Shingles Is Nasty, And The New Vaccine Works Well. Why Do Adults Avoid Shots?

Cost, procrastination and a lack of insurance coverage are just a few of the reasons adults give health care providers for not getting vaccinated against shingles and other illnesses.
Andrew Brookes/Getty Images/Cultura RF
hide caption
toggle caption
Andrew Brookes/Getty Images/Cultura RF
Federal officials have recommended a vaccine against shingles that is more effective than an earlier version at protecting older adults from the painful rash. But persuading many adults to get this and other recommended shots continues to be an uphill battle, health providers say.
” ‘I’m healthy; I’ll get that when I’m older,’ ” is what adult patients often tell Dr. Michael Munger when he brings up an annual flu shot or a tetanus-diphtheria booster or the new shingles vaccine. Sometimes, he says, they put him off by questioning a vaccine’s effectiveness.
Munger, a family physician in Overland Park, Kan., who is president of the American Academy of Family Physicians, says he gets more pushback from adults about getting their own vaccines than about immunizing their children.
“As parents, we want to make sure our kids are protected. But as adults, we act as if we’re invincible.”
The new schedule for adult vaccines for people age 19 and older has been updated in the last several months by the federal Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices. The most significant change was to recommend Shingrix, the shingles vaccine that was approved by the Food and Drug Administration last fall, over an older version of the vaccine.
Shingrix should be given in two doses between two and six months apart to adults who are at least 50 years old, the CDC says. The older vaccine, Zostavax, can still be given to adults who are 60 or older, but Shingrix is preferred, according to the agency.
In clinical trials, Shingrix was 96.6 percent effective in adults ages 50 to 59, while Zostavax was 70 percent effective. The differences were even more striking in older age groups: Effectiveness in adults 70 and older was 91.3 percent for Shingrix, compared with 38 percent for Zostavax.
Shingrix also provided longer-lasting protection than Zostavax; the older vaccine’s effectiveness waned after the first year.
The CDC’s guidelines suggest that people who have already had the Zostavax shot be revaccinated with Shingrix.
The two-shot series of Shingrix costs about $280, while Zostavax runs $213.
“What’s remarkable [about the new vaccine] is that the high level of immunity persists even in the very old,” says Dr. Anne Louise Oaklander, a neurologist at Harvard and Massachusetts General Hospital who studies the complications that can arise with shingles.
Shingles is caused by the same varicella-zoster virus that causes chickenpox. The virus can re-emerge decades after a recovery from chickenpox, often causing a painful rash that may burn or itch for weeks before it subsides.
About 1 in 3 Americans will get shingles during their lifetime, according to the Centers for Disease Control and Prevention; there are roughly 1 million cases every year. People are more likely to develop shingles as they age, as well as develop complications like postherpetic neuralgia, which can cause severe, long-standing pain after the shingles rash has disappeared. In rare cases, shingles can lead to blindness, hearing loss or death.
Although shingles vaccination rates have inched upward in recent years, only a third of adults who were 60 or older in 2016 had received the Zostavax vaccine, the CDC says.
Many adults seem to skipping other recommended vaccines, too. Typically, about 45 percent get the annual flu shot, and only 23 percent of those the CDC says should get the pneumococcal and tetanus-diphtheria-pertussis vaccines are up-to-date with those immunizations.
In contrast, by the time children are 3 years old, typically more than 80 percent (and more than 90 percent, in the case of some vaccines) have received recommended immunizations.
Why the discrepancy between kids and grown-ups? Cost can be a big deterrent for adults who are considering some vaccinations. The federal Vaccines for Children program helps parents whose kids are eligible for Medicaid or are uninsured cover the cost of vaccines up to age 19.
Adults with private insurance who get vaccines recommended by the CDC are sheltered from high costs because (under the Affordable Care Act) the shots must be covered by most commercial plans without charging consumers anything out-of-pocket.
Still, patients, should confirm their coverage before requesting the new shingles vaccine, health care providers say; insurers typically add new vaccines gradually to their formularies after they have been added to the recommended list. So some consumers may need to wait a little while before their insurer covers Shingrix.
Vaccine coverage under the Medicare program for people age 65 and older tends to be much less comprehensive. Vaccines to prevent influenza and pneumonia are covered without a copayment under Medicare Part B, which covers outpatient care, while other vaccines — including the shingles vaccine — are typically covered under Part D drug plans. And those Part D plans may leave some beneficiaries on the hook for all or part of the cost of the two-shot series.
That can pose a significant problem for patients.
“Not every Medicare beneficiary elects Part D, and even if you do, some have deductibles and copayments,” says Dr. William Schaffner, an infectious-diseases specialist at Vanderbilt University School of Medicine.
And even if adults want to get their recommended shots, some lose track of which they have already received and when. Pediatricians routinely report the vaccines they provide to state or city vaccination registries that electronically collect and consolidate the information. But the registries are not widely used for adults, who are more likely to get vaccines at various locations, such as a pharmacy or at work, for example.
“I’m always asking patients, ‘Did you get all the doses in the series?’ ‘Where did you get them?’ ” says Dr. Laura Riley, vice chair of obstetrics at Boston’s Mass General Hospital, and a member of the CDC’s Advisory Committee on Immunization Practices. “It can be very challenging to track.”
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Michelle Andrews is on Twitter @mandrews110.
President Trump Unveils Plan To Fight Opioid Crisis

An estimated 64,000 people died from drug overdoses in the United States in 2016 — the vast majority of those were from heroin or synthetic opioids. New Hampshire is one of the states hardest hit by the epidemic and on Monday President Trump unveiled his plan to fight the crisis.
Black And Latino Children Are Often Overlooked When It Comes To Autism

Shannon Wright for NPR
Sherry Alvarez says she knew there was something different about her son since he was about 9 months old. Back then Sherry says his pediatrician told her there was nothing to worry about, ” ‘Boys are a little slower than girls, so let’s just wait until his second birthday.’ ” We aren’t using Sherry’s son’s name to protect his privacy.
By her son’s second birthday, Sherry says she was getting desperate. She didn’t know why he wasn’t talking yet or showing affection like other kids. At 2 1/2, he was referred to Children’s Hospital Los Angeles.
There, after four hours of tests, Sherry says the doctor handed her a 20-page report explaining his autism spectrum disorder diagnosis, among others. She says she was paralyzed by emotion.
ASD is a disease that affects people of all races and ethnicities, but research shows that African-American and Latino children with autism are diagnosed at older ages than white children, giving them less of an opportunity for proper intervention and treatment.
This is especially true of minimally verbal kids like Sherry’s son and there are many possible reasons for a late diagnosis. Some families face healthcare access issues and prohibitive costs for treatment, and some families just don’t know how important it is to get diagnosed to move on to the treatment phase. The dialog between doctors and minority families during the diagnosis process is critical.
A recent study from Georgia State University found that African-American parents reported fewer concerns about behaviors like delayed speech and repetitive behaviors, even though their children showed a greater severity with these symptoms, overall. But, of course, it isn’t all up to parents.
“There are very likely parent aspects of this and very likely clinician aspects of this,” says Meghan Rose Donohue, a lead researcher on the study. Perhaps families, like Sherry’s, don’t have the information necessary to really push physicians, but it is also possible that doctors don’t take these cases seriously enough from the beginning.
Families and doctors, alike, can mistake ASD for simple bad behavior, especially in boys, as research has shown over the past couple of decades. A 2001 study at McGill University in Montreal found that doctors were more hesitant to diagnose ASD in minority families.
In 2007, a study by a team at the Center for Autism and Developmental Disabilities Research and Epidemiology, University of Pennsylvania, found that African-American children were 5.1 times more likely to be misdiagnosed with conduct disorders before being diagnosed with ASD.
When Sherry was growing up, she had a cousin who the family thought of as “different,” she says. “He was basically hidden. We didn’t talk about it as a community.” He had autism. “We have to retrain ourselves. It’s not OK to hide our kids.”
Regional Centers in Los Angeles, which offer services to the developmentally disabled, are now starting to look at the diagnosis disparity problem. Westside Regional Center in Culver City just received a grant from the state to look at how autism diagnosis disparities manifest within their intake and treatment programs.
“We’ve implemented a series of trainings with intake counselors on cultural awareness and sensitivity, and we’re starting to have a lot of conversations about biases,” says Tom Kelly, Westside’s chief psychologist.
One of the apparent biases among intake counselors at the center stems from the difference in the documentation that arrives with each new child. African-American families tend to arrive at the center with lots of documentation detailing behavior issues from their child’s school or social services. With all those official papers sitting in front of them, it’s much easier for a counselor to think “behavior disease” rather than “autism,” says Kelly.
And that disparity exists in dollars spent, as well. As reported in a 2017 survey, South Central Regional Center spends $8,000 less per client than the Westside location and the racial disparity persists statewide.
But there are more resources for minority families today than compared to when Sherry’s son was young. The Autism Society of Los Angeles runs a hotline to help parents navigate the diagnosis and healthcare landscape and Children’s Hospital Los Angeles now employs liaisons to help families connect with the right resources. But, the spending gap persists.
Today, Sherry says her now 15-year-old son is happy. He attends Hamilton High School and communicates almost solely through a typing device. “This is the time in his life where those early treatments could have made a difference,” she laments.
More Than A Job: Home Care For A Mom With Alzheimer's Disease

Celina Raddatz and her mother, Guadalupe Pena Villegas, at home in California.
Xavier Vasquez/NPR
hide caption
toggle caption
Xavier Vasquez/NPR
Celina Raddatz quit her job at a nursing home in 2014 when she realized she would have to take care of her mother full-time. Raddatz’s mother, Guadalupe Pena Villegas, 83, suffers from Alzheimer’s and bipolar disorder, a combination that sometimes makes her a danger to herself and others, and thus requires her to be supervised 24 hours a day.
Raddatz and one of her sisters, Rosalia Lizarraga, 61, had been caring for their mother together. But as the Alzheimer’s progressed, the task became too stressful for Lizarraga. The full responsibility fell on Raddatz, who was determined to fulfill a promise she and her siblings had made their mother as children.
“When my mother was sane, she made us promise never to put her in a nursing home. And of course, us young kids said, ‘OK, mom we would never …’ ” Raddatz says. “But we never ever once ever thought that she would get sick like this.”
As the elderly population in the United States grows, an increasing number of people require extra help in their daily lives. Because of this, the Bureau of Labor Statistics predicts employment for home health aides will grow 40% between 2016 and 2026. Hiring private caregivers, however, can be a financial burden for some families who can’t afford to pay an average of $22,170 a year for extra help.
Many families take on the responsibility of caring for their aging relatives. In some cases, like Raddatz’s, it can leave little time for other employment. Luckily, there are federally and state-funded programs across the country that allow elderly individuals like Raddatz’s mother to use Medicaid funds to hire their own personal caregivers – including family members.
“We noticed that she was not right”
Raddatz, 57, was born in Mexico. Her mother, a widow, supported nine children as a food vendor. When Raddatz was 8 years-old, her mother married a U.S. soldier, who immigrated the entire family to the United States, where the couple had two more children.
Raddatz’s mother and stepfather divorced two years after moving to the U.S. in 1971 and the family relocated Los Angeles.
“My mom was a very strong woman,” Raddatz says. Due to gang activity in their east L.A. neighborhood, when Raddatz was growing up, her mother quit her job and began collecting welfare so she could stay home and keep an eye on her children.
“She would take us to school and bring us home. She would not let us walk alone to school.”
Raddatz and her siblings first began to notice their mother changing in 2005 after she had a bad fall while working as a housekeeper.
“She kept telling this story that she fell at work and her head fell in her lap and she picked it up and put it back on her shoulders,” Raddatz says. “We kept telling her, ‘Mom, that’s impossible’ and she would get upset. And that’s when we noticed that she was not right.”
In 2006, Raddatz’s mother was diagnosed with Alzheimer’s disease.
“It’s just constant, constant, work”
At the time, Raddatz was working as an activity director at a nursing home in La Mesa, Calif. Her job was to make sure the residents remained engaged with their community through special outings and social events. “You get close to these people after working there for so many years and we felt like a family. Definitely,” Raddatz says.
It’s a field in which she’d spent more than 30 years working across California, having started out as certified nursing assistant. And she noted, her inspiration to pursue a career caring for the elderly came from tending to her grandmother as a teenager.
So when it became clear that her mother could no longer live by herself, Raddatz’s siblings turned to her as the most qualified to look after the elderly matriarch. Raddatz knew, however, there was a distinction between providing care professionally at a facility and caring for an elderly relative at home.
“It’s a lot easier doing it at work because you get a break,” Raddatz says. “And when you go home and you work taking care of your own parent, you don’t get a break. It’s 24/7, nonstop. It’s just constant, constant, work.”
But nonetheless, she quit her job at the nursing home and moved her mother in with her.
Shortly after leaving her job, Raddatz lost her apartment in El Cahon, Calif. and moved into her sisters’ home in Riverside. She cares for her mother around the clock, preparing her meals, helping her bathe and dress, and keeping her calm and entertained during the day. They also share a bedroom, so Raddatz can assist her mother when she wakes up throughout the night.
“Cash and Counsel” program
For about a year Raddatz cared for her mother without an income until one day in December, 2015, a social worker friend of hers recommended a government program called In-Home Supportive Services (IHSS). IHSS is what is called a “Cash and Counsel” program, which allows disabled and elderly individuals to use federal and state funds to hire their own help as they need it. These caregivers help their employers with anything from getting dressed to cooking meals to making sure they take their medication. Caregivers can be anyone the employer chooses (as long as the person passes a background check), including friends and family.
“I was very excited,” Raddatz says. “I was happy to hear that the government had such a program because we were in so much need.”
Raddatz registered her mother with IHSS and completed her background check. But when a social worker came to their home to evaluate her mother’s level of need, she was only granted 44 hours a month to hire a caregiver for an hourly wage of $10.50.
Programs like IHSS use evaluations to determine how much time a day an individual requires assistance and with what tasks. For the evaluation process, a social worker from San Diego County came to Raddatz’s home and did a physical and mental assessment of her mother. Because her mother is able-bodied and was able to respond to the simple interview questions the social worker asked, it was determined she needed less extensive care.
Raddatz was taken aback by how few hours her mother had been approved for, based on the amount of care she provided her mother every day. She felt the interview portion of her mother’s assessment hadn’t been thorough enough to accurately gauge her mother’s need for care. The social worker only asked two or three simple questions during the interview, to which Raddatz’s mother’s responses didn’t demonstrate the full extent of her dementia.
Caring for her mother “until the very end”
Raddatz had learned about a home care providers’ union, UDW, during her registration with IHSS and reached out to them out to see if they could help. With UDW, Raddatz began the process of appealing the number of hours her mother was given. But even with the lack of paid hours, Raddatz says she is determined to care for her mother until the very end because “it’s more than a job.”
“It’s a family responsibility because of the promises we made her when she was younger,” Raddatz says.
After her mother passes, Raddatz says she intends to return to her old job and when she does, it will be with a greater understanding of the families she serves. It used to pain Raddatz to see families leave their relatives with dementia in a nursing home. Now, she says, she has a personal appreciation for the emotional and physical sacrifices that caring for an elderly loved one involves.
“I can relate more to these families and my heart goes out to them,” says Raddatz says. “Even more so now than before.”
After Raddatz was interviewed for this story, San Diego County conducted another evaluation of her mother’s needs. In November, it was determined her mom was eligible for the maximum number of hours allowed through IHSS, which is 283 hours a month — approximately 70 hours a week. Additionally, Raddatz is paid overtime for every hour she works past 40 a week, is receiving back-pay for hours worked since June, 2017 and was given a small raise at the beginning of the year.
Raddatz says even though her hourly rate is lower than her old job, she is now making more than she did as a nursing home activity director. With the recent improvements to their standard and quality of life, Raddatz and her mother hope to move out of her sister’s house soon and into their own home.
NPR’s Alexi Horowitz Ghazi contributed to this report.
Landmark Report Concludes Abortion In U.S. Is Safe

A report from the National Academies of Sciences, Engineering, and Medicine says that abortion is safe but that “abortion specific regulations in many states create barriers to safe and effective care.”
Bryce Duffy/Getty Images
hide caption
toggle caption
Bryce Duffy/Getty Images
Abortions in the United States are safe and have few complications, according to a landmark new study by the National Academies of Sciences, Engineering and Medicine.
The report, called “The Safety and Quality of Abortion Care in the United States,” examined the four major methods used for abortions — medication, aspiration, dilation and evacuation, and induction — and examined women’s care from before they had the procedure through their follow-up care.
“I would say the main takeaway is that abortions that are provided in the United States are safe and effective,” says Ned Calonge, the co-chair of the committee that wrote the study. He is an associate professor of family medicine and epidemiology at the University of Colorado and CEO of The Colorado Trust.
Calonge says the researchers found that about 90 percent of all abortions happen in the first 12 weeks of pregnancy. And complications for all abortions are “rare,” the report says.
But the report did find that state laws and regulations can interfere with safe abortions.
“Abortion-specific regulations in many states create barriers to safe and effective care,” the report says.
Calonge says those rules often have no basis in medical research.

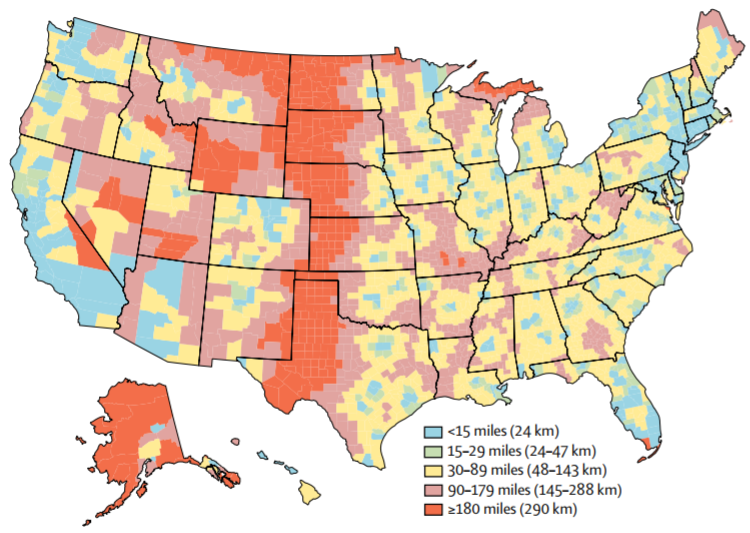
Analysis is limited to facilities that had caseloads of 400 abortions or more per year and those affiliated with Planned Parenthood that performed at least one abortion in the period of analysis.
Credit: National Academies of Sciences; Source: Bearak et al., 2017
hide caption
toggle caption
Credit: National Academies of Sciences; Source: Bearak et al., 2017
“There are some requirements that require clinicians to misinform women of the health risks, that say you have to inform a woman that an abortion will increase her risk of breast cancer,” he says.
There is no evidence that breast cancer follows abortion, for example, but five states require doctors to tell women there is a link, according to the Guttmacher Institute, a research group that focuses on reproductive and sexual health.
“There are policies that mandate clinically unnecessary services like pre-abortion ultrasounds, separate inpatient counseling. There are required waiting periods,” Calonge says.
According to Guttmacher, 27 states make women wait at least 24 hours for an abortion and 11 states require women to have an ultrasound before they can terminate their pregnancy.
And there are state laws that dictate who can perform abortions and where they can do them. Some require all abortions to happen in the equivalent of a hospital or surgery center. Others require a doctor to have admitting privileges at a nearby hospital.
The National Academies report says waiting periods and requirements for unnecessary tests can result in long delays because women may have to travel to get care and have trouble getting appointments.
“Delays put the patient at greater risk of an adverse event,” the report says.
Hal Lawrence, the CEO of the American College of Obstetricians and Gynecologists, says the report settles the debate over abortion-restricting laws and regulations.
“Those sorts of laws have been totally debunked,” he says.
He says the study shows most of those laws do nothing to improve women’s health.
“Abortion is safer when it’s performed earlier in gestation,” Lawrence says. “And so delaying and making people wait and go through hoops of unnecessary, extra procedures does not improve the safety. And actually by having them delay can actually worsen the safety.”
The U.S. Supreme Court in 2016 voided some state abortion laws when it ruled that Texas’ strict rules around abortion facilities impose an undue burden on women. But other laws remain in place even without any backing in medical research.
Still, Donna Harrison says there are good reasons for the requirements.
“The tendency to look at abortion as though it were not a serious medical procedure is irresponsible. I mean, we all know that the fetus is killed during an abortion but women can be harmed by irresponsible medical care,” says Harrison, the executive director of the American Association of Pro-Life Obstetricians and Gynecologists.
She says data on complications from abortion is incomplete because doctors and patients don’t always report it accurately, or at all.
“There is no good data collection — and when you have garbage in, and you have garbage out,” she says.
And she says waiting periods are important so that women can give fully informed consent before they undergo what she says is a sometimes dangerous, surgical procedure.
The new report — which runs more than 200 pages — addresses most aspects of abortion care, including the use of the abortion pill mifepristone.
For example, it concludes that the strict requirements on how doctors can administer mifepristone may need review. The researchers say the rules may be erecting unnecessary barriers.
The report also says nurse practitioners and physician assistants can perform abortions just as safely as physicians.
Also, abortions have no long-term consequences on women’s physical and mental health, the report says.
Financial Side Effects From A Prescription For Toenail Fungus

When Anne Soloviev, a retiree who lives in Washington, D.C., received a prescription to treat toenail fungus, she never thought to ask how much the medicine cost.
Cheryl Diaz Meyer for KHN
hide caption
toggle caption
Cheryl Diaz Meyer for KHN
When Anne Soloviev went to Braun Dermatology and Skin Cancer Center in Washington, D.C., for her semiannual dermatology checkup in early January, the physician assistant diagnosed fungus in two of her toenails.
Soloviev hadn’t complained about her toenails or even noticed a problem.
But the P.A. offered a solution anyway. She called in a prescription for an antifungal medicine to a specialty pharmacy with mail-order services that would send it to Soloviev’s Capitol Hill home.
It seemed like an easy fix to an inconsequential health issue. “I did not ask how much it cost – it never crossed my mind, ever,” said Soloviev, a former French teacher, who still works part time.
Then the bill came.
Patient: Anne Soloviev, 76, of Washington, D.C.
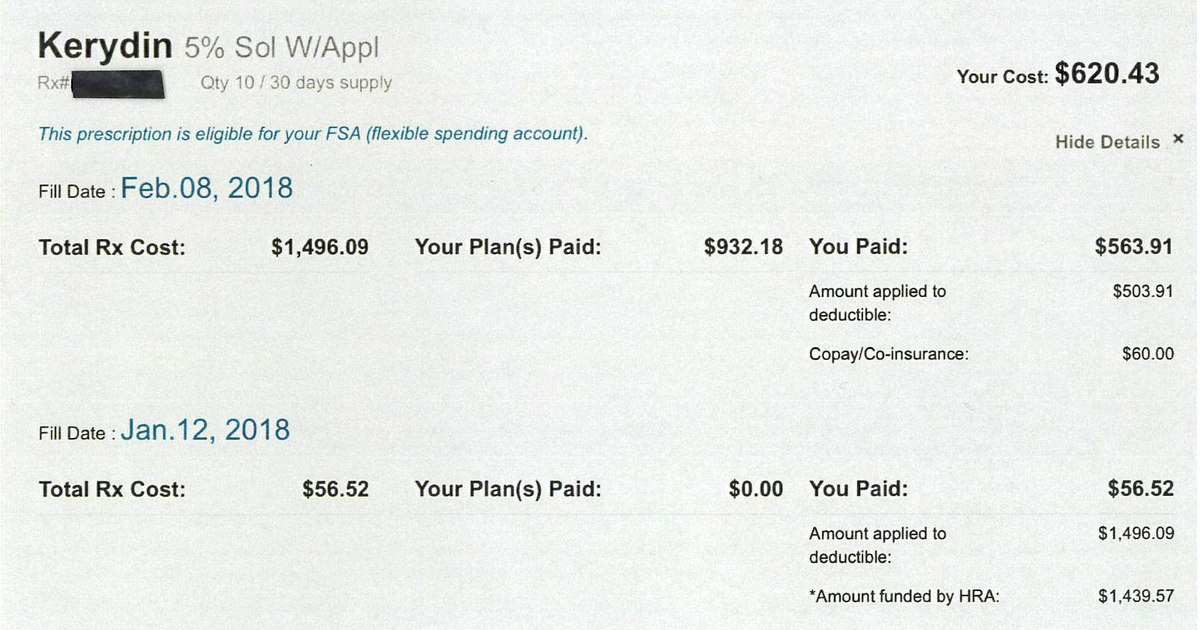
The bill: $1,496.09 for Kerydin, a topical medication that treats toenail fungus. Originally produced by Anacor Pharmacueticals, Inc., the drug is now a product of Sandoz, a division of Novartis.
Service provider: My Express Care Pharmacy, plus Braun Dermatology and Skin Cancer Center
Medical treatment: The antifungal medicine arrived by overnight mail, and an automatic refill came a few weeks later. She began using it on the two toenails, as directed, having been told it would take about 11 months to treat her feet.
She thought little of it.
Soloviev, a widow, has robust insurance. She is covered by Medicare, parts A and B, and has supplemental insurance through her late husband’s government health benefits that covers prescription drugs. She also has a health reimbursement account, which receives almost $1,500 pre-tax each year to pay for uncovered medical expenses. She typically uses the HRA money to cover copays for the other medicines she takes regularly.
But when Soloviev went to her local CVS to pick up another medication – a cholesterol-lowering statin that is usually paid for by her HRA – she discovered her reserve was empty.
Unbeknownst to her, the Kerydin charges had wiped out her entire health reimbursement account.
What gives: According to Leslie Pott, Sandoz vice president of communications, Kerydin is patent-protected and priced “at parity” with its one market competitor, Jublia. She also pointed out that to secure a place on an insurer’s list of approved drugs – its formulary – the company often had to offer substantial discounts to insurers and various middlemen. “We have no visibility into the extent to which these discounts are passed onto patients or payers,” she wrote in an email.
In the application for Food and Drug Administration approval granted in 2014, Anacor Pharmaceuticals highlighted that a yearlong treatment of Kerydin completely cured toe fungus in 6.5 percent of patients for one trial, and 9.1 percent of patients in another.
There are many treatment options for toenail fungus – both older medicines in pill form and newer topical treatments such as Kerydin, said Dr. Shari Lipner, an assistant professor at Weill Cornell Medicine in New York and director of its nail unit. The patient in this case would have been a candidate for “quite a few” of them.
Patients are likely to pay less for the pills, she said, and they also seem to have greater efficacy. Health plans also are less likely to cover the newer treatments, such as Kerydin. If they do, they often require patients to try the less expensive options first.
After a proper diagnosis based on a nail clipping or scraping, Lipner said, patients should be offered all the options and be counseled about their proper use. For example, the oral treatments usually last three months while the topical medicines must be used for a year. And, especially for the newer ones, like Kerydin, insurance coverage can be limited. Cost is likely to be something patients will want to consider, Lipner said.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The bill for a toenail fungus remedy came as big surprise.
Courtesy of Anne Soloviev
hide caption
toggle caption
Courtesy of Anne Soloviev
Xavier Davis, Braun Dermatology and Skin Cancer Center’s practice manager, said a drug’s price tag simply isn’t a factor when prescribers recommend a course of treatment.
“When our providers are treating patients, we’re not treating them based on what the cost’s going to be. We look for what’s the best care for the patient,” Davis said. “If the patient calls and says that’s too expensive then we’ll look for alternatives.”
But patients often don’t see the actual price until it’s too late.
In January, Soloviev’s insurance plan was billed the full price of Kerydin. Of that, $1,439.57 came from her HRA. The difference, $56.52, was covered by a patient-assistance program from the drug manufacturer, explained Jonathan Lee, a pharmacist for My Express Care.
In February, when her prescription was refilled, Soloviev’s plan was again billed the full price. But she didn’t know about that either. A manufacturer coupon was applied to cover what remained of her insurer’s $2,000-annual deductible and the $60 copay. Her insurance then kicked in to pay the difference.
CVS Caremark, the pharmacy benefit manager that administers the drug coverage for Soloviev’s plan, said it was structured to pay for such an expense automatically, using the HRA. Had the HRA been structured differently, the coupon may have covered more of the costs up front, said company spokeswoman Christine Cramer.
Meanwhile, Lee, the pharmacist, said even he didn’t realize that money could be withdrawn directly from a patient’s HRA without her knowledge.
“I just find it is outrageous for a fungal medicine to cost $1,400, to be prescribed for 11 months, and for neither the P.A. nor the pharmacy to warn you,” Soloviev said.
Resolution: Although Soloviev told My Express Care not to renew the prescription, her HRA is depleted. For the rest of the year, she’ll have to pay out-of-pocket costs for any other medications, an expense she hadn’t planned on.
The takeaway: Medical professionals should talk with patients about the options for treatment and what the costs will be. That’s especially true if they are recommending a high-priced medicine.
Patients should take nothing for granted and ask about the cost of every new prescription. And, because costs can vary depending on coverage, they may need to contact their insurance carrier or the PBM that handles their medicine claims. Finally, patients should ask again at the pharmacy – even if that means calling a mail-order pharmacy. It never hurts to ask if there are generic or over-the-counter alternatives.
This is a monthly feature from Kaiser Health News and NPR that dissects and explains real medical bills to shed light on prices in U.S. health care and to help patients learn how to be more active in managing costs. Do you have a medical bill that you’d like us to see and scrutinize? Submit it here and tell us the story behind it.
Revolutionary Pediatrician T. Berry Brazelton Dies At 99
Pediatrician T. Berry Brazelton revolutionized the way parents interacted with their babies and young children. His career spanned more than half a century and included dozens of books, hundreds of publications and a TV show. He died Tuesday, just shy of his 100th birthday.
SEC Charges Theranos Founder Elizabeth Holmes With 'Elaborate, Years-Long Fraud'

{kind=link}
Elizabeth Holmes, founder and CEO of Theranos, speaks at the Clinton Global Initiative’s closing session in 2015 in New York City. The SEC says Holmes and Theranos made exaggerated and false claims.
Andrew Burton/Getty Images
hide caption
toggle caption
Andrew Burton/Getty Images
Elizabeth Holmes, the 34-year-old founder and CEO of the health technology company Theranos, had a compelling story of dropping out of college to launch a multibillion-dollar Silicon Valley venture to revolutionize the blood-testing industry.
But on Wednesday, the Securities and Exchange Commission accused the company, Holmes and its former President Ramesh “Sunny” Balwani of “an elaborate, years-long fraud in which they exaggerated or made false statements about the company’s technology, business, and financial performance” to raise more than $700 million from investors.
Holmes and Theranos agreed to settle the charges against them, the SEC says. Holmes will give up voting control of the company, pay a $500,000 penalty, agree to not serve as a director or officer of a publicly traded company for 10 years and return “the remaining 18.9 million shares that she obtained during the fraud.”
As part of the settlement, Theranos and Holmes neither admitted nor denied the allegations. The company’s “independent directors” said in a statement, “The Company is pleased to be bringing this matter to a close and looks forward to advancing its technology.”
Holmes founded Theranos in 2003 at the age of 19 after dropping out of Stanford University. She attracted famous investors such as Rupert Murdoch and venture capitalist Tim Draper, according to The Wall Street Journal. Henry Kissinger and George P. Schulz sat on the company’s board at one point. At its height, Theranos reached a valuation of more than $9 billion.
Holmes claimed to have developed technology that could “run comprehensive laboratory tests from a tiny sample or a few drops of blood that could be taken from a finger,” as she told an audience at a TED talk, NPR’s Laura Sydell reported in 2016.
But the SEC alleged that “Theranos’ proprietary analyzer could complete only a small number of tests, and the company conducted the vast majority of patient tests on modified and industry-standard commercial analyzers manufactured by others.”
Federal regulators also say Theranos falsely claimed its products were used “on the battlefield in Afghanistan” by the Department of Defense and that the company would make $100 million in revenue in 2014. The military never used Theranos technology and the actual profit was closer to $100,000, the SEC alleges.
Regulators began investigating after The Wall Street Journal’s John Carreyrou reported in late 2015 about doubts over the company’s technology claims and the accuracy of its tests.
Problems for the company quickly began to stack up. In 2016, Theranos cut 40 percent of its staff of 790 and closed blood-test centers in Arizona, California and Pennsylvania. In the same year, Theranos lost a lucrative contract to have its “wellness centers” in Walgreens stores, while regulators prohibited Holmes from owning or operating a lab for two years.
Many investors have lost all of the money they put into the company, the Journal reports, including Murdoch, who lost more than $100 million.
The SEC said it did not settle with Balwani; it says it will litigate a case against him in the Northern District of California. In a statement to multiple media outlets, Balwani’s lawyer Jeffrey Coopersmith said Balwani “accurately represented Theranos to investors to the best of his ability.”
“The Theranos story is an important lesson for Silicon Valley,” Jina Choi of the SEC’s San Francisco office said in a statement. “Innovators who seek to revolutionize and disrupt an industry must tell investors the truth about what their technology can do today, not just what they hope it might do someday.”
Federal prosecutors in San Francisco are still conducting a criminal investigation, according to the Journal, while patients have filed lawsuits consolidated in Arizona accusing Theranos of “consumer fraud and medical battery.”
How Many Opioid Overdoses Are Suicides?

{kind=link}
Mady Ohlman, who lives near Boston and has been sober for more than four years, says many drug users hit a point when the disease and the pursuit of illegal drugs crushes the will to live.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
Mady Ohlman was 22 on the evening some years ago when she stood in a friend’s bathroom looking down at the sink.
“I had set up a bunch of needles filled with heroin because I wanted to just do them back-to-back-to-back,” Ohlman recalls. She doesn’t remember how many she injected before collapsing, or how long she lay drugged-out on the floor.
“But I remember being pissed because I could still get up, you know?”
She wanted to dead, she says, glancing down. A wisp of straight brown hair slips from behind an ear across her thin face.
At that point, says Ohlman, she’d been addicted to opioids — controlled by the drugs, she says — for more than three years.
“And doing all these things you don’t want to do that are horrible — you know, selling my body, stealing from my mom, sleeping in my car,” Ohlman says. “How could I not be suicidal?”
For this young woman, whose weight had dropped to about 90 pounds, who was shooting heroin just to avoid feeling violently ill, suicide seemed a painless way out.
“You realize getting clean would be a lot of work,” Ohlman says, her voice rising. “And you realize dying would be a lot less painful. You also feel like you’ll be doing everyone else a favor if you die.”
Ohlman, who has now been sober for more than four years, says many drug users hit the same point, when the disease and the pursuit of illegal drugs crushes their will to live. Ohlman is among at least 40 percent of active drug users who wrestle with depression, anxiety or another mental health issue that increases the risk of suicide.
Measuring suicide among patients addicted to opioids
Massachusetts, where Ohlman lives, began formally recognizing in May 2017 that some opioid overdose deaths are suicides. The state says confirmed suicides are only about 2 percent of all overdose deaths, but Dr. Monica Bharel, head of Massachussett’s department of public health, says it’s very difficult to determine the person’s true intent.
“For one thing, medical examiners use different criteria for whether suicide was involved or not,” Bharel says, and the “tremendous amount of stigma surrounding both overdose deaths and suicide sometimes makes it extremely challenging to piece everything together and figure out unintentional and intentional.”
Research on drug addiction and suicide suggests much higher numbers.
“[Based on the literature that’s available] it looks like it’s anywhere between 25 and 45 percent of deaths by overdose that may be actual suicides,” says Dr. Maria Oquendo, immediate past president of the American Psychiatric Association.
Oquendo points to one study of overdoses from prescription opioids that found 54 percent were unintentional. The rest were either suicide attempts or undetermined.
Several large studies show an increased risk of suicide among drug users addicted to opioids, especially women. In a study of 5 million veterans, women were eight times as likely as others to be at risk for suicide, while men faced a twofold risk.
The opioid epidemic is occurring at the same time suicides have hit a 30-year high, but Oquendo says few doctors look for a connection.
“They are not monitoring it,” says Oquendo, who chairs the department of psychiatry at the University of Pennsylvania. “They are probably not assessing it in the kinds of depths they would need to prevent some of the deaths.”
That’s starting to change. A few hospitals in Boston, for example, aim to ask every patient admitted about substance use, as well as about whether they’ve considered hurting themselves.
“No one has answered the chicken and egg [question],” says Dr. Kiame Mahaniah, a family physician who runs the Lynn Community Health Center in Lynn, Mass. Is it that patients “have mental health issues that lead to addiction, or did a life of addiction then trigger mental health problems?”
With so little data to go on, “it’s so important to provide treatment that covers all those bases,” Mahaniah says.
‘Deaths of despair’
When doctors do look deeper into the reasons patients addicted to opioids become suicidal, some economists predict they’ll find deep reservoirs of depression and pain.
In a seminal paper published in 2015, Princeton economists Angus Deaton and Anne Case tracked falling marriages rates, the loss of stable middle-class jobs and rising rates of self-reported pain. The authors say opioid overdoses, suicides and diseases related to alcoholism are all often “deaths of despair.”
“We think of opioids as something that’s thrown petrol on the flames and made things infinitely worse,” Deaton says, “but the underlying deep malaise would be there even without the opioids.”
Many economists agree on remedies for that deep malaise. Harvard economics professor David Cutler says solutions include a good education, a steady job that pays a decent wage, secure housing, food and health care.
“And also thinking about a sense of purpose in life,” Cutler says. “That is, even if one is doing well financially, is there a sense that one is contributing in a meaningful way?”
Tackling despair in the addiction community
“I know firsthand the sense of hopelessness that people can feel in the throes of addiction,” says Michael Botticelli, director of the Grayken Center for Addiction at Boston Medical Center; he is in recovery for an addiction to alcohol.
Botticelli says recovery programs must help patients come out of isolation and create or recreate bonds with family and friends.
“The vast majority of people I know who are in recovery often talk about this profound sense of reestablishing — and sometimes establishing for the first time — a connection to a much larger community,” Botticelli says.
Ohlman says she isn’t sure why her attempted suicide, with multiple injections of heroin, didn’t work.
“I just got really lucky,” Ohlman says. “I don’t know how.”
A big part of her recovery strategy involves building a supportive community, she says.
“Meetings; 12-step; sponsorship and networking; being involved with people doing what I’m doing,” says Ohlman, ticking through a list of her priorities.
There’s a fatal overdose at least once a week within her Cape Cod community, she says. Some are accidental, others not. Ohlman is convinced that telling her story, of losing and then finding hope, will help bring those numbers down.
The National Suicide Prevention Lifeline is 800-273-8255.This story is part of NPR’s reporting partnership with NPR, WBUR and Kaiser Health News.
Virginia Republicans Divided On Medicaid Expansion

{kind=link}
Virginia Governor Ralph Northam meets with state legislators March 10, to discuss next steps in the budget. He wants Medicaid expansion to be a priority.
Craig Carper /WCVE
hide caption
toggle caption
Craig Carper /WCVE
Virginia is among 18 states that have not expanded Medicaid under the Affordable Care Act. But this year, the state legislature is going into a special session to continue discussions about whether or not to include it in their budget. By the time the regular session adjourned Saturday, members of Virginia’s GOP-controlled House of Delegates and Senate could not reach agreement on whether or not to expand Medicaid.
Republican Delegate Barry Knight from the Virginia Beach area calls it, “The 800-pound gorilla in the room.” He’s one of more than a dozen Republicans who voted to include Medicaid expansion in the House budget – along with a work requirement – this year.
It’s a big shift in the House position on the issue and comes after 15 seats flipped in the so-called “blue wave” of last November’s election, which also saw the election of Democratic Governor Ralph Northam.
“On the big-picture issues, I think it was a reawakening and a call to look at things from a different perspective,” says Republican Delegate Chris Peace from the Richmond area.
At a recent rally outside the state Capitol in Richmond, Governor Northam continued his campaign message. “Are you all ready to get this done?” he called to the crowd’s cheers. “Are you ready to expand coverage?”
A December poll showed over 80 percent of likely Virginia voters support an expansion.
“I think the House heard that message, loud and clear. I think the Senate still needs to listen a little bit,” Northam says.
He’s referring to a strong movement against expansion, led by Senate Majority Leader Tommy Norment from the Tidewater area in southeastern Virginia. Norment has come out against the House Republicans who want to expand. He reminds them that despite a slim margin, Republicans are still in charge and could stop Medicaid expansion.
“I do think that the House of Delegates is waiting for that moment of lucidity and epiphany to realize that their majority is 51 to 49,” Norment says.
But President Trump has managed to mobilize Democratic voters, says Bob Holsworth, a former political science professor at Virginia Commonwealth University. He thinks there’s a greater chance of state expansion this year.
It could pass in the Senate, he says, because of a potential wildcard.
That wildcard is Republican Senator Emmett Hanger from mostly-rural central Virginia. Hanger has expressed support for some form of Medicaid expansion, and has a track record of voting independently, says Holsworth.
“What Hanger has said that’s very interesting … is that if he decides to support some version of Medicaid expansion, he says, ‘There are a number of other Republicans who are going to go over with me.’ “
However, Hanger isn’t happy about a tax on hospitals that’s been incorporated into the House’s budget to help pay for the state’s share of expansion costs. The tax accounts for about three quarters of the over $400 million Medicaid-related gulf between House and Senate budgets.
If legislators don’t come up with a budget that includes Medicaid expansion, Governor Northam has a plan B. He says he’ll introduce an amendment to add it back into the budget. In the amendment process, the Lieutenant Governor, Justin Fairfax, gets a vote if the Senate ties. Fairfax says he’d be happy to vote to expand coverage to up to 400,000 low-income Virginians.
“There are so many people that we can help and we have the means to do it if we expand Medicaid. We just have to have the political will to do it,” Fairfax says.
Among those expansion would help in Virginia: low-income adults without children.
“An adult who does not have children can have zero income – can be totally impoverished – and they cannot get Medicaid,” says Jill Hanken with the Virginia Poverty Law Center.
And family of three with a total income of about $10,000 doesn’t qualify for Medicaid, she says.
“It’s hard to explain to them that they don’t have a choice: they’re not eligible for Medicaid,” she says, and and they’re not eligible for subsidies for insurance on the exchange, so health insurance is out of reach. “And the reason is because Virginia hasn’t expanded Medicaid,” she says.
The special session begins April 11. The state needs a budget agreement by June 30 to prevent a government shutdown.
This story is part of a reporting partnership with NPR, local NPR stations and Kaiser Health News.