Big Jump In Number Of Inmates Prescribed Psychiatric Drugs In California

An average of 13,776 inmates in the 45 California counties were on psychotropic medications in 2016-2017, a recent report found. That’s up from 10,999 five years ago.
erwin rachbauer/imageBROKER RM/Getty Images
hide caption
toggle caption
erwin rachbauer/imageBROKER RM/Getty Images
When 47-year-old Edward Vega arrived in jail, he couldn’t quiet the voices in his head. He felt paranoid, as though he was losing control. “I knew if I didn’t get my medication, I was going to hurt someone,” says Vega.
He was right. A week after being arrested for alleged drug possession, Vega says, he assaulted a fellow inmate and ended up in isolation, which only made him feel worse.
Finally, a doctor prescribed medicines that Vega says helped. He’d been taking them on the outside until he ran out — just before he was arrested.
“The medication hasn’t totally taken away the voices, but I am able to differentiate reality from fiction,” says Vega, who was released three months ago.
The number of inmates in California who’ve been prescribed psychiatric drugs has jumped about 25 percent in five years, according to a recent analysis of state data. These inmates now account for about a fifth of the county jail population across the state.
The increase might be a reflection of the growing number of inmates with mental illness, though it also might stem from better identification of people in need of treatment, say researchers from California Health Policy Strategies, a Sacramento-based consulting firm.
Amid a severe shortage of psychiatric beds and community-based treatment throughout the state and nation, jails have become repositories for people in the throes of acute mental health crises.
The number of people with mental illness in jails and prisons in the U.S. is “astronomical,” says Michael Romano, director of Three Strikes & Justice Advocacy Project at Stanford Law School, who was not involved in the research. “In many ways, the whole justice system is overwhelmed with mental illness.”
Contributing to the problem in California is a 2011 federal court order, and a state decision a few years later, that had unintended consequences.
In 2011, the U.S. Supreme Court ordered California to reduce the prison population because of overcrowding that the judges said constituted cruel and unusual punishment. Three years later, a state proposition reclassified some felony crimes as misdemeanors. Taken together, that led to a huge influx of offenders going to county jails instead of state prisons.
The CHPS analysis, based on survey data from 45 of California’s 58 counties, opens a window into how the largest state is coping with the influx.
“We think this is the first part of a more systematic discussion about what is going on in the jails and in the broader community with respect to mental health,” says David Panush, a co-author of the report, which was funded in part by the California Health Care Foundation.
Far more people with mental illness are housed in jails and prisons than in psychiatric hospitals. Insufficient staff training and poor patient treatment have contributed to inmate suicides, self-mutilation, violence and other problems, say advocates for the mentally ill.
One oft-cited complaint is that inmates have poor access to psychiatric prescriptions to treat such conditions as schizophrenia, major depression and bipolar disorder.
Jail officials in California say they are trying to better identify incarcerated people who could benefit from such drugs. The numbers suggest the strategy may be working. According to the CHPS report, an average of 13,776 inmates in the 45 California counties were on psychotropic medications in 2016-2017, up from 10,999 five years ago.
But the portion of inmates taking psychotropic medicine varies widely by county — from 8 percent in Glenn County to 32 percent in Sonoma and Napa, according to the analysis. The report is based on data from the Board of State and Community Corrections, an independent state agency.
In Los Angeles County, whose jails have been described as the largest mental institution in the country, about 30 percent of the roughly 18,000 inmates are mentally ill and most of those diagnosed are on medication, says Dr. Joseph Ortego, chief psychiatrist for correctional health services in L.A. County.
Although some still are missed in the screening process, he says, the county jails have improved identification and treatment of inmates and expanded staffing as part of the department’s 2015 settlement with the U.S. Department of Justice. The department had alleged inadequate mental health care and suicide prevention in the jails.
Overall, medications are likely under-prescribed in jails, psychiatrists say.
“You need enough mental health professionals to treat the very large numbers of mentally ill people in jails,” says Dr. H. Richard Lamb, professor emeritus of psychiatry at the University of Southern California School of Medicine. “There probably aren’t enough.”
And the medications these doctors prescribe are a crucial aspect of treatment, Lamb says.
Some advocates for the mentally ill worry that the drugs are at times prescribed inappropriately. Zima Creason, president and chief executive officer of Mental Health America of California, says psychoactive medicines, though sometimes necessary, are no substitute for comprehensive care for jail inmates.
“Sadly, they just throw a bunch of pills at them because there is nothing else,” she says, adding that jails should also be providing individual and group therapy, more time outside of cells and sufficient recreation time.
“Jail is not conducive for real recovery,” Creason says. “We are never going to put a dent in the numbers unless we provide a therapeutic environment.”
Like people who live outside the correction facilities, inmates can be subject to involuntary drug treatment, officials say, but only if a court deems that step appropriate.
County jail officials, including Dr. Alfred Joshua, chief medical officer for the Sheriff’s Department in San Diego County, say the influx of mentally ill inmates and the rising need for psychotropic drugs stems from a lack of resources for patients in the community.
“When they have [an] exacerbation of mental illness, they do many times come into contact with law enforcement,” Joshua says.
Some of the most common charges that bring people with mental illness to jail are drug offenses and parole violations. Those who are homeless frequently get charged with panhandling, public urination and related crimes.
In addition to trying to improve treatment inside the jails, Los Angeles and San Diego county officials say they are working more closely with community organizations to ensure inmates with mental illness get the services they need after their release.
Vega says a local community group, the Neighborhood House Association, was able to help in his case, ensuring he got his meds and other treatment.
“Without the medication,” Vega says, “I would probably be right back in jail.”
Kaiser Health News is an editorially independent program of the Henry J. Kaiser Family Foundation, a nonprofit, nonpartisan health policy research and communication organization not affiliated with Kaiser Permanente. You can follow Anna Gorman on Twitter: @annagorman.
British Health Services Failed To Send Mammogram Notices And Some Women May Have Died

Britain’s Health and Social Care Secretary Jeremy Hunt arrives at 10 Downing Street in central London on March 13.
Daniel Leal-Olivas/AFP/Getty Images
hide caption
toggle caption
Daniel Leal-Olivas/AFP/Getty Images
A “computer algorithm failure” in the U.K. kept hundreds of thousands of women from getting notified it was time for a mammogram, potentially shortening the lives of up to 270 women, the National Health Service says.
The U.K. sends letters to women who are due for breast screening, according to British national guidelines, which call for exams every 3 years for women age 50-70. Because of the computer glitch, an estimated 450,000 women in England around the age of 70 did not receive their mammogram invitation.
Health Secretary Jeremy Hunt announced the “serious failure” on Wednesday, apologizing to the women affected.
My thoughts today with the thousands of women and families affected by failures in our breast cancer screening programme. We will get to the bottom of this so we can stop it happening again.
— Jeremy Hunt (@Jeremy_Hunt) May 2, 2018
“At this stage it is unclear whether any delay in diagnosis will have resulted in any avoidable harm or death,” Hunt said.
An independent review will work to answer that question, but in the meantime, preliminary statistical models show that as many as 270 women may have “had their lives shortened as a result” because of the glitch, Hunt said.
David Spiegelhalter, a British statistician, notes that Hunt’s announcement could be misinterpreted to mean hundreds of women died because of missed mammograms. But the total number likely includes women who have not yet died.
None of that takes away from the fact that the government made a painful mistake, Spiegelhalter said.
“There is no doubting that Jeremy Hunt needed to make a strong apology,” he wrote.
The government says new screening notifications will be sent English women 70-72 who missed their notifications. For older women, for whom the benefit of such screenings is less clear, optional screenings will be available.
The Times reports that the NHS and Public Health England, which administers the screening problem, are pointing fingers at each other, with each group suggesting the other body is to blame for the glitch.
Meanwhile, the Royal College of General Practitioners says “the priority should not be to establish blame” but rather to address the demand for mammograms and prevent such a problem in the future.
In the United States, which does not have a universal health care system like the U.K., there is no equivalent centralized process for notifying women they are due to have a mammogram.
Otis Brawley, the chief medical officer of the American Cancer Society, tells NPR that some HMOs and mammogram facilities will send out reminders, but it’s not typical.
“The overwhelming majority of women in the United States, it’s expected they or their physician will remember when it’s time to get a mammogram,” Brawley says.
And the need for screenings in older women, like those affected by the U.K. debacle, is not widely discussed, Brawley says — even though 50 percent of breast cancers are diagnosed in women age 67 or above.
However, as a woman gets older, a breast cancer detected by a mammogram is also less likely to end her life, Brawley notes. Meanwhile, unneeded treatment of such cancers could have serious side effects, as NPR’s Rob Stein reported last year.
That’s why the U.K. stops testing women in their 70s, and why the ACS doesn’t recommend mammograms for women with a life expectancy of 10 years or less.
Brawley also emphasizes that many women diagnosed with cancer find the cancer themselves, and encouraged all women to be aware of any changes in their breasts.
Veterans Groups Concerned That Lack Of VA Leadership Will Hurt Millions Of Veterans

The Department of Veterans Affairs still lacks a secretary and many inside and outside the vast agency say a lack of leadership is affecting its mission.
Sprained Your Ankle? The Cost Of A Walking Boot Could Sprain Your Wallet

Under the Affordable Care Act, many insurance plans are required to cover a range of essential services, such as hospitalization and prescription drugs. But reimbursement for certain medical equipment — such as crutches or a leg boot after an injury — varies widely from plan to plan.
tirc83/Getty Images
hide caption
toggle caption
tirc83/Getty Images
One July evening a few years ago, Carol Harnett was in a crosswalk in downtown Portland, Ore., when a driver made an illegal turn and hit her.
Transported by ambulance to a hospital, Harnett, who is president of the nonprofit Council for Disability Awareness, was diagnosed with a severely sprained right ankle and left wrist, as well as a concussion.
At the emergency room, doctors gave her steel-reinforced braces for her wrist and ankle and told her she was free to go.
“But I can’t walk,” Harnett recalls saying. With a third-degree sprain, the ligaments in her right ankle were completely torn and she couldn’t bear weight on it.
“They said, ‘If you broke a bone, we could give you a wheelchair, but you didn’t — so, we don’t think your insurance will cover it,’ ” she recalls. Instead, after she signed a waiver agreeing to pay whatever her insurance didn’t cover, they gave her a pair of crutches to use while in Portland to give a speech.
Her hotel was more accommodating, loaning her a wheelchair at no charge.
Unless you’ve already had need of such equipment, chances are you have no idea how your insurance policy would cover the wheelchair, walker or knee brace you might require if you had a car accident or got hurt on the ballfield or tripped on the stairs.
The cost for “durable medical equipment,” as these devices are called, may be small compared with the bills for emergency or specialist medical care. But if you’re paying for such equipment out-of-pocket, the costs can add up — it’s worth your time to look into your coverage and figure out how to get the best deal.
Harnett’s 2015 accident was later determined to be work-related, and the workers’ compensation program paid for her care. If that hadn’t been the case, she would have been on the hook for the crutches, because her own insurance plan didn’t cover any durable medical equipment that could be purchased over the counter. It would have covered the reinforced braces for her wrist and ankle, but only after she met her deductible.
“Historically, [durable medical equipment] has always been a weak point in coverage,” says Harnett, who is familiar with these insurance issues because of her disability work. A typical employer-based health plan covers 80 percent of the cost after the deductible is met, according to Harnett.
But some consumers may not get that benefit. “We’re seeing more skinny plans with no durable medical equipment coverage at all,” says Thomas Ryan, president and CEO of the American Association for Homecare, an advocacy organization for home care equipment manufacturers and providers.
Insurers often have preferred providers
Under the Affordable Care Act, many insurance plans are required to cover a range of essential services, such as hospitalization and prescription drugs. But durable medical equipment isn’t among them — except for breast pumps, which most plans must cover.
These days, insurers often contract with certain medical supply companies to provide equipment, just as they negotiate rates for other services. But patients often don’t realize that, says Alice Bell, a physical therapist and senior payment specialist at the American Physical Therapy Association, a professional group. Patients who don’t use an insurer’s preferred provider may be charged a higher rate or have to pay the entire amount out-of-pocket, she says.
“It’s important to make sure the supplier is in-network, even if the doctor prescribes it, because it varies,” Bell says.
When Bruce Lee, 48, strained a ligament in his left leg, his doctor prescribed a walking boot and gave him a list of medical suppliers. The doctor warned Lee to make sure he chose one in his insurance network.
Lee selected a supplier near his Fairfield, Conn., home that he described as a “medical Disneyland” of assistive devices. Although it was convenient, the supplier didn’t accept his insurance. He paid about $320 for the boot and used his flexible spending account to cover the cost.
To make matters more confusing, hospitals, urgent care centers and physicians may themselves negotiate with insurers or Medicare to become an approved supplier of medical equipment for their patients, or they may contract with a medical supply company to provide those items.
Wanda Wickizer didn’t know what to think when her 23-year-old daughter got a $40 bill from a medical supply company for a wrist brace she received at an urgent care center after falling down some stairs at a friend’s house in Norfolk, Va.
The company was in her daughter’s insurance network, as it turned out.
Still, “it boggled my mind that they were allowed to bill her, because she never saw anyone from there,” Wickizer says.
Whatever the arrangement, the key for the patient is to find out whether whoever is supplying the equipment is in their insurance network and how much they’ll owe out-of-pocket. You have to ask.
Insurers might approve coverage of medical equipment only if a provider certifies it’s medically necessary. Even with a doctor’s OK, approval isn’t assured. The “fancier” a piece of equipment is, the more challenging it is to get an insurer to agree that it’s medically necessary, says Dr. Angela Gardner,who practices in Dallas and is a past president of the American College of Emergency Physicians.
“In general, for a commercial [insurer], basic crutches will be covered, forearm crutches are partially covered, and hands-free crutches won’t be covered,” she says, referring to a crutch that attaches to the injured leg and allows someone to move around without relying on their hands or arms.
Yet for some patients, shopping around for such equipment is not an option. They need it on the spot or, like Harnett, are unable to get around well enough to go somewhere to buy it. If the patient can wait, many medical device suppliers deliver equipment to the home, or the devices can be purchased online.
Opting not to use insurance
Beyond weighing in- and out-of-network options, patients have an option on durable medical equipment they don’t typically get when choosing medical services: buying over the counter.
Sometimes this proves significantly cheaper than using an insurance plan. A pair of standard armpit crutches, for example, may cost $40 at the local pharmacy, while the insurance copayment might be $100.
“A savvy consumer will look at the copay and see whether or not they need to use their insurance,” Gardner says.
Sometimes the prices insurers agree to pay for durable medical equipment are significantly higher than the price online or at the drugstore. That differential can be important if someone has a high-deductible plan and has to pay the entire amount.
An orthopedist suggested that Barbara Barrall, of Medford, N.J., replace her simple knee brace with a hinged model she could bend. When the bill arrived, Barrall’s daughter, Cynthia B. Sosnowski, thought the $1,400 charge must be a mistake. She went online and found the identical brace for between $79 and $99 at sporting goods and medical supply stores.
But when she called the orthopedist’s office, the woman said there was no mistake. That was the amount the doctor was allowed to charge the insurer. When Sosnowski called the insurer, she was told not to worry: Her mother’s share of the charge was $145; the rest was covered by her mom’s employer-based plan for retirees.
Sosnowski wasn’t placated. “This is why insurance is so expensive in our country,” she says.
She’s since filed a grievance with the insurer to protest the charge.
Kaiser Health News, a nonprofit news service, is an editorially independent program of the Kaiser Family Foundation, which is not affiliated with Kaiser Permanente.
Planned Parenthood Sues To Block Trump's 'Radical Shift' In Family Planning Program

President Trump shakes hands with Health and Human Services Secretary Alex Azar after he is sworn in by Vice President Pence on Jan. 29. Major reproductive health organizations are voicing concerns about the Trump administration’s new approach to federal family-planning grants, which may reduce the role of Planned Parenthood and place greater emphasis on “natural family planning.”
Andrew Harnik/AP
hide caption
toggle caption
Andrew Harnik/AP
Updated at 11:50 a.m. ET
Three national reproductive rights groups are suing the Trump administration, arguing that changes to the federal Title X program will put the health of millions of low-income patients at risk by prioritizing practices such as the rhythm method over comprehensive sexual health services.
The two lawsuits filed Wednesday — one by about the state budget here: https://t.co/GAD5jYtjpA
— Gov. Pete Ricketts (@GovRicketts) April 4, 2018
Texas: Revisiting federal funding — without Planned Parenthood in the mix
Under the Obama administration, Texas was excluded from receiving Title X family planning funds because of the state’s ban on public funds going to organizations that provide abortions. Now, Texas officials see an opportunity to recapture that funding while maintaining that prohibition.
In March, Texas Attorney General Ken Paxton wrote a letter to HHS Secretary Alex Azar asking the state to be allowed to receive those funds under the Trump administration:
“In light of the recent statements by … President Trump,” Paxton wrote, “… and communications that Texas officials had with members of your agency last Fall, Texans are encouraged that cooperative participation to accomplish the objectives of the Title X program, is yet again possible.”
Federal Government Sends Warning To Vaping Companies

E-Liquid (right) with labeling that resembles kid-friendly candy (left).
FDA/Flickr
hide caption
toggle caption
The Food and Drug Administration and Federal Trade Commission on Tuesday sent warning letters to 13 manufacturers, distributors and retailers of e-cigarette liquids. In a phone briefing for reporters, FDA Commissioner Scott Gottlieb said the companies are endangering kids by marketing the products to resemble juice boxes, cookies or candy.
“You look at the lollipop for example. I don’t see how my 4- or 5-year-old doesn’t just look at that and see a lollipop. It’s a lollipop,” he said.
E-liquids are used in electronic cigarettes, and they often use nicotine which can cause illness — even death — if ingested by a small child. Products targeted have names like Smurf Sauce and V’Nilla Cookies & Milk.

Two U.S. government agencies are warning companies that sell vaping products that their packaging resembles candy and may be in violation of safety and marketing guidelines because of its possible appeal to teens and children.
Food and Drug Administration
hide caption
toggle caption
Food and Drug Administration
“These are being deliberately designed in ways that they can be just mistakenly confused by a child,” Gottlieb said in the briefing.
The agencies cited recent national data of thousands of nicotine exposures in kids younger than 6, who accidentally ingested the vaping liquid. The letters and violations vary somewhat by company but, overall, the letters say the products’ appeal to minors violates parts of the Federal Food, Drug and Cosmetic Act, which gives the FDA authority over marketing and distributing tobacco products.
“Today’s announcement should send a clear signal that companies selling these products have a responsibility to insure they aren’t putting children in harm’s way or enticing youth use,” Gottlieb said. He warned more actions would be coming.
Jameson Rodgers is vice president of business development for California-based NEwhere Inc., one of the companies that received a letter. He says his company’s products are only for adults who want to switch to vaping from traditional cigarettes, which he says are less healthful. The FDA targeted the company’s One Mad Hit Juice Box e-liquid. Rodgers says the company voluntarily removed it from distribution last year.
“We definitely didn’t intend to position it as a product that would appeal to anybody who wasn’t of legal smoking age,” he says, though he admits it might have sent a “questionable” message.
Ray Story, CEO of an industry trade group based in Georgia called the Tobacco Vapor Electronic Cigarette Association, says he welcomes the federal agency crackdown on what he calls “fly by night” companies targeting minors.
“Really would you buy a product, a vape with the name Dancing Monkey or Cotton Candy? At the end of the day we’re trying to create products that have the ability to compete against Big Tobacco,” he says. According to its website, TVECA is a nonprofit dedicated to “create a sensible and responsible electronic cigarette market” by providing education, communication and research to media, lawmakers and consumers.
Tuesday’s warning letters are part of a larger push by the federal government to crack down on youth access to tobacco products, including vaping. Last week the FDA sent a warning letter to 40 retail stores for selling the e-cigarette brand Juul to minors. They also asked the company for research on its appeal to children and teenagers. Health officials say Juul is highly addictive, and it’s so new there’s scant research about its health effects.
The companies targeted Tuesday have 15 days to respond — to either defend their practices or explain how they’ll change their labeling, or risk federal action such as fines or prosecution.
This story is part of a reporting partnership with NPR, Colorado Public Radio and Kaiser Health News.
Questions Raised About Study Of Device To Ease Opioid Withdrawal

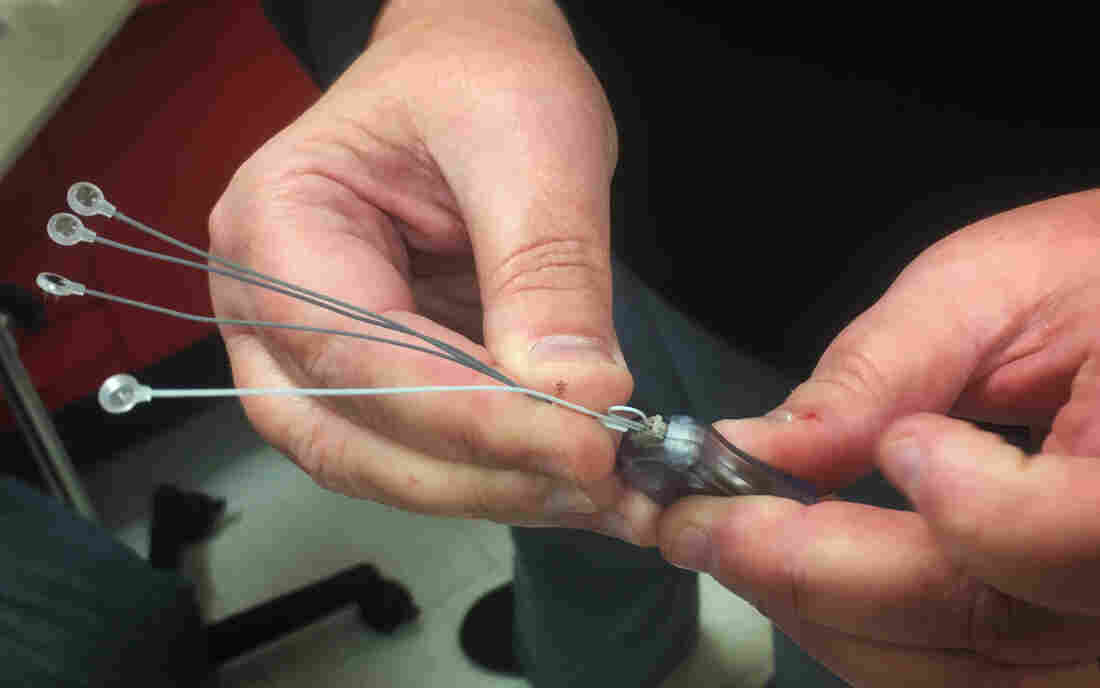
The Bridge, a medical device worn behind the ear, delivers electronic pulses to ease the symptoms of opioid withdrawal.
Maria Fabrizio for NPR
hide caption
toggle caption
Maria Fabrizio for NPR
To the untrained, the evidence looks promising for a new medical device to ease opioid withdrawal. A small study shows that people feel better when the device, an electronic nerve stimulator called the Bridge, is placed behind their ear.
The company that markets the Bridge is using the study results to promote its use to anyone who will listen: policymakers, criminal justice officials and health care providers.
The message is working.
In the face of a nationwide crisis of opioid addiction, people are eager for new solutions. Criminal justice officials in multiple states have started Bridge pilot programs. At least one such program in Indiana received state funds. Providers with a major hospital chain in Indiana began prescribing the Bridge. And politicians in Indiana, Utah and Ohio publicly touted the device.
Innovative Health Solutions, the device maker, has marketed the Bridge for opioid withdrawal for more than a year, even before it had clearance for that use from the Food and Drug Administration. Then, last November, the Versailles, Ind.-based company got that, too. Citing the study, the FDA allowed the Bridge to be promoted for opioid withdrawal.
Indiana State Sen. Jim Merritt, a Republican who is known for sponsoring legislation addressing the opioid crisis, held an effusive press conference after the FDA gave its OK to the Bridge. “People will detox,” he told reporters. “They will withdraw from drugs if it’s a simpler process, and this is it.”
But some addiction specialists aren’t persuaded by the evidence behind the device. The study informing the agency’s decision didn’t randomly compare the experience of patients treated with the device with others who got a sham treatment. Andy Chambers, an addiction psychiatrist in Indianapolis, said there’s no way to know if the $595 device works, or if patients and providers simply believe that it does.
“For the sake of patients, I do hope the Bridge works,” Chambers wrote in a letter published in the Indianapolis Star in November. “But for me to use it in regular practice, don’t show me a sales job, or the enthusiasm of lobbyists, politicians or prosecutors; just give me the solid science.”
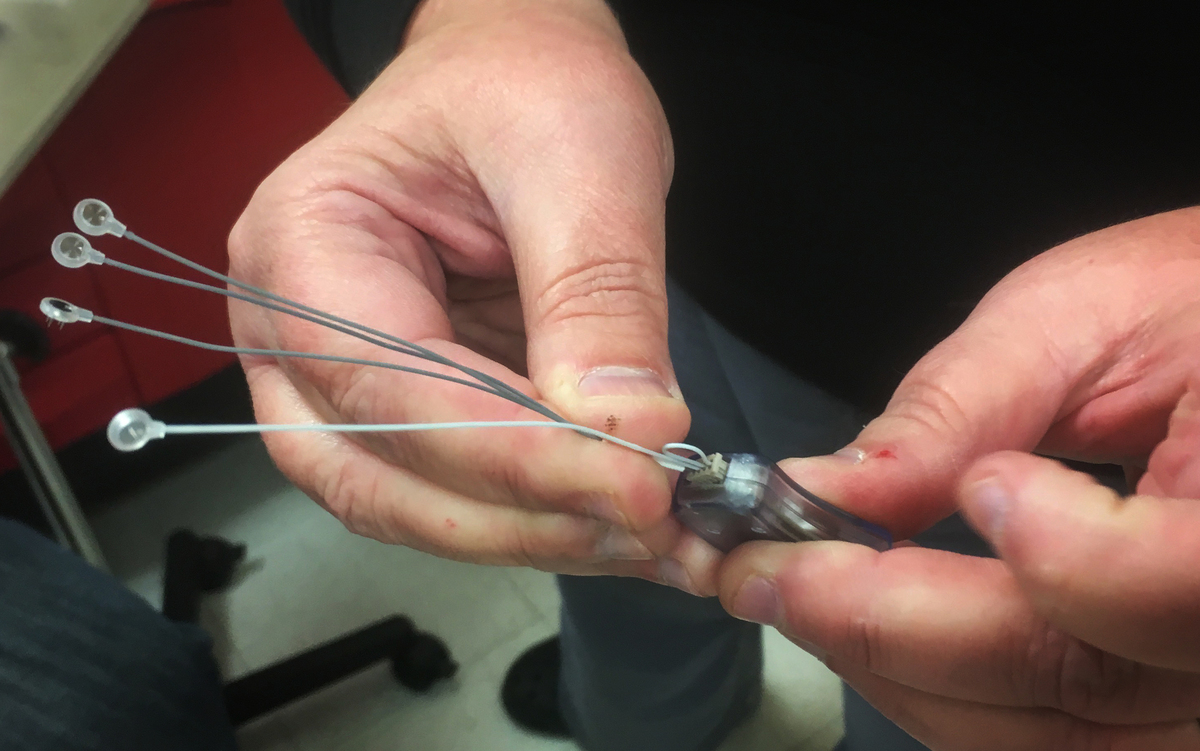
The company that markets the Bridge device claims that its electronic pulses stimulate branches of certain nerves that emanate directly from the brain to help people quit opioids.
Jake Harper/Side Effects Public Media
hide caption
toggle caption
Jake Harper/Side Effects Public Media
An investigation by Side Effects Public Media and NPR reveals that researchers working with Innovative Health Solutions, maker of the Bridge, submitted to a medical journal a study that wasn’t what it appeared to be. The study authors said it was a “retrospective study,” which means they would have simply reviewed existing medical data. But it seems that they instead conducted a clinical trial that skirted FDA rules and ethical norms, using vulnerable people suffering from addiction as test subjects. The FDA then relied on the results of the study in making its decision to clear the Bridge for marketing as a treatment for opioid withdrawal.
In a response to questions from Side Effects and NPR, the FDA said it cleared the Bridge for use in opioid withdrawal because the study demonstrated “a clinical benefit that outweighs the risk of the device.” The agency also said it is reviewing the issues raised by the investigation but didn’t say what, if any, action it might take.
Innovative Health Solutions said that company representatives and researchers followed FDA rules when the study was conducted.
To Chambers, the FDA decision in favor of the Bridge was another sign of unsupported enthusiasm for the device. Chambers said policymakers and clinicians should support the use of proven therapies, instead of the Bridge. “You’re potentially draining money away from other treatments that we know are efficacious,” Chambers said.
The experiment
On a cold December afternoon in Liberty, Ind., James was sweating. (Because of his drug use, Side Effects and NPR agreed not to use his full name to protect his identity.) He showed up at the Union County Health Department to get help with his opioid withdrawals. It had been two days since he last used.
“I get hot and cold chills,” he said as he waited. “In two seconds, it changes. It’s crazy.” His dark hair, flecked with gray, was damp with perspiration. His legs ached, he had diarrhea and hadn’t slept the night before.
After several minutes a nurse ushered James into an exam room. She assessed his withdrawal symptoms, and then began to fasten the Bridge around his ear, tiny needles piercing his skin. When the final electrode was in place, James said he could feel the mild pulse of electricity emitted by the device.
The company claims these pulses stimulate branches of certain nerves that emanate directly from the brain. The idea is that this stimulation can relieve symptoms of withdrawal.

Jeff Mathews’ treatment program, which operates out of the Union County Health Department in Liberty, Ind., helped collect data for the study of the Bridge.
Jake Harper/Side Effects Public Media
hide caption
toggle caption
Jake Harper/Side Effects Public Media
James had used drugs since his teens. He’d tried to quit before, but couldn’t. Jeff Mathews, a county official who runs the treatment program, told James the Bridge could help him stop using opioids so that he could get treatment with Vivitrol, a monthly shot of the opioid-blocker naltrexone.
“I know this thing sounds too good to be true,” Mathews told him. “I’ve seen it repeatedly. It’s going to do exactly what we say it does.”
Over the next hour, James said his symptoms got better. He stopped sweating, his mood improved and his goosebumps disappeared.
“I’m ready to quit,” said James. “I want my family back.”
“I’m sure they want you back, too,” the nurse replied.
The nurse told James to leave the Bridge in place and come back five days later. If he tested negative for opioids, he’d move on to Vivitrol.
But James never returned.
Scientific shortcuts
The idea of using the Bridge for opioid detox came from Arturo Taca, an addiction psychiatrist who practices near St. Louis. Taca worked with Brian Carrico, now the president of Innovative Health Solutions, to adapt the company’s existing nerve stimulator (a device which was already cleared by the FDA for treating pain in 2014) so it could be worn during withdrawal, as the website STAT previously reported.
Taca also developed instructions for using the device as a “bridge” to treatment with Vivitrol.
Taca started promoting this use of the device. Innovative Health Solutions did, too, as early as 2016, before it had gotten the green light from the FDA for this use. Without explicit permission, this marketing by the company is called off-label promotion, which violates FDA regulations.
“They are they are not allowed to promote off-label use period, whether it’s to a physician, whether it’s to a judge, whether it’s to just a random person in the public,” said Basia, Andraka-Christou, a health policy researcher at the University of Central Florida who reviewed the company’s presentation.
There is an obvious market for the Bridge. As Side Effects and NPR reported last year, Alkermes, Vivitrol’s manufacturer, had been aggressively pushing its medicine to lawmakers and in criminal justice settings. Vivitrol, an opioid-blocker, can be especially appealing to people who are opposed to the other two FDA-approved medicines for opioid addiction — methadone and buprenorphine — which are both long-acting opioids themselves. They ease symptoms of withdrawal and reduce cravings, but some critics view them as replacing one opioid with another.
The Bridge can appeal to Vivitrol advocates, because to start that medicine, patients need to make it through opioid withdrawal.
But for Innovative Health Solutions to legally market the Bridge for opioid withdrawal, it needed the FDA’s OK. To get it, the company presented the agency with results from a study published in the American Journal of Drug and Alcohol Abuse in March 2017. The paper was written by Taca and Adrian Miranda, a pediatric gastroenterologist and professor at the Medical College of Wisconsin.
Reporting by Side Effects and NPR shows that the company and study authors took shortcuts in the research that violated FDA regulations.
The authors call it a “retrospective assessment,” claiming they reviewed medical records from patients who had been treated with the Bridge.
But it was not a retrospective assessment, reporting by Side Effects and NPR finds.
Innovative Health Solutions and Taca recruited health care providers to conduct a clinical trial. The company and Taca told them to measure withdrawal symptoms at specific intervals. According to instructions laid out in documents obtained by Side Effects and NPR, providers would then submit those data online, which wouldn’t have been necessary unless the data were being gathered for study purposes.
The FDA requires strict oversight of clinical trials to protect patients and ensure the study results are valid. The Bridge study had no such oversight.
The treatment program in Liberty is run by Jeff Mathews, a retired Navy man, who heard about using the Bridge for opioid withdrawals from Carrico in January 2016.
Mathews was intrigued. “If this thing does what you say it does, this is a game changer,” he told Carrico.
Mathews said he struck a deal with the company. “I’m a shrewd negotiator,” he said. “I negotiated free devices for the information that we were going to give back.” Mathews agreed his program would collect data on Bridge patients and send it to the company. Innovative Health Solutions disputed this characterization, saying in an emailed statement, “It was not a quid pro quo.”

Brian Carrico, now the president of Innovative Health Solutions, worked with Dr. Arturo Taca to adapt the company’s existing nerve stimulator so it could be worn during opioid withdrawal.
Emily Forman/Side Effects Public Media
hide caption
toggle caption
Emily Forman/Side Effects Public Media
Taca helped them implement the protocol later described in the 2017 paper, and Mathews said his group prescribed its first Bridge a month later.
Another provider, Katrina Lock, a nurse practitioner who runs a clinic in Rising Sun, Ind., said she began using the device on patients around Thanksgiving 2015, after she was approached by Tom Carrico, chief regulatory officer for Innovative Health Solutions and Brian Carrico’s father. She said Tom Carrico told her the company was trying to clear FDA hurdles in order to use the Bridge for opioid addiction, and she agreed to do “some testing with the Bridge for him and for the company.”
Taca himself provided much of the data for the research from his clinic, and appeared to be recruiting participants. In April 2016, he posted in a Facebook group that he was conducting a study, and asked people to call his clinic.
Brian Carrico insisted the research was conducted according to FDA regulations and that it wasn’t coordinated in advance. “We as a company cannot give anyone a protocol and we never have,” Carrico said in an interview.
Clinical trials with FDA-regulated devices require oversight from institutional review boards, or IRBs, which protect patients by ensuring the benefits of the research outweigh the risks.
Adrian Miranda, Taca’s co-author, got approval for the study from an IRB at Medical College of Wisconsin, but it was for a retrospective review — not a clinical trial. David Clark, who oversees the IRB at Medical College of Wisconsin, said he did not know that the research was a coordinated effort. “There has to be an IRB review for stuff like this,” said Clark.
Questionable results
An IRB would have evaluated the study’s adherence to FDA rules and ethical standards guiding clinical trials and could have required changes to protect the interests of patients and the validity of the data.
“Most studies of withdrawal are done in residential settings, where people are under pretty continuous monitoring and observation,” said George Bigelow, a professor who heads an IRB at Johns Hopkins University. If patients leave the study site, they may use illicit drugs or over-the-counter medications, skewing the results.
Patients could also relapse and never return, and providers involved with the study told us this was a common occurrence with the Bridge.
Under Taca’s protocol, patients were sent home once after an initial assessment and again after getting the device. The plan then was for patients to come back after five days for a final evaluation and possible Vivitrol treatment. But without monitoring and support, the time spent at home led many patients to drop out of treatment. “There was a fair amount of people that didn’t show up,” Lock said of her patients who were assessed for the Bridge. “And then there was a few people that didn’t show back up to get them taken off.”
Paul Finch, a physician assistant in Fairbanks, Alaska, who gathered data for the study, said he has now used the device dozens of times. He estimated that a little more than half of his Bridge patients successfully complete the detox. “Two-thirds of those will go on to get Vivitrol shots,” he said. “None of it’s perfect.”
In a clinical trial, researchers would normally report how many people completed a study and how many dropped out so it’s possible to better gauge how successful a treatment is. The published study says 73 people were included in the study. Sixty-four people went on to take Vivitrol or naltrexone; the other nine didn’t. However, the researchers didn’t report how many people dropped out, either after their assessment or after receiving the device.
“If you treat 10 people successfully and crow about it, but 90 people dropped out … that’s pivotal,” said Medical College of Wisconsin’s Clark.
Clinical trials also require informed consent from patients to make sure they understand the risks and benefits of participation. But it’s unclear if patients in the Bridge study even knew they were part of an experiment.
The study states that the researchers did not obtain informed consent. At least one provider indicated they told patients they were part of a trial and that the Bridge was not a proven treatment for withdrawals. Another did not.
Autumn Howard, a 30-year-old patient who used the Bridge in Mathews’ program in April 2016, said staff told her the device was experimental, but she couldn’t remember being told she was part of a study because her withdrawals were too intense.
“It was kind of a blur,” Howard said. “I couldn’t read … I don’t even know pretty much a lot of what they said to me when I got there.”
James, the patient at the Union County clinic, also said he didn’t know he was part of a study when he got the Bridge in December. But Mathews indicated he would be sending James’ data to the company. James signed a document just before he got the Bridge, but it was so faded it was difficult to read. Side Effects and NPR obtained a copy of the form, which does not mention a study, or even withdrawals.
The day after he got the Bridge, James shared a photo of himself with the device still behind his ear. But he texted that it stopped working the next day. He started to feel sick again and relapsed.
“I’m on man,” he texted in December. “I haven’t even called the office at all just didn’t go back.”
When we contacted him in April, James said he still hadn’t gone back to get a new device.
“They haven’t tried to contact me or nothing,” he said.
Study under review
IRB oversight might have caught another problem with the study. In 2015, Taca applied for a patent on his treatment method. If approved, Taca could license it to the company and get a slice of the money made from Bridge sales.
Taca didn’t disclose the patent application and the potential financial conflict to the American Journal of Drug and Alcohol Abuse. The IRB at Medical College of Wisconsin never knew about it either, because Miranda left Taca’s name out of the research proposal.
“This is an enormous, astonishing, unbelievable conflict of interest,” said Jake Sherkow, who teaches patent and FDA law at New York Law School. “It casts significant doubt on the results of the study.”
After NPR and Side Effects contacted the journal, it posted a correction noting the possible conflict of interest.
Neither Taca nor Miranda agreed to an interview for this story. Miranda now works as chief medical officer for Innovative Health Solutions.
Experts we consulted found the ethical and regulatory issues in the study troubling. “In an ideal world, the journal would retract the article and the FDA would take the product off the market until an appropriate study was done,” said Diana Zuckerman, president of the National Center for Health Research.
Bryon Adinoff, editor of the American Journal of Drug and Alcohol Abuse, which published the study, said the journal would review the study to decide whether to retract it.
Benefits of legitimacy
Despite the study’s flaws, FDA clearance means the company can now legally market the device for detox, and Carrico is asking insurers to cover it.
The day after the FDA decision, the company reached out to Chambers’ colleague at the Indiana University School of Medicine to inquire about setting up a conversation about the Bridge with a group of addiction treatment providers. The company was following up on an invitation from the medical school extended weeks before. But Innovative Health Solutions representatives had some preconditions.
“What we would not like is any negative energy, non-believers or multiple questions about efficacy,” one wrote to Chambers’ colleague.
Chambers said the message fits a disturbing pattern: The opioid epidemic was fueled by pharmaceutical companies making misleading claims about the risk of addiction with opioid painkillers. Now, Chambers said, Innovative Health Solutions appears to be to ignoring the role of science and overstating its evidence to exploit the addiction treatment market.
“A cult is what comes to mind when I hear ‘nonbelievers,’ ” he said.
He thinks there’s a real risk policy makers and providers may be swayed by the company’s overly enthusiastic marketing.
As far back as 2016, well before the device was cleared for this use, Carrico started talking to Indiana lawmakers about how the Bridge can help with opioid withdrawals. Republican lawmakers even started talking about getting Medicaid to pay for it. “I think it became almost a joke,” said a state official at Indiana’s Family and Social Services Administration. “Every meeting that you attend with a legislator … was all about the Bridge.”
Chambers is worried. “The desperation to treat opioid use disorders is so great that the doors are wide open for non-science to come in to drive practice,” he said.
But Brian Carrico remains a believer. “I’m still looking for the first device that didn’t work. I keep asking and no one can find it,” Carrico said in an interview. “If it was placebo, it’s 100 percent placebo. That’s the best placebo I’ve ever seen.”
This story was produced by Side Effects Public Media, a reporting collaborative focused on public health, in partnership with NPR. You can follow Jake Harper on Twitter: @jkhrpr.
When Inmates Need A Specialist, They Often See The Doctor By Video

Telemedicine is making it easier for inmates to be seen for special medical needs, like cancer or cardiac care.
Heidi de Marco/Kaiser Health News
hide caption
toggle caption
Heidi de Marco/Kaiser Health News
When an inmate needs to see a medical specialist, getting that care can be complicated.
Prisons are often located in rural areas far from medical centers that have experts in cancer, heart and other disease treatments. Even if the visit just involves a trip to a hospital across town, the inmate must be transported under guard, often in shackles.
The whole process is expensive for the correctional facility and time-consuming for the patient.
Given the challenges, it’s no wonder many correctional facilities have embraced telemedicine. They use video conferencing to allow inmates to see medical specialists and psychiatrists without ever leaving the facility.
A survey by the federal Centers for Disease Control and Prevention of prison health care in 2011 found that 30 states out of 45 that responded said they used telemedicine for at least one type of specialty or diagnostic service. The participating states reported that telemedicine was most commonly used for psychiatry (62.2 percent) and cardiology (26.6 percent), according to the research, which was published in 2016.
Among the corrections facilities offering these services is Rikers Island, which houses nine jails on an island near LaGuardia Airport in New York City. It recently began to provide telehealth services for female inmates who need oncology, rheumatology and hematology services. Other specialties are expected to be added in the future.
Male inmates on Rikers have been receiving telehealth services since 2016. Roughly 40 inmates have virtual visits each month with specialists in those same areas as well as infectious disease, urology, dermatology, pulmonology and gastroenterology.
“Initially we implemented [telehealth] for the efficiency part, to avoid hours of transport,” says Dr. Ross MacDonald, chief medical officer for NYC Health + Hospitals/Correctional Health Services, which runs the health care services at Rikers. “But what we’ve learned over time is that it really improves clinical care.” Telehealth allows the referring physician at the jail to consult with the specialist at the hospital as a team, and together clarify information for the patient, MacDonald says.
When the jail’s primary care provider identifies a medical concern that requires a specialist’s attention, the provider will accompany the patient to the jail’s medical clinic and together they’ll consult with a specialist at NYC Health + Hospitals/Elmhurst in Queens who is visible on the monitor. If the patient’s vital signs need to be checked or if she needs other tests, the primary care provider can handle that and communicate results with the specialist.
If after that meeting, a face-to-face exam with the specialist is necessary, that would be scheduled, MacDonald says.
“This is not meant to replace in-person visits, it’s meant to complement them,” he says.
Still, some prisoner advocates worry about the increasing use of telemedicine. Khalil Cumberbatch says he’s concerned that the video visits may heighten inmates’ feelings of isolation. Cumberbatch spent nearly a year on Rikers Island, first as he awaited trial on first-degree robbery charges in the early 2000s and later when he appealed his conviction.
He now works as the associate vice president of policy at the Fortune Society, a nonprofit organization that supports efforts to help prisoners re-enter society after incarceration.
“You’re removing contact with the outside world,” he says. “There’s a level of engagement that can be lost when you’re doing it on the screen.”
But for sick prisoners, that may not be a priority, others say.
“Lots of them don’t want to go to the outside facility,” says Dr. Edward Levine, the medical director for prison care for Ohio State University Wexner Medical Center, which has been doing telemedicine with the Ohio Department of Rehabilitation and Correction since 1995. “These people are sick. They have to get on a bus, it’s bumpy, and there are delays, and if [they’re] not feeling well, they don’t like it.”
Levine estimates he sees up to 150 gastroenterology patients a year at Ohio’s 29 prisons through telemedicine visits. “You develop a relationship with them the same as you would if you saw them in a clinic,” he says.
Although inmates may owe copayments if they see a doctor or nurse for run-of-the-mill aches and pains, they won’t generally have to pay for specialty care, whether provided on-site or through telemedicine, says Dr. Anne Spaulding, an epidemiologist and associate professor at Emory University’s public health school in Atlanta who has worked as a medical director in corrections. That’s because a medical provider typically initiates specialty care. Inmates are more commonly charged for medical visits that they initiate, she says.
Telemedicine can improve continuity of care and help patients keep chronic conditions under control. In one study of HIV-infected adults incarcerated at Illinois Department of Corrections facilities, 91 percent of telemedicine patients achieved complete suppression of the virus during the first six visits, compared with 59 percent of patients who received standard care on-site at the facilities. The study credited the results to having specialists provide evidence-based, up-to-date care through telemedicine, rather than relying on primary care physicians at the correctional facilities.
“If we can see them in real time without having to leave the facility, we get better outcomes,” says Dr. Jeremy Young, an infectious-disease specialist and associate professor of medicine at the University of Illinois at Chicago, who was the lead author of the study.
Kaiser Health Newsis a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation which is not affiliated with Kaiser Permanente.Follow Michelle Andrews on Twitter: @mandrews110.
'Failing Patients': Baltimore Video Highlights Crisis Of Emergency Psychiatric Care

Cheryl Chandler says she happened to click on a viral video showing a woman wearing a hospital gown, not knowing it showed her 22-year-old daughter, Rebecca. She has mental health issues and was left outside a Baltimore hospital on a cold January night. The video recorded by a passer-by went viral.
Jared Soares for NPR
hide caption
toggle caption
Jared Soares for NPR
A viral video from Baltimore is drawing attention to a crisis that’s unfolding in emergency rooms across the country: Surging numbers of patients with psychiatric conditions aren’t receiving the care they need.
On a cold night in January, a man walking by a downtown Baltimore hospital saw something that shocked him. He started recordingthe incident on his phone.
Imamu Baraka’s video, which has been viewed more than 3 million times, shows security guards walking away from a bus stop next to the emergency room of University of Maryland Medical Center Midtown Campus.
One is pushing an empty wheelchair. The woman they left there is wearing a thin yellow hospital gown and socks.
“Wait, so you’re just going to leave this lady out here with no clothes on?” Baraka asks the guards. They continue walking away.
The woman, later identified as a 22-year-old named Rebecca, staggers near the bus stop. She appears distressed and confused. She moans and shouts.
“Are you OK, ma’am? Do you need me to call the police?” Baraka asks.
Nationwide, hospitals are struggling to provide services to people with psychiatric emergencies. Between 2006 and 2013, ER visits increased by more than 50 percentfor psychoses and bipolar disorders and depression, anxiety and stress reactions according to the Healthcare Cost and Utilization Project, which compiles health care data. Between those years the number of visits climbed from 3,448 visits to 5,330 per 100,000 U.S. patients ages 15 and older.
“We’re just failing patients with mental illness and it’s just getting worse as time goes on,” says Dr. John Rogers, president-elect of the American College of Emergency Physicians.

Imamu Baraka, the man who came to the aid of a woman discharged from a hospital wearing only a gown and socks on a cold winter’s night, stands outside the University of Maryland Medical Center Midtown Campus in Baltimore. He recorded the events on cellphone video, fearing no one would believe him if he reported a woman being left at a bus stop.
David McFadden/AP
hide caption
toggle caption
David McFadden/AP
In the viral video, Rebecca has a visible wound on her forehead, and her breath forms white clouds in the cold. Baraka calls for an ambulance, which brings her back to the hospital that just discharged her.
Rebecca’s mother, Cheryl Chandler, says she happened to click on the video, not knowing it showed her daughter. “Once he focused on her face I realized it was her. And I think I went into shock initially,” Chandler says.
That realizationset off a desperate search. The hospital wouldn’t tell her where she was. Chandler called the police. They found out that the hospital didn’t readmit Rebecca, even though according to a federal regulator’s report, Rebecca told workers in the ambulance, “I do not feel normal, and do not know what normal is.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A screenshot shows Rebecca outside University of Maryland Medical Center Midtown Campus hospital in Baltimore in January.
Imamu Baraka/Reuters
hide caption
toggle caption
Imamu Baraka/Reuters
Hospital staff put her into a cab that took her to a nearby homeless shelter, where family members found her the next day. She’s been hospitalized on and off since the incident.
“She could have got hypothermia. She could have died. She could have been raped, she could have been killed,” Chandler says. “All she wanted was treatment and they had two opportunities to do it and denied it both times.”
Rebecca was clearly asking for medical care, her mother says, which ERs are legally required to provide.
“That, what I saw in the video, was my worst nightmare for Rebecca,” Chandler says. Several years ago, Rebecca was diagnosed with bipolar and schizoaffective disorders. Her mom adds that she’s a shy and lovable introvert who loves animals and making art.
Rebecca has insurance and had been in a residential home when she went missing, Chandler says.
The hospital has apologized and says it has already put in place measures to correct the issues.
Chandler says she hopes that means it won’t happen to other patients. But she adds that Rebecca will continue to suffer from the hospital’s decisions: “No part of Rebecca, because of this, is going to heal. No part. We can’t make the scars go away.”

Rebecca has been diagnosed with bipolar and schizoaffective disorders. Her mom says she’s a shy and lovable introvert who enjoys animals and making art.
Courtesy of Cheryl Chandler
hide caption
toggle caption
Courtesy of Cheryl Chandler
James E. Farmer, a lawyer for Rebecca’s family, says they’re investigating now and considering filing lawsuits. “It’s going to be difficult to determine the exact extent of harm to Rebecca,” he says. “I could not imagine the psychological damage and harm that was done as a result of this.”
The Centers for Medicare & Medicaid Services says the hospital failed to discharge the patient safely, among other breaches.
According to the federal regulator’s report, Rebecca was “resistant to discharge and refused to get dressed into street clothes when requested by nursing.” The hospital stated there was a “communication failure” which led to her discharge into the cold weather, though the report says it is not clear whether nursing or security staff made that decision.
Chandler says she’s heard from other families with similar stories: “The only difference is it wasn’t caught on video.“
“They told me to leave”
Here’s another story from Baltimore, about Laura Pogliano and her son Zaccaria. Zac, who had schizophrenia, died in 2015 of heart failure when he was 23.
Zac was sensitive and empathetic, and loved playing the piano, his mother says. He started to show symptoms of the disease when he was 16. He became paranoid, and started doing things like hiding kitchen implements out of fear that someone was trying to kill his family.

Laura Pogliano holds a photo of her son Zaccaria, who was diagnosed with schizophrenia. As part of his illness, Zac started to think that he had dramatic injuries. He made frequent trips to the emergency room but hospital staff would call her to pick him up.
Eslah Attar/NPR
hide caption
toggle caption
Eslah Attar/NPR
“His personality just drastically changed,” Pogliano says. “He had a thousand rituals around things so that he wasn’t harmed.”
Then, as part of his illness, Zac started to think that he actually did have dramatic injuries. Like a gunshot wound or a pulverized ankle. He’d call 911.
“He got to the point where he would pick up the phone at the drop of a hat and say, can someone come and help me, I’m having a heart attack,” Pogliano says.
This happened about 20 times in the two years before his death, she says. Often, ambulances took Zac to Good Samaritan Hospital, where Pogliano says the doctors would typically call her to let her know he arrived and would provide appropriate care for him. Later, hospital staff would call her to pick him up.
But one night after Zac went to the ER, Pogliano woke up hours later and got worried that she hadn’t received a call.
“I just got in the car and drove over there, and he was sitting outside. It was early spring but it was still wintery, probably 40 degrees out, 45 degrees out,” she says.

A framed photo of Laura Pogliano’s son Zaccaria. He died in 2015 of heart failure when he was 23. About a year before he died, Laura drove to the hospital to check on Zac, and she found him sitting outside in 40 degree weather in shorts, a hospital gown and no shoes. “They told me to leave,” he told his mom.
Eslah Attar/NPR
hide caption
toggle caption
Eslah Attar/NPR
“All he had on was what he wore to the hospital, which was a pair of white linen shorts. I know he didn’t have shoes on. … And a hospital gown and no shirt. I said to him, ‘Oh my gosh, what are you doing here?’ He said, ‘They told me to leave.’ “
A hospital spokeswoman acknowledged that Pogliano was a patient there but says she found no indication that he was ever inappropriately evaluated or mistreated. She says she couldn’t comment further because of federal privacy laws.
Emergency room doctors are frustrated at the growing gap in care for patients with psychiatric disabilities.
“We’re kind of tired of waiting for legislators and regulators to act and to meet their responsibility to these patients in the form of providing funding for resources,” says Rogers, the president-elect of the American College of Emergency Physicians.
Even as there is increasing demand, there are fewer resources to care for psychiatric patients. It can be difficult for doctors to find an inpatient bed — the numbers are have decreased dramatically over the decades. Rogers says there have been significant cuts to community and outpatient resources — so the emergency department is often the only place for psychiatric patients to go.
“Every emergency physician in the country knows this problem well and wants to do something about it,” Rogers says.
Often the ER is not properly equipped with staff that can offer treatment to psychiatric patients. The emergency room’s mission is to assess and stabilize, but the actual care they can provide psychiatric patients is fairly limited. A 2008 survey of ER doctors found that 62 percent of them said there were no psychiatric services provided while the patients were in the ER.

Cheryl Chandler says she’s heard from other families with stories like her daughter’s. “The only difference is it wasn’t caught on video,” Chandler says.
Jared Soares for NPR
hide caption
toggle caption
Jared Soares for NPR
“And the disparity between our ability to care for a patient with a medical problem and a patient with a psychiatric problem is growing, that gap is increasing,” Rogers says.
He says Rebecca’s case is an outlier. More common, he says, is that ERs will hold patients for too long before they can transfer them somewhere that can treat them. In a recent poll of emergency physicians, 84 percent said that psychiatric patients are “boarded” in their departments for hours or days. Rogers says he’s heard of patients being held for weeks.
And the options for where to transfer them are often limited. “And that’s where it starts breaking down,” he says. “The time that it takes to get someone transferred for something like that is just unacceptable….They wait, and wait, and wait.”
It’s a bad situation for everyone – for patients with psychiatric disabilities, and for other patients who have lengthy wait times because ERs are overwhelmed.
“They’re being asked to do way too much with way too few resources,” says Susan Stefan, a lawyer focusing on rights of people with psychiatric disabilities. ERs “have a specific mission, which is to provide emergency medical care, and they’re being turned into essentially 24-7 social service agencies.”
Stefan, who wrote a book about treating psychiatric patients in ERs, says it’s common for them to transfer people to homeless shelters because they are not equipped to find people stable housing.
And there’s another crucial point here: The ER is simply a bad place to treat severe mental illness, even as it is becoming increasingly central for those patients.

A video showing a patient wearing a hospital gown being dropped off at a bus stop near University of Maryland Medical Center Midtown Campus in downtown Baltimore this January went viral.
Emily Bogle/NPR
hide caption
toggle caption
Emily Bogle/NPR
“The emergency department is probably the worst place for somebody in psychiatric crisis,” Stefan says. “It’s loud, it’s chaotic and people don’t take a lot of time because they don’t have a lot of time.”
And it’s not straightforward to transform an ER into a place that is appropriate to provide treatment to people who are in the middle of psychiatric crises — although there are hospitals that are experimenting with new models to better serve these patients.
The Alameda Health System in Alameda County, Calif., is a model that both Stefan and Rogers point to. There, a doctor named Scott Zeller has set up a dedicated psychiatric emergency service — a department separate from the standard emergency room that can provide specialized evaluation and treatment for these patients.
The Alameda model reduced boarding times by 80 percent, according to a study published in the Western Journal of Emergency Medicine, and the fast, stabilizing treatment made it far less likely that the patient would need to be transferred to an inpatient bed.
If there were adequate services in place, most of the people coming to ERs for psychiatric crises wouldn’t need to come there at all, says Jennifer Mathis, the director of policy and legal advocacy at the Bazelon Center for Mental Health Law.
“And much as everybody loves to talk about the need for mental health services, that doesn’t translate into state policy and funding for community mental health services,” she says.
The problem here, Mathis says, is political will. There’s a big gap between politicians talking about mental health and actually making sure people are getting the services they need.
After Push From Activists, Chicago's South Side Gets An Adult Trauma Center

{kind=link}
The Level 1 adult trauma center will officially launch on May 1.
Rob Hart/Courtesy of University of Chicago Medicine
hide caption
toggle caption
In 2010, 18-year-old Damian Turner was shot in the South Side of Chicago, just a few blocks away from the world-class University of Chicago hospital. But the ambulance that arrived to help him couldn’t take him there, because the hospital didn’t have an Level 1 adult trauma center.
Instead, it drove the gravely injured Turner nine miles to Northwestern University hospital, where he died from his wounds.
Turner’s death mobilized South Side young black activists. For years, they demanded that the University of Chicago reopen an adult trauma center that had closed in 1988 after losing millions of dollars each year treating patients without health insurance.
After years of resistance, the university is reopening its adult trauma center on May 1 — a decision that will provide the South Side with more accessible trauma care.
“There are a lot of trauma-related deaths because gun violence is such a prevalent issue on the South Side. It was then it is now. It has been for decades,” said activist Veronica Morris-Moore.“A lack of a trauma center was a severe indication of the institutional racism that existed on the South Side. And the reason it was worth our time as young people was because we were losing friends.”

Veronica Morris-Moore stands outside the adult emergency room at the University of Chicago Medical Center in Feb. 2013. Morris-Moore was one of many activists pressuring the medical center to reopen an adult trauma center it closed in the 1980s.
Charles Rex Arbogast/AP
hide caption
toggle caption
Charles Rex Arbogast/AP
Research backs Morris-Moore up: If you are shot more than five miles from a trauma center in Chicago, your likelihood of dying is 21 percent greater.
The university’s effort to reopen the center received a boost in 2015 when it made a bid for the Obama Presidential Center. That year, in an about face, the university said it would again open a trauma center.
Trauma care is costly complex web of care treatment lots of specially trained surgeons and nurses who treat penetrating wounds — from car crashes, stabbings to serious falls to gunshots. New staff have been hired, a new emergency room in the hospital opened in December and the state public health department approved trauma care earlier this month.
The new center’s head, Dr. Selwyn Rogers, said he will also work with local groups on social services centered around violence in addition to providing care.
“We bring together the resources of the university, medical center and community partners so that we can be better able to address health disparities and the public health epidemic of intentional violence,” Rogers said.
One of those community partners is Julian DeShazier, the pastor of University Church, which is not affiliated with the university. Activists used this church as a meeting space when they were planning strategy.
“Once we got on board it took on another dimension. We began to talk about it from different angles in terms of faith, and use our resources and access to try to help their voices be heard more,” DeShazier said. “We were able to help mediate conversations between medical center executives and the organizers on the ground doing that work. That’s the kind of work churches can do when they’re really rooted inside of a community.”
The hospital estimates the trauma care will cost $48 million a year. While trauma injuries are unpredictable, officials say the new trauma unit could treat up to 4,000 patients yearly starting next Tuesday.