Big Tobacco Spends Big To Block A Tax And Medicaid Expansion In Montana

Amanda Cahill, a supporter of Montana’s tobacco tax measure, I-185, at a press conference near the state capitol last August. Tobacco firms have spent $17 million in opposition to the initiative, compared to an $8 million campaign by those in favor of it.
Corin Cates-Carney/Montana Public Radio
hide caption
toggle caption
Corin Cates-Carney/Montana Public Radio
Montana legislators expanded Medicaid by a very close vote in 2015. The measure passed with the condition that the expansion of Medicaid eligibility in the state would expire in 2019 unless lawmakers voted to reapprove it. And once it expired, people who got Medicaid under the expansion would lose it.
Fearing legislators might not renew funding for Medicaid’s expanded rolls, Montana’s hospitals and other health advocacy groups have come up with a ballot measure to keep it going — and to pay for it with a tobacco tax.
Amanda Cahill works for the American Heart Association and is spokesperson for Healthy Montana, the coalition backing the measure, which will be on Tuesday’s ballot. She says coalition members knew big tobacco would fight back.
“We poked the bear, that’s for sure,” Cahill says. “And it’s not because we were all around the table saying, ‘Hey, we want to have a huge fight and go through trauma the next several months.’ It’s because it’s the right thing to do.”
If ballot initiative I-185 passes, it will mean an additional $2 per pack tax on cigarettes, and a tax on other tobacco products. It would also levee a tax on e-cigarettes, which are currently not taxed in Montana.
The tobacco tax initiative has become the most expensive ballot measure race in Montana history — drawing more than $17 million in opposition funding from tobacco companies alone — in a state with fewer than 200,000 smokers. Most of that money has come from cigarette maker Altria. According to records from the National Center for Money in Politics, that’s more money than Altria has spent on any state proposition nationwide since the center started keeping track in 2004.
Meanwhile, backers of I-185 have spent close to $8 million on the initiative, with most of the money coming from the Montana Hospital Association.
“What we want to do is — No. 1 — stop Big Tobacco’s hold on Montana,” Cahill says. Also, she continues, it’s imperative that the nearly 100,000 people in Montana who have Medicaid under the expansion will be able to keep their health care.
Cahill says I-185 will allocate plenty of money to cover the expansion, though some lawmakers say the state can’t afford it.

{kind=link}
{kind=link}
Kristin Page-Nei, government relations director of the American Cancer Society in Montana, was one of the authors of measure I-185, which would raise state taxes on cigarettes and other tobacco products.
Corin Cates-Carney/Montana Public Radio
hide caption
toggle caption
Corin Cates-Carney/Montana Public Radio
Nancy Ballance, a Republican representative in the Montana state legislature opposes the measure.
“In general I am not in favor of what we like to refer to as ‘sin taxes,’ ” Ballance says. “Those are taxes that someone determines should be [levied] so that you change people’s behavior.”
Ballance also isn’t in favor of ballot initiatives that, she says, try to go around what she sees as core functions of the legislature: deciding how much revenue the state needs, for example, or where it should come from, or how it should be spent.
“An initiative like this for a very large policy with a very large price tag — the legislature is responsible for studying that,” Ballance says. “And they do so over a long period of time, to understand what all the consequences are — intended and otherwise.”
Most citizens, she says, don’t have the time or expertise to develop that sort of in-depth understanding of a complicated issue.
Montana’s initiative to keep Medicaid’s expansion going would be a “double whammy” for tobacco companies, says Ben Miller, the chief strategy officer for the nonprofit Wellbeing Trust.
“People who are covered are more likely to not smoke than people who are uninsured,” says Miller, who has studied tobacco tax policies for years. He notes research showing that people with lower incomes are more likely than those with higher incomes to smoke; and if they’re uninsured, they’re less likely to quit.
Federal law requires Medicaid to offer beneficiaries access to medical help to quit smoking.
Plus, Miller adds, every time cigarette taxes go up — thereby increasing the price per pack — that typically leads to a decrease in the number of people smoking.
And that, he says, works against a tobacco company’s business model, “which is, ‘you need to smoke so we can make money.’ “
Ballance agrees that tobacco companies likely see ballot initiatives like I-185 as threats to their core business. But, she says, “for anybody who wants to continue smoking, or is significantly addicted, the cost is not going to prohibit them from smoking.”
The U.S. Centers for Disease Control and Prevention says tobacco use is the leading cause of preventable disease and death in the U.S.
Montana’s health department says that each year more than 1,600 people in the state die from tobacco-related illnesses.
This story is part of NPR’s reporting partnership with Montana Public Radio and Kaiser Health News.
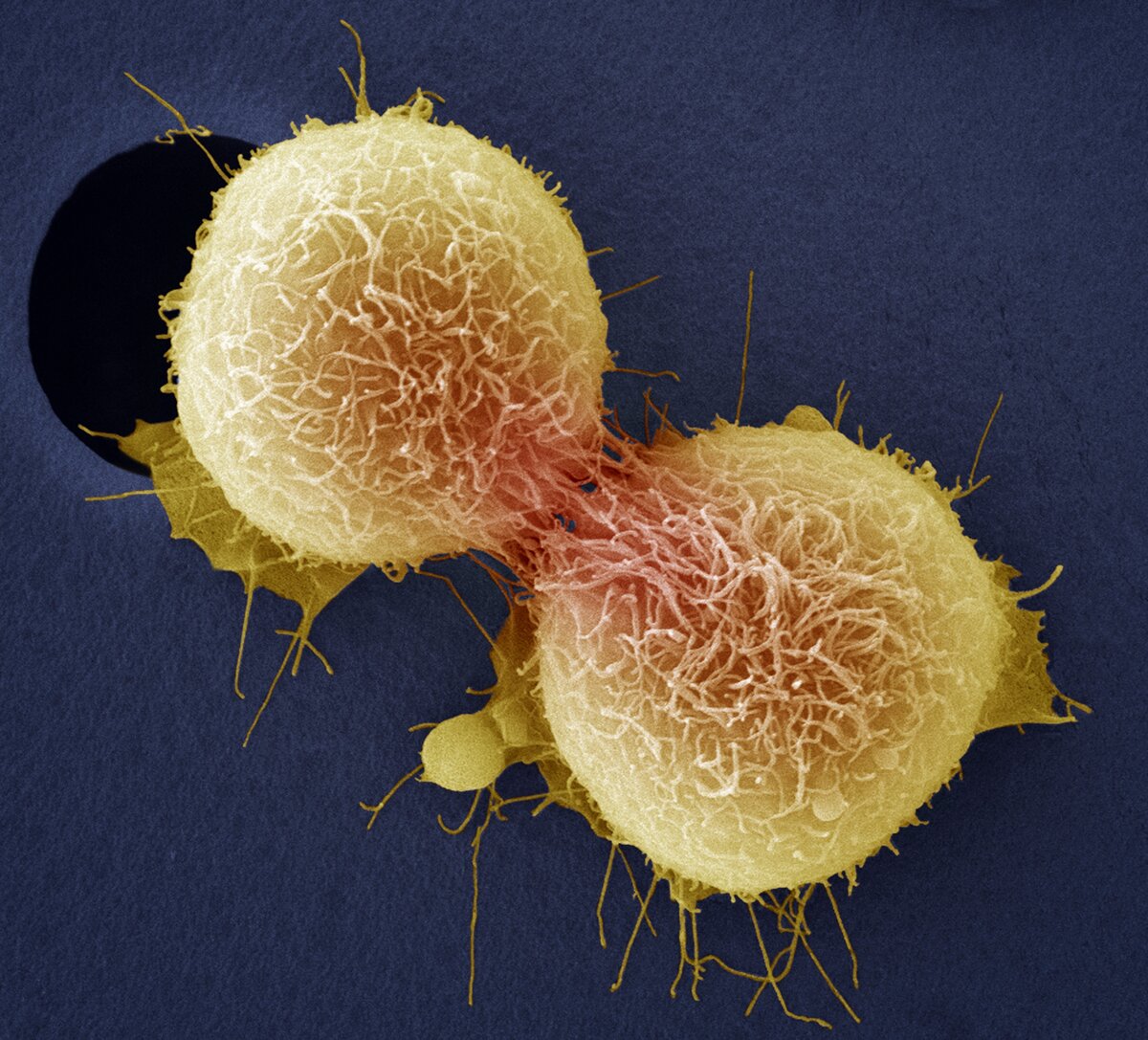
For Cervical Cancer Patients, Less Invasive Surgery Is Worse For Survival

{kind=link}
Cancer of the cervix is one of the most common cancers affecting women and can be fatal. Here, cervical cancer cells are dividing, as seen through a colored scanning electron micrograph.
Steve Gschmeissner/Getty Images/Science Photo Library
hide caption
toggle caption
Steve Gschmeissner/Getty Images/Science Photo Library
A treatment for early stage cervical cancer that has rapidly gained acceptance in the United States turns out to be worse than standard surgery, according to two studies.
The practice, now thrown into question, is called minimally invasive surgery. Instruments are threaded through small incisions, and surgeons use those to remove a diseased uterus. This technique has been growing in popularity since 2006 and has been widely adopted.
But it turns out that minimally invasive surgery for early stage cervical cancer has unexpected risks. The studies were published online Wednesday in the New England Journal of Medicine.
“Patients who underwent the minimally invasive surgery had four times greater likelihood of [cancer] recurrence than when they had the surgery through the open approach,” says Dr. Pedro Ramirez at the MD Anderson Cancer Center in Houston.
That was the surprising result of a study he co-authored comparing the minimally invasive approach to standard surgery though a large incision. The study involved more than 600 women recruited at medical centers worldwide. Half had their uterus removed through open abdominal surgery, the other half had minimally invasive surgery.
A safety board overseeing the experiment called it to a halt before its scheduled completion after it became obvious that women in the minimally invasive group were doing substantially worse.
These women were also less likely to be alive four and a half years following the surgery. About 94 percent of the women were still alive after minimally invasive surgery, compared with 99 percent of women who had standard surgery for the early-stage cancers being studied. (Women with more advanced cervical cancer are generally treated with chemotherapy and radiation rather than surgery).
Ramirez says surgeons at MD Anderson “decided to stop offering the minimally invasive radical hysterectomy and completely convert to the open approach.”
The research team reported its preliminary results at a cancer meeting in March, and since then, Ramirez says, doctors throughout the United States have been reconsidering their approach to treating early cervical cancer.
What’s causing this effect is a bit of a mystery. According to similar high-quality studies, “for uterine cancer, minimally invasive surgery is safe,” Ramirez says. That suggest that cervical cancer cells may be released more readily during a procedure. Ramirez says carbon dioxide gas used to inflate the abdomen during this surgery could also be playing a role.
The study was funded in part by medical device-maker Medtronic. Ramirez said the company had no role in analyzing or publishing the results.
And, making the outcome even stronger, a second study published alongside this report comes to the same conclusion about minimally invasive surgery for early cervical cancer.
For the second report, a research team headed by scientists at Northwestern University looked at national cancer data and found that after four years, 9 percent of the women with minimally invasive surgery had died, versus 5 percent of the women with open surgery.
“That is quite a big deal,” says Masha Kocherginsky, an epidemiologist and co-author of the study. “These patients are early-stage cancer patients, and the intent of surgical treatment is cure.”
What’s more, the researchers noted that the national survival trend for early cervical cancer, which had been improving for years, started to decline in 2006, just as minimally invasive surgery started becoming popular.
Word of these results has spread among physicians, and as a result the national guidelines are already changing to reflect the risks and benefits of these two approaches.
Dr. Emma Barber at Northwestern says she’s now telling her patients about the choice they face. “I think increasingly that’s going to be open surgery for many women,” she says, “but there may still be a role for minimally invasive surgery in some patients.”
You can reach Richard Harris at rharris@npr.org.
Looking For ACA Health Insurance For 2019? Here's What To Expect

{kind=link}
Open enrollment for 2019 health plans begins Nov. 1 on HealthCare.gov and on most state insurance exchanges.
Healthcare.gov via Screenshot by NPR
hide caption
toggle caption
Healthcare.gov via Screenshot by NPR
It’s time for consumers who buy their own health insurance to start shopping for policies for next year. Open enrollment for Affordable Care Act coverage starts Thursday across most of the country.
But the shopping and buying experience will vary widely, depending on where people live.
In California, for example, where political leaders have always been supportive of the Affordable Care Act, legislators have allocated $100 million for outreach.
“We’re going to be hitting the airwaves with TV, radio, interrupting people’s Pandora,” says Peter Lee, executive director of Covered California. “That means that in California the average Californian will hear us, see us, be interrupted by us over 50 times this open enrollment season.”
That sort of hard-sell is crucial if you want to create lower premiums for everyone, Lee says.
“Look, no one thinks they’re going to get sick unless they’re already sick,” he says. “No one wants to spend dollars today for something they think they’re never going to use. You’ve got to sell insurance” to convince healthy people to sign up.
Meanwhile, in states that rely on the federal government’s insurance exchange — mostly conservative states whose leaders opposed the ACA — there won’t be nearly as much outreach to potential customers.
The federal Centers for Medicare and Medicaid Services says it plans to spend about $10 million on marketing nationwide. The effort will include email and text messages to consumers and YouTube videos, according to the CMS website. The agency declined to talk to NPR about open enrollment.
Lee worries that consumers will be confused. With all the political fighting around the ACA, he says, many people believe insurance is now too expensive for them, or don’t realize they likely can get government help to pay their premiums.
“Every place in America — no matter where you live — the subsidies are there today and people should check and find out if they’re eligible for them,” Lee says.
In February 2018, nearly 90 percent of people who had insurance through an exchange qualified for subsidies.
The average premium for a benchmark policy for a 27-year-old is about $405 per month, according to the Department of Health and Human Services. But because of subsidies, the average price a 27-year-old will actually pay is $140 per month.
The Trump Administration has made changes to the ACA’s rules, including gutting the tax penalty for those who don’t buy coverage, and making it easier for some people to buy a short-term policy that doesn’t carry all the consumer protections of an ACA policy. Those changes have added to the cost of some ACA plans, according to Cynthia Cox of the Kaiser Family Foundation.
“Insurance companies, when they set their premiums for the coming year, have to show their math,” Cox says. “They have to justify each element of what is driving up premiums each year — or driving them down.”
The Kaiser Family Foundation analyzed hundreds of filings. And Cox says insurers pointed to the lack of a mandate and the availability of cheaper, short-term insurance to justify their prices. Some companies even mentioned the reduced marketing as as a factor that’s driving up premiums.
Those changes, along with regulatory changes made by the Trump Administration last year, have resulted in premiums being about 16 percent higher than they would have been otherwise, Cox says.
In response, some states have made their own changes. In May, New Jersey adopted it’s own individual mandate. And California banned the sale of short-term health policies that don’t meet ACA standards. Maryland and Alaska have added other programs to stabilize the insurance marketplace. So premiums are stable or even going down in those places, Cox says.
In New Jersey, for example, the monthly premium for a benchmark policy is $289 for 2019 — a decline of 15 percent from 2018’s premiums.
But in Wyoming, it’s a different story. That state has the highest average benchmark premium — $709 a month — according to HHS.
“Rural areas have been particularly hard-hit by high premiums,” Cox says. “There’s not a lot of insurance market competition [there].”
Katie Nicol, senior manager of public benefits and insurance navigation at Whitman-Walker Health in Washington, D.C., helps people choose insurance plans.
“Our biggest role as navigators is to really ensure that people understand that the ACA is still the law of the land, and that the marketplace will be up and running [as of]Nov. 1,” Nicol says.
The deadline to sign up for new insurance on Healthcare.gov is December 15. But some states, including California, have enrollment periods that extend into January.
Language Barrier Means Millions Of Elderly Can't Access Alzheimer's Trials

{kind=link}
Getting people of different ethnicities and cultural backgrounds into clinical trials is not only a question of equity, doctors say. It’s also a scientific imperative to make sure candidate drugs work and are safe in a broad cross-section of people.
Richard Bailey/Getty Images
hide caption
toggle caption
Richard Bailey/Getty Images
Sign up for the CommonHealth newsletter to receive a weekly digest of WBUR’s best health, medicine and science coverage.
My grandmother, Bella, a former nurse in the Ukraine, moved to the United States to help raise me when I was 7 months old. She was diagnosed with Alzheimer’s disease last year.
There was nothing to do to prevent her inexorable loss of memory and independence, her Massachusetts General Hospital memory specialist told our family, except to take a drug called memantine that slightly improves cognition in Alzheimer’s patients, but does not treat the underlying disease.
Only one other type of drug, which acts on how nerve cells communicate, has been approved to treat the cognitive problems that come with Alzheimer’s. Notably, both drugs have been around more than 15 years. And neither one changes the course of the disease.
While there are no drugs to treat the underlying disease, there are a number of clinical trials underway. And those trials are in desperate need of patients to enroll. Trials can be risky for patients and are far from guaranteed to help them, but there is no other way medical researchers learn whether their experimental therapies are safe and effective.
But it turns out that many patients like my grandmother, who do not speak English fluently — and millions of other immigrants, mainly Spanish speakers — can’t participate.
According to interviews with doctors, government officials and pharmaceutical companies, few Alzheimer’s studies include medical interpreters to help patients complete the specialized neuropsychological testing component required.
One of the challenges is that clinicians and researchers have strongly cautioned against using interpreters to facilitate neuropsychological testing based on clinical experiences, observations and anecdotal evidence that they affect outcomes, according to a study published in Clinical Neuropsychology.
Dr. Benjamin Sommers, who studies health policy for vulnerable populations at the Harvard T.H. Chan School of Public Health, says the problem goes beyond clinical trials and affects diagnosing as well. He recently had trouble arranging for neuropsychological testing to diagnose a Spanish-speaking patient who did not speak English fluently.
The language barrier is a “real issue for mental health disparities,” says Sommers, who is also a primary care physician at Brigham & Women’s Hospital in Boston. “It’s very hard to find a hospital in the [Boston] area that does Spanish-language dementia testing,” he says. “There are months-long waiting times — sometimes up to six months. And sometimes such testing is not available at all.”
The barriers to Alzheimer’s trials may be felt most acutely by Hispanics in the U.S. According to census data, almost 6 million Americans are age 60 or older. That includes about 2.2 million Spanish speakers who are 65 or older and do not speak English very well.
The challenges are likely to get worse in the coming decades, says Jason Resendez, executive director of LatinosAgainstAlzheimer’s and chief of staff at UsAgainstAlzheimer’s, an organization that lobbies to find a cure for the disease.
Latinos represent the country’s fastest-growing over-65 demographic and are predicted to be 50 percent more likely to get Alzheimer’s than non-Latino whites, according to a report released by the University of Southern California, he notes.
“We know Latinos will make up a bigger and bigger share of the community living with Alzheimer’s in the future,” Resendez says. “And we know that we don’t have the workforce pipeline in place to accurately diagnose and enroll these folks into cutting-edge research.”
Getting people of different ethnicities and cultural backgrounds into clinical trials is not only one of equity, Resendez says, “it’s also a scientific imperative. We need to know whether a drug developed for Alzheimer’s is going to work the same in Caucasians as it does in African-Americans and other cultures.”
UsAgainstAlzheimer’s has launched an initiative called the Alzheimer’s and Dementia Disparities Engagement Network that aims to track disparities in access to Alzheimer’s and dementia care for minorities and display them publicly on a ZIP code map.
“We’ll be able to look at whether there’s language-accessible services and research in these areas, and if not, what we can do about it,” Resendez says. “We think that making the data accessible and actionable is going to be the foundation for addressing these issues at a national level.”
LatinosAgainstAlzheimer’s is also helping build the government’s new Latino task force on Alzheimer’s, whose goal will be to determine how to improve outreach and recruitment in the Spanish-speaking dementia community, he adds.
Currently, there seems to be little government policy on the issue.
Dr. Eliseo J. Pérez-Stable, the director of the National Institute on Minority Health and Health Disparities, says that the National Institutes of Health has no policy on clinical trial access for non-native English speakers, while acknowledging that it would be humane to include them. “I don’t think we have an easy answer for this yet,” he says.
A glimmer of hope for non-English speaking dementia patients may lie in the work pharmaceutical companies such as Eli Lilly are doing. Joe Kim, senior adviser in patient experience and design innovation at Eli Lilly, says that his team is exploring telemedicine as a way to enable broader access to clinical trials.
“If we can virtualize trials and allow patients to enroll remotely, not only would it lower the burden on patients but it would also expand the patient population that’s eligible for the trial.”
Kim is optimistic that in the future, a group of patients more representative of the American population will have access to clinical trials. “We’ve done one virtual trial already, and we found we can get a more diverse population,” he says. “With the rise of digital health care, I think we have a lot of tailwind. This will enable medical care to be democratized.”
Meanwhile, time is not on my grandmother’s side. I have noticed in our weekly phone conversations that she is forgetting common words and idioms in Russian. They are on the tip of her tongue, but beginning to recede from memory.
Indeed, she herself is receding.
Josh Eibelman, a junior at Cornell University, was born and raised in Boston. You can email him here.
GOP Revives Medicare Scare Tactics As Election Nears
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.
Bill Of The Month: A $48,329 Allergy Test Is A Lot Of Scratch
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.
2 Moves By Trump This Past Week Could Reshape U.S. Health Insurance In Big Ways
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.
Trump Aims To Lower Some U.S. Drug Spending By Factoring In What Other Countries Pay
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.
Methamphetamine Roils Rural Towns Again Across The U.S.
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.
2018 Is The Year Democrats Got Comfortable Talking Health Care Again
By choosing “I agree” below, you agree that NPR’s sites use cookies, similar tracking and storage technologies, and information about the device you use to access our sites to enhance your viewing, listening and user experience, personalize content, personalize messages from NPR’s sponsors, provide social media features, and analyze NPR’s traffic. This information is shared with social media services, sponsorship, analytics and other third-party service providers.
See details.