carol Guzy for NPR
Every day across Puerto Rico, with its shattered power grid, hospitals are waging a life-and-death battle to keep their patients from getting sicker in the tropical heat. Now two weeks after the storm, about three-quarters of Puerto Rico’s hospitals remain on emergency power. This creates dangerous conditions for critically ill patients.

Credit: Alyson Hurt/NPR
At the Pavia Arecibo Hospital, about an hour west of San Juan, administrator Jose Luis Rodriguez wipes sweat from his worried brow. “We don’t have any air conditioning,” he says. “We can handle maybe a week, but it’s already been two weeks almost.”
The government calls them “indirect deaths” – those who died after the violent storm: heart attack victims, people on kidney dialysis machines that failed, people who fell off roofs inspecting storm damage, and people killed in auto accidents on highways made more treacherous from Maria’s destruction.
“So far after the storm we have had 49 dead bodies,” says Rodriguez. Earlier this week, the governor of Puerto Rico raised the official fatality figure for Hurricane Maria from 16 people to 34. But with unofficial reports like the one from Arecibo, that number is expected to rise.

The U.S. Disaster Medical Assistance Team (DMAT) inspects a damaged hospital in Aguadillo, Puerto Rico, with a federal agent providing force protection.
Carol Guzy/for NPR
hide caption
toggle caption
Carol Guzy/for NPR

Hospitals in Puerto Rico are dealing with no power, no air conditioning, no local water, no local food, no Internet and very limited communication.
Carol Guzy for NPR
hide caption
toggle caption
Carol Guzy for NPR
The fourth floor of the Arecibo hospital has now been taken over by stocky mid-westerners in khaki pants, black boots and T-shirts emblazoned with DMAT, for Disaster Medical Assistance Team. It’s a kind of National Guard for reservist medical workers that falls under the Department of Health and Human Services.
Chief medical officer of this DMAT currently deployed to Arecibo is Dr. Melissa Stein. She’s normally an urgent care physician at Mercy Hospital in St Louis. “In telling team members coming here we tell them it’s going to be an extremely austere environment,” she says.
No power, no air conditioning, no local water, no local food, no Internet and very limited communication. Hurricane Maria falls somewhere between Hurricane Harvey in Houston — where teams stayed in a hotel — and the 2010 Haiti earthquake, where they created a field hospital in Port-au-Prince and slept outside.
Each deployment has its challenges. In the Arecibo hospital, it was the sweltering sixth-floor cardiac unit.

The U.S. Disaster Medical Assistance Team (DMAT) inspects a damaged hospital in Aguadillo, Puerto Rico, with a federal agent providing force protection.
Carol Guzy for NPR
hide caption
toggle caption
Carol Guzy for NPR
The temperatures up there were as high as 108 degrees and even higher. “This was a huge stress on the patients who were quite sick. So we have ended up moving them to these tents where the hospital staff is caring for them,” says Dr. Jim Fehr, who is on the DMAT team.
Lying in the cooling tent is a 77-year-old retired factory worker named Georgina Gonzales. Had she not been brought here she might have ended up as an indirect victim of the storm.
“Very hot, very hot! I was suffocating,” she says. “When they transferred me here on Sunday, they rescued me from the dragon’s mouth.”
Back on the fourth floor, a distraught woman appears with a shocking story: the hospital an hour away in the city of Aguadilla, she says, has shut down, kicked out the patients, and it smells like decomposing bodies.
Team commander George Thorp springs into action. “We’ll get a strike team there right away,” he says. Within an hour, the strike team is racing down the highway, past utility poles snapped like pencils and the fallen arches of a McDonald’s.
The team roars up to the Good Samaritan Hospital of Aguadilla. Two heavily armed federal agents enter first, then comes the DMAT expecting the worst.
They walk down a corridor past bewildered nurses and are ushered into a quiet, orderly office. There is nervous laughter.

U.S. Disaster Medical Assistance Teams erected two cooled emergency rooms for critically ill patients at the hospital in Arecibo, Puerto Rico, where temperatures on the 6th floor soared to 112 degrees one day. Sarilin Lopez, grateful to be in the field hospital, says, “It was so hot I could hardly breathe.”
Carol Guzy for NPR
hide caption
toggle caption
Carol Guzy for NPR
“I’m chief medical officer for a national disaster medical assistance team,” Dr. Stein tells the hospital director. “We had been told that you needed significant help. I can tell when we pulled up the story was somewhat exaggerated.”
The Aguadilla hospital administrator, Marilyn Morales, listens politely.
“Our emergency room is in bad condition in terms of the temperature,” Morales says. “If you can install something next to the ER that would be excellent, with physicians, medications and supplies.”
As it turns out, both the Arecibo and Aguadilla hospitals are in the same boat —there’s no air-conditioning, the emergency generators need maintenance, and the patients and staff are hot.
After a tour, Stein promises to request some federal help, and the team files back out onto the sidewalk.

Dr. Arturo Cedeno, medical director of Good Samaritan Hospital in Aguadilla, Puerto Rico, tells an American disaster medical team his hospital needs a new generator to run the air conditioning to keep it functioning.
Carol Guzy for NPR
hide caption
toggle caption
Carol Guzy for NPR
“All right, saddle back up, get your packs,” she says, adding with a smile, “This is not the hospital of the walking dead which is what had been described.”
The experience is a good example of what happens after a traumatic weather event, when there’s no communication — rumors fly, and people worry about their hospitals.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
About three-quarters of hospitals in Puerto Rico are operating on limited emergency power—which means no air conditioning. No one knows when the electric grid will be rebuilt and they can be resume normal service
Carol Guzy/for NPR
hide caption
toggle caption
Carol Guzy/for NPR
California Bill Would Compel Drugmakers To Justify Price Hikes

{kind=link}
Drug lobbyists and consumer health advocates fill the halls of the state Capitol in September to see how Assembly members vote on a controversial drug price transparency bill.
Tam Ma/Courtesy of Health Access California
hide caption
toggle caption
Tam Ma/Courtesy of Health Access California
Insurers, hospitals and health advocates are waiting for Gov. Jerry Brown to deal the drug lobby a rare defeat, by signing legislation that would force pharmaceutical companies to justify big price hikes on drugs in California.
“If it gets signed by this governor, it’s going to send shock waves throughout the country,” said state Sen. Ed Hernandez, a Democrat from West Covina, the bill’s author and an optometrist. “A lot of other states have the same concerns we have, and you’re going to see other states try to emulate what we did.”
The bill would require drug companies to give California 60 days’ notice anytime they plan to raise the price of a drug by 16 percent or more over two years. They would also have to explain why the increases are necessary. In addition, health insurers would have to report what percentage of premium increases are caused by drug spending.
Drugmakers have spent $16.8 million on lobbying since January 2015 to kill an array of drug legislation in California, according to data from the Secretary of State’s Office. The industry has hired 45 lobbyists or firms to fight the price transparency bill alone. Against the backdrop of this opposition campaign, Brown must decide by Oct. 15 whether to sign or veto the bill.
This is the second go-round for this drug price bill. Last summer, the same legislation crashed and burned. Its intended regulations were gutted so extensively that Hernandez decided to pull it. But, he said, two key things happened after that, stetting the stage for a successful second attempt.
First, in August 2016, less than a week after Hernandez pulled the bill, a firestorm of controversy erupted nationally over the price of EpiPens spiking nearly 500 percent. The increase sparked outrage from parents who carry the auto-injectors to save their children from life-threatening allergic reactions.
Momentum grew among federal lawmakers last September to do something. They called for hearings. Several proposed bills aimed to reign in drug prices across the country.
But then, the election of November 2016 disrupted all order of health care business in Washington. After Donald Trump was elected and Republicans took control of Congress, the number one health policy priority became repealing and replacing the Affordable Care Act.
As federal lawmakers focused on dismantling the ACA, Hernandez said he saw another opportunity for state lawmakers to act on drug prices. He reintroduced his bill in early 2017, and this time political support grew quickly, beyond the usual suspects.
“It wasn’t just labor,” he recalls. “It was consumer groups, it was health plans. It was the Chambers of Commerce, it was the hospital association.”
Hernandez is optimistic the governor will sign SB 17 into law. But he knows nothing’s certain. That’s because of what happened on Sept. 11, the day the bill came up for a key vote in the state Assembly — the same place it went down the year before. Hernandez thought he’d secured all the votes he needed, but at the last minute the votes started slipping away.
The bill needed 41 votes to pass the Assembly. During the roll call, the tally stalled around 35. Hernandez said he had plenty of colleagues willing to cast the 42nd vote, but with drug lobbyists swarming the Capitol, no legislators wanted to be the one to cast the deciding vote.
“If the bill fails and you’re stuck out there, then you’re the person that’s attacking the industry,” Hernandez says.
But, the bill crossed the 41-vote threshold and the remaining lawmakers joined in. In the end, the bill passed with 66 votes. All the Democrats and half the Republicans in the state Assembly voted for it.
This was much to the dismay of drug companies, which lobbied hard and issued a blitz of advertising in the last weeks before the vote.
The Pharmaceutical Research and Manufacturers of America, or PhRMA, a drug industry’s trade group, argued that SB 17 was full of “false promises” that wouldn’t help consumers pay for their medicines, and would instead stifle innovation with cumbersome regulatory compliance.
“That takes up a lot of resources and will take up a lot of time,” says Priscilla VanderVeer, deputy vice president of public affairs for PhRMA. “And that could mean pulling resources from research and development and having to put it into the reporting structure.”
Experts say the drug industry doesn’t want a large influential state like California forcing them to share their data.
“When they have to justify in California, de facto, they have to justify it to the other 49 states,” says Gerard Anderson, a health policy professor at Johns Hopkins Bloomberg School of Public Health in Baltimore. “Other states essentially get to piggyback on the good efforts of California, and hopefully, because they might have difficulty justifying the price increases, everybody’s prices around the country will be lower.”
Other states, including Maryland, Vermont, Nevada and New York, have passed similar laws aimed at bringing more transparency to prices and curbing price gouging. But the pharmaceutical industry has fought the hardest in California. If drug companies don’t like the disclosure laws in smaller states, they could decide not to sell their drugs there, Anderson says, but the market in California is just too big to ignore.
“States like Maryland are just not as powerful,” he says. “It just doesn’t have the clout that a state like California has.”
But drugmakers are likely already devising ways to work around the California bill, Anderson warns. They’ve filed lawsuits to try to slow or stop laws from being implemented in other states, or to weaken the rules if and when they go into effect. Policy experts are watching to see what kinds of legal challenges the California law might be vulnerable to, and if it can withstand them.
“We learn from the mistakes of other states,” Anderson says. “Legislation is an iterative process. We have 50 states and hopefully, by some time, we’ll get it right. We’re looking for California to take the lead on this.”
This story is part of a reporting partnership with NPR, KQED and Kaiser Health News.
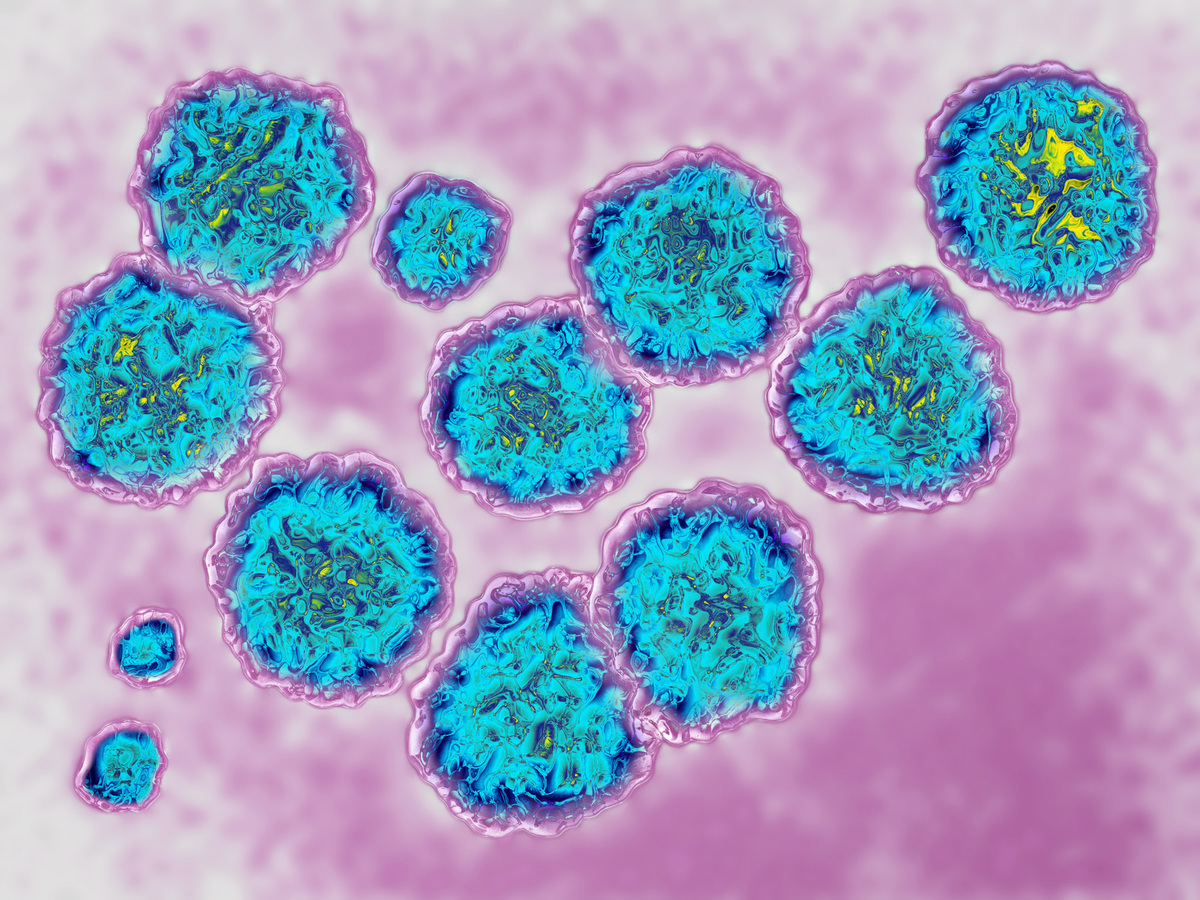
FDA's Approval Of A Cheaper Drug For Hepatitis C Will Likely Expand Treatment

{kind=link}
Hepatitis C virus, via transmission electron microscopy. (The actual viral diameter is around 22 nm.) Doctors say the recent FDA approval of Mavyret, a less expensive drug for treating the virus, may make it easier for more insurers and correctional facilities to expand treatment.
James Cavallini/Science Source
hide caption
toggle caption
Valerie Green is still waiting to be cured.
The Delaware resident was diagnosed with hepatitis C more than two years ago, but she doesn’t qualify yet for the Medicaid program’s criteria for treatment with a new class of highly effective but pricey drugs.
The recent approval of a less expensive drug that generally cures hepatitis C in just eight weeks may make it easier for more insurers and correctional facilities to expand treatment.
The drug, Mavyret, is the first to be approved by the Food and Drug Administration that can cure all six genetic types of hepatitis C in about two months in patients who haven’t previously been treated. Other approved drugs generally require 12 weeks to treat the disease and often aren’t effective for all types of hepatitis C.
In addition, Mavyret’s price tag of $26,400 for a course of treatment is significantly below that of other hepatitis C drugs whose sticker price ranges from about $55,000 to $95,000 to beat the disease. Patients and insurers often pay less, however, through negotiated insurance discounts and rebates.
“It certainly stands to reason that the continual march downward on cost would lead to continual opening up of criteria,” says Matt Salo, executive director of the National Association of Medicaid Directors.
Hepatitis C is a viral liver infection spread through blood that affects an estimated 3.5 million people in the United States. It can take years to cause problems. Many baby boomers who contracted it decades ago before blood was screened for the virus don’t realize they have it until they develop liver disease. In addition, the growing heroin epidemic is adding to the problem as people become infected by sharing contaminated needles.
“Direct-acting antiviral” therapies like Harvoni, a once-a-day pill introduced in 2014 that generally cured hepatitis C in 12 weeks, are much more effective than earlier treatments that required weekly interferon injections and multiple daily pills for nearly a year. But the newer regimens came at a price: $94,500, in Harvoni’s case.
State Medicaid programs, which cover a high proportion of people with hepatitis C, balked at the high prices, even with the 23 percent drug discount the programs typically receive. Many threw up roadblocks to limit drug approval until the disease was advanced. Some required people to be drug- and alcohol-free for six months or more before treatment would be approved.
Those moves prompted advocates to push for better access, in some cases filing suit to force the programs to cover more people.
Faced with a lawsuit in Delaware, the state Medicaid program began loosening up treatment criteria this year, and in January will begin approving enrollees regardless of the severity of their disease.
The state joins more than a dozen others that no longer (or never did) restrict hepatitis C treatment based on disease severity, says Kevin Costello, director of litigation at Harvard Law School’s Center for Health Law and Policy Innovation, which has been a key player in litigation in Delaware and other states.
It can’t happen soon enough, says Green. She is 58 and believes she contracted the disease 31 years ago when she suffered complications during childbirth and required a blood transfusion. Although her liver isn’t damaged, Green says, she has suffered with abdominal and joint pain, weight loss and fatigue for decades – all symptoms her doctors attribute to the hepatitis C virus.
“It’s been a difficult fight for us Medicaid patients,” she says.
People who are incarcerated face an even tougher battle to get treatment for hepatitis C. A recent study of state prisoners suggested that roughly 17 percent of prisoners are infected with hepatitis C, compared with about 1 percent of the general population.
Prisons have a duty not to be deliberately indifferent to the medical needs of incarcerated people. Prisons don’t get the price discounts that the Medicaid programs have, and their budgets are fixed.
“Administrators have to make do with what is there,” says Dr. Anne Spaulding, an epidemiologist and associate professor at Emory University’s public health school, who has worked as a medical director in corrections and published research on hepatitis C among prisoners.
Lawyers in a handful of states are pursuing class action lawsuits to force prisons to provide hepatitis C treatment. Mavyret may make a difference, says David Rudovsky, a civil rights lawyer who’s litigating a class action lawsuit against the Pennsylvania Department of Corrections.
“Everyone recognizes that it’s going to make it easier to cover people,” he says.
Coverage for drugs that treat hepatitis C is typically less problematic for people who have private insurance (though some obstacles remain). For example, Mavyret is one of seven hepatitis C drugs that are included in the 2018 national preferred formulary by Express Scripts, which manages the pharmacy benefits for 83 million people.
“The benefit to patients and payers is the additional competition, which brings down costs across the class, thus resulting in greater access and affordability,” says Jennifer Luddy, director of corporate communications at Express Scripts.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Follow Michelle Andrews on Twitter: @mandrews110.
For Many Women, The Nearest Abortion Provider Is Hundreds Of Miles Away

{kind=link}
For women in rural areas, the nearest abortion provider can be a day’s drive away.
Carlos Ciudad Photos/Getty Images
hide caption
toggle caption
Carlos Ciudad Photos/Getty Images
There’s a clinic that’s right in Kelsey’s town of Sioux Falls, S.D., that performs abortions, but she still drove hours away to get one.
Back in 2015, she was going through a difficult time — recently laid off, had to move suddenly, helping a close family member through some personal struggles — when she found out she was also pregnant.
“I kind of knew right away that this was just not the time or place to have a child. I mentally wasn’t ready, financially wasn’t ready,” she says. “The whole situation really wasn’t very good.”
When Kelsey decided to end her pregnancy, she found herself navigating a maze of legal restrictions, in a part of the country where providers are few and far between. NPR is not using her last name to protect her privacy.
South Dakota has a 72-hour waiting period for abortions and requires women to meet with their doctor in advance of the procedure. Kelsey, a nurse, had recently started a new job and couldn’t take the time off to go to two appointments at the clinic in her city.
She was just a few weeks along, and it was important to her to end the pregnancy early.
“I just knew that I didn’t want to wait on this too long,” she said. “Everybody has their own feelings about what is appropriate for them to have an abortion … how far they want to wait and things like that. I just knew I just wanted to do it.”
She called several providers throughout the region, some hundreds of miles away, before she finally found an appointment in Minneapolis, about a four-hour drive away, on a day she happened to have off work.
Kelsey’s story is similar that of many women across the country, according to a report released Tuesday by the Guttmacher Institute, a reproductive health research organization that supports abortion rights.
The report, published in The Lancet Public Health, includes an analysis by Guttmacher researchers of the distances women must travel to obtain abortions in the United States. For 1 in 5 women, the report finds, the trip is more than 40 miles one way.
Loading…
The trip is often longest for women in rural areas, with some in South Dakota driving more than 330 miles, according to Jonathan Bearak, a senior research scientist with Guttmacher and lead author of the report.
“I think there’s an unfortunate extent to which access to abortion is a bit contingent on your ZIP code, and that doesn’t need to be the case but it is,” he says.
Bearak says that increasing the use of options like telemedicine to provide medication abortion and reducing legal barriers to the procedure, like cumbersome health regulations on clinics and providers, could help improve access.
Social pressure is another factor that deters some doctors, midwives and nurse practitioners from providing those services, Bearak says.
“I think right now the issue is that it’s hard to do that because there are so many barriers in place to providing that care — not just the patients, but the doctors are affected by stigma,” Bearak says.
In South Dakota, where patients like Kelsey struggle with limited access to abortion services, Planned Parenthood has had to find creative ways to staff its local clinic. There’s no full-time abortion provider there, so Planned Parenthood flies a doctor from Minneapolis to Sioux Falls and back twice each week — first to consult with patients, as required by law, and then to perform the abortions.
Dr. Carol Ball has been making that trip for about a decade. She said local doctors are unwilling or unable to provide abortion services.
“I’ve been told by a supportive physician here that basically providing abortions for a South Dakota physician in Sioux Falls would be — quote unquote — ‘career suicide,’ ” Ball says. “Because I believe that the feeling is that there would be consequences to their practice.”
Ball says many of her patients travel hundreds of miles, some from out of state, to obtain an abortion at the clinic in Sioux Falls.
“It means that they have to find time away from their jobs and find child care for their children and all of the other sort of logistical things that it takes for us to stop and go to a doctor’s appointment,” Ball says. “They have to do that twice.”
Planned Parenthood’s Upper Midwest region has been flying abortion providers in and out of Sioux Falls for more than 25 years. Communications director Jen Aulwes says women there have limited options for abortion services.
“They’re very few and far between. They’re very spread out.” Aulwes says. “There’s, over the years, fewer and fewer clinics that that are providing abortion.”
Lapse In Federal Funding Imperils Children's Health Coverage

{kind=link}
Senate Finance Committee Chairman Orrin Hatch, R-Utah, center, and ranking member Ron Wyden, D-Ore., have a plan to renew funding for the Children’s Health Insurance Program, which lapsed Sept. 30.
Jacquelyn Martin/AP
hide caption
toggle caption
Jacquelyn Martin/AP
Congress finally seems ready to take action on the Children’s Health Insurance Program after funding lapsed Sept. 30.
Before the deadline, lawmakers were busy grappling with the failed repeal of the Affordable Care Act.
CHIP covers 9 million children nationwide. But until Congress renews CHIP, states are cut off from additional federal funding that helps lower- and middle-income families.
CHIP, which has enjoyed broad bipartisan support, helps lower- and middle-income families that otherwise earn too much to be eligible for Medicaid. Besides children, it covers 370,000 pregnant women a year. Like Medicaid, CHIP is traditionally paid for by state and federal funding, but the federal government covers most of the cost.
The House Energy and Commerce Committee posted its bill just before midnight Monday. It mirrors the Senate Finance plan by extending funding for CHIP for five years and gradually phasing down the 23 percentage point funding increase provided under Affordable Care Act over the next two years.
Though current authorization for spending has expired, states can use some of their unspent federal funding to continue their programs. Several states are expected to run out of money before the end of 2017, and most of the rest will run out by next summer. CHIP has been in this fix only one other time since it was established in 1997. In 2007, CHIP went weeks without funding authorization from Congress.
Here’s a quick look at what may lie ahead for the program.
Will children lose coverage because Congress missed the deadline?
They could eventually, but not immediately. A few states facing the most pressing threat — including California and Arizona — have enough funding to last only until the end of the year.
No states have yet announced plans to freeze enrollment or alert families about any potential end in coverage. But if Congress fails to renew funding quickly, some states may begin taking steps to unwind the program in the next few weeks.
What are states doing in response to Congress missing the deadline?
Most states are doing little except reaching into their unspent federal funds.
Minnesota, however, was among the most imperiled because it had spent all its CHIP money. State officials said Tuesday that the federal Centers for Medicare & Medicaid Services was giving Minnesota $3.6 million from unspent national funds to cover CHIP this month.
Emily Piper, commissioner of the Minnesota Department of Human Services, reported in a newspaper commentary Sept. 18 that her state’s CHIP money funds would be exhausted last Sunday.
Even without the last-minute cash infusion, most of the children covered by CHIP would have continued to receive care under the state’s Medicaid program. But Minnesota would receive less fewer federal dollars for each child, according to Piper’s commentary. However, she added, those most at risk are the 1,700 pregnant women covered by CHIP, because they wouldn’t be eligible for Medicaid.
Utah has notified CMS has notified the Centers for Medicare & Medicaid Services that it plans to discontinue its CHIP program by the end of the year unless it receives more federal money. About 19,000 children are in the state’s CHIP program, state officials say. So far, though, the state says it is not moving to suspend service or enrollment or alert enrollees about any possible changes.
Nevada officials say if funding isn’t extended it might have to freeze enrollment on Nov. 1 and end coverage by Nov. 30.
California, which has 1.3 million children covered by CHIP, has the highest enrollment of any state running out of funding this year. But, so far, it’s continuing business as usual.
“We estimate that we have available CHIP funding at least through December 2017,” says Tony Cava, spokesman for California Department of Health Services. “Our CHIP program is open for enrollment and continues to operate normally.”
Oregon says it has enough CHIP funding to last through October for its program that covers 98,000 children.
When is Congress likely to act?
The Senate Finance and the House Energy and Commerce committees have scheduled votes Wednesday on legislation to extend CHIP funding. If both approve their individual bills, floor votes could come quickly, and then both houses would need to resolve any differences.
Senate Finance Committee Chairman Orrin Hatch, R-Utah, and the committee’s ranking Democrat, Sen. Ron Wyden of Oregon, announced an agreement in mid-September to renew CHIP funding. Under the proposed deal, federal CHIP funding would drop by 23 percentage points starting in by 2020, returning to its pre-Affordable Care Act levels. The agreement would extend the life of the CHIP program through 2022.
Hatch and Wyden didn’t provide any details on how they would pay for the CHIP extension.
The House Energy and Commerce Committee posted its bill just before midnight Monday. It mirrors the Senate Finance plan by extending funding for CHIP for five years and gradually phasing down the 23 percentage point funding increase provided under Affordable Care Act over the next two years.
If CHIP is so popular among Republicans and Democrats, why hasn’t Congress renewed the program yet?
The funding renewal was not a priority among Republican leaders, who have spent most of this year trying to replace the Affordable Care Act and dramatically overhaul the Medicaid program. Some in Congress also thought the Sept. 30 deadline was squishy since states could extend their existing funds beyond that.
Who benefits from CHIP?
While CHIP income eligibility levels vary by state, about 90 percent of children covered are in families earning 200 percent of poverty or less ($40,840 for a family of three).CHIP covers children up to age 19. States have the option to cover pregnant women, and 19 do so.
The program goes by different names depending on the state, such as Hoosier Healthwise in Indiana and PeachCare for Kids in Georgia.
For families that move out of Medicaid as their incomes rise, CHIP is an affordable option that ensures continued coverage for their children. Many states operate their CHIP programs as part of Medicaid.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Phil Galewitz is a senior correspondent for KHN.