When The Flu Hits Campus, The Gesundheit Machine Will Be Ready

Undergraduate Shira Rubin gamely demonstrates the Gesundheit machine, which collects samples of virus from the breath that sick students exhale. Rubin helps Dr. Somayeh Youssefi (left) set up the machine before patients use it.
Selena Simmons-Duffin/WAMU
hide caption
toggle caption
Selena Simmons-Duffin/WAMU
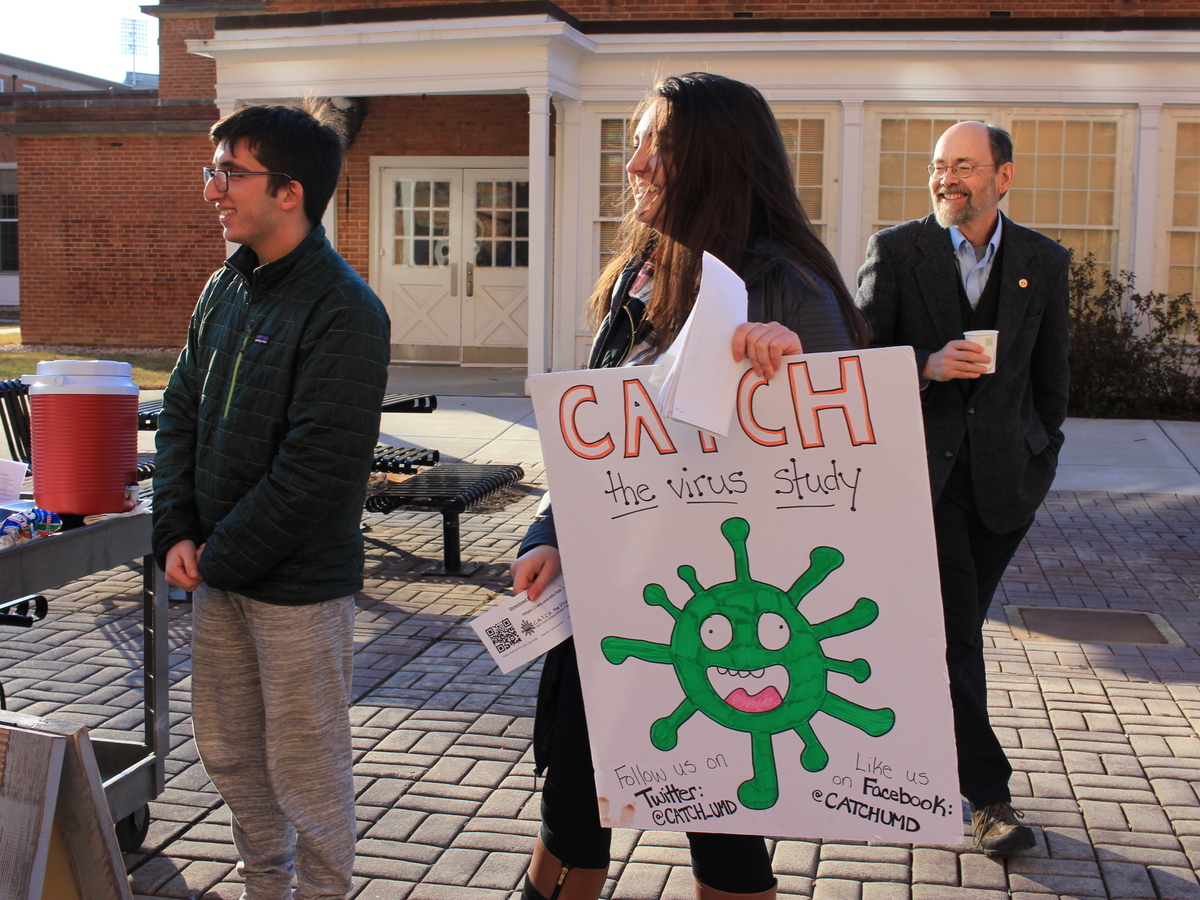
On a blustery winter day, Dr. Don Milton and his undergraduate research assistants, Louie Gold and Amara Fox, are recruiting students for his new study on how the flu — and other viruses — spread.
As incentives, they have vouchers for the school convenience store and free hot chocolate.
Milton, a professor at the University of Maryland, College Park, is hoping dozens of students will enroll for the study, which will help him look at flu transmission. When one of them gets sick, the student will be sent to the clinic at the School of Public Health, just across the street from the dorms.

{kind=link}
{kind=link}
Louie Gold, Amara Fox and Dr. Don Milton recruit students to join the new virus study they’re working on.
Selena Simmons-Duffin / WAMU
hide caption
toggle caption
Selena Simmons-Duffin / WAMU
One student does come by, but doesn’t make the cut. “She had some of the right symptoms: cough, little bit of runny nose, but didn’t have much of a fever,” says Dr. Barbara Albert, who screens for the study.
Those sick enough will get sent around the corner to a room with a crazy-looking, Rube-Goldberg-like contraption known as the Gesundheit machine.
For half an hour, the student sits in the machine. As the student breathes, the machine collects whatever virus they’ve got from the droplets in their breath.
The researchers will then use the student’s contacts to try to figure out how infections spread from person to person: “roommates, study buddies, girlfriends and boyfriends,” Milton says. “We’re going to swab them every day for a week to see if they get infected.”
If the student’s contacts get infected, researchers will try to pin down whether they got the bug from the original subject or someone else.
“We’re going to deep sequence the genetic code of the agent to see if it was really exactly the same thing,” Milton explains. He’s aware that confirming that your roommate gave you a horrible flu could ruin some perfectly nice relationships, but it’s for science.
The fact is, he says, researchers don’t know that much about the mechanics of how bugs spread, so he’s trying to understand it from every possible angle.
“We’re measuring the environment in the rooms, contact, biomarkers from blood, what they’re shedding into the air,” he says.
All the data will also help people design spaces to keep infections from spreading too easily and protect ourselves more effectively.
That’s how he and his research staff can be around sick people all the time without getting infected themselves. They all got flu shots, and he installed a system that killed germs with ultraviolet light.
During his last flu study, it worked. “Not a single person on my research team got the flu that year. Even though we saw 156 people, some of whom were shedding up to 10 million copies per half hour of the virus, none of my people got sick.”
He hopes environmental measures like these could be used to fight bugs that are even worse than the flu.
“What about pandemics and what about new infections that come along? How can we defend against those?” Milton asks. “It is possible, even if it’s airborne, to protect against it. We just need to understand how it works better.”
The information they get from this study could, for example, lead to better ventilation systems that would make it harder for the flu and even more dangerous viruses to spread.
This story is part of a reporting partnership with NPR, local member stations and Kaiser Health News. Selena Simmons-Duffin is a producer at NPR’s All Things Considered, currently on an exchange with Washington, D.C., member station WAMU.
Venezuela's Health Care System Ready To Collapse Amid Economic Crisis

{kind=link}
A volunteer from the non-profit Accion Solidaria organizes imported medicines alphabetically, in a store room in Caracas, Venezuela, last April. The Pharmaceutical Federation of Venezuela estimates the country is suffering from an 85 percent shortage of medicine.
Fidel Suarez/AP
hide caption
toggle caption
Fidel Suarez/AP
The death of a former major league baseball player in his native Venezuela this week is renewing concerns over the Latin American country’s growing health crisis amid ongoing economic and political turmoil.
Marcos Carvajal, a 34-year-old former pitcher for the Colorado Rockies and Florida Marlins, died of pneumonia on Tuesday. He fell sick in December, but the antibiotics needed to treat the illness were hard to find. Drugs for Carvajal eventually were sent from abroad but he relapsed, returned to the hospital on Monday and died the next day.
The Pharmaceutical Federation of Venezuela estimates the country is suffering from an 85 percent shortage of medicine amid an economic crisis also marked by severe hyperinflation and food scarcity.
The entire Venezuelan health care system is on the verge of collapse, says Francisco Valencia, head of the public health advocacy group Codevida. Some hospitals lack electricity, and more than 13,000 doctors have left Venezuela in the past four years in search of better opportunities.
“They don’t give food to the patients in the hospital,” Valencia tells Here & Now’s Peter O’Dowd. “They don’t have the proper medical supplies to take care of the people who go to the emergency [room] like gloves, like every basic thing they need for an emergency.”
According to the pharmaceutical association, there is also a 90 percent deficit of other medical supplies and drugs used to treat more serious conditions like cancer.
The shortage has forced Venezuelans to go looking for medicine on the black market, Valencia says. Even if they find the right medicine, which is often smuggled from Colombia and Brazil and could be expired, most people can’t afford it.
The crisis affects Valencia personally, who relies on medication for a kidney transplant.
“I haven’t received my medicine since August last year,” he says. “Right now, I’m taking medicines that [have] expired, and my transplant is at risk.”
Venezuela’s President Nicolas Maduro has refused to accept humanitarian aid, blocking shipments of medicine and first aid supplies. Government data shows infant mortality rose by 30 percent in 2016 and malaria infections shot up 76 percent, Reuters reports.
“So most countries when they’re hit by a crisis, they’re taking aid from other countries, from NGOs,” Associated Press reporter Hannah Dreier told NPR in 2016. “But Venezuela keeps refusing to take donations that other countries are offering and is actually turning back shipments of donations that people have given in places like the U.S., not letting medicine in.”
Drug prices have skyrocketed along with those for food and other basic necessities. The International Monetary Fund predicts inflation will soar to 13,000 percent this year and the economy will shrink by 15 percent.
Earlier this week, the government announced it would abandon one of its two official foreign exchange rates, which had been used for food and medicine imports, Reuters reports. The policy change could encourage businesses to import more goods, but critics say it won’t be very effective due to the lack of hard currency in Venezuela.
The elimination of the exchange rate was “a step in the right direction because it helps correct foreign exchange distortion,” Asdrubal Oliveros of local consultancy Ecoanalitica told Reuters. “But without dollars, things will continue to be more complicated.”
Since the collapse of Venezuela’s oil-rich economy in 2014, the country has struggled to raise hard currency. The monthly minimum wage for many Venezuelans is now equal to $3, according to the AP.
Maduro blames the country’s growing crisis on foreign economic sanctions, claiming that the U.S. is leading an effort to wipe out socialism in Venezuela, according to Reuters. Presidential elections are set to be held by April 30, which is much earlier than usual, but Venezuela’s pro-government Supreme Court last week banned the main opposition party from running.
Can Cooking Classes Keep Chronic Heart Failure Patients Out Of The Hospital?

{kind=link}
Leah Sarris (center) is the head chef and program director at the Goldring Center for Culinary Medicine at Tulane University. She teaches healthy cooking techniques and educates people about the significant role that food plays in preventing and managing diseases.
Paula Burch-Celentano | Tulane U
hide caption
toggle caption
Paula Burch-Celentano | Tulane U
Shirline Burbanks is one of the 6.5 million Americans suffering from congestive heart failure (CHF). Recently, she checked herself in to the Tulane Medical Center in New Orleans, complaining of shortness of breath. But unlike most other CHF patients in the U.S., within hours of her admittance, Burbanks was met at her bedside with an offer: to sign up for cooking classes.
The offer came from Colleen McCullough, a research coordinator at the Goldring Center for Culinary Medicine at Tulane. She started working last August to recruit people for the pilot phase of an 18-month study. Its goal is to determine whether the 30-day readmission rate for CHF patients, which is a whopping 22 percent, can be cut by almost half — all by teaching these patients how to make their own meals.
Many of McCullough’s potential subjects have been eating loads of saturated fat and sodium their whole lives. Such habits can lead to conditions like high blood pressure and coronary artery disease, which may increase their likelihood of developing CHF, a chronic condition in which the heart can’t pump enough blood and oxygen to the body’s tissues. High amounts of fat and salt can aggravate CHF, trapping patients in a cycle of ongoing illness.
The condition is “a great one to intervene in,” says Kristi Artz, a physician and culinary medicine specialist at healthcare organization Spectrum Health in Grand Rapids, Mich., one of 45 U.S.-based medical training programs that licenses Goldring’s curriculum. “Unless these patients change their dietary behavior, over time their [CHF] just worsens. “
Fried, salty, sweet food is “such a cornerstone of New Orleans culture,” says McCullough. “When I first start talking to patients” in the hospital — she’s interviewed 120 so far and enrolled 60; 30 have taken classes upon being released — “they usually come clean about their diet pretty quickly.” Teaching them to change their eating habits may seem like a simple fix, but as the Goldring research team knows, nothing could be further from the truth.
The battle begins before patients hear about the center’s kitchen classroom. Many of them live below the poverty line. This sets them up for a multitude of hardships: food insecurity and poor access to nutrition, exacerbated by lousy public transportation. Mobility is often a problem: CHF sufferers can have a hard time walking because of breathing issues or swelling in their feet. In designing the study, Timothy Harlan, Goldring’s executive director, wrote taxi vouchers into the grant request, to make it easier for patients to commute to and from Goldring’s bright, large kitchen in the bustling Mid-City neighborhood.
With transportation streamlined, other challenges suddenly translate into strong selling points for the classes. “When you’re food insecure, the fact that you can get free meals in addition to learning how to make them is pretty attractive,” points out Leah Sarris, Goldring’s head chef and program director.
The isolation many homebound CHF patients experience is another motivator, says McCullough. “They’ll tell me, I have nothing else to do; sign me up for every class this week.”
The CHF patients are folded into Goldring’s usual 2-hour community classes (the center also runs classes for med students). Once in the kitchen, friendships born of shared medical experience quickly blossom. “They hug when they see each other, and cook in the same groups, and talk and text between classes,” McCullough says.
According to Mary Ann McLaughlin, a cardiologist at Mount Sinai Medical Center in New York City, “Any time you have patients with severe chronic conditions, socialization has an important impact. Food bonds people, and they can learn from each other, and share their fears and concerns.”
The CHF students have severe restrictions on sodium, and also on fluid intake, because they retain it. Says Sarris, “That basically means we don’t teach them how to make soup.” What she does teach them is how to make pasta sauces that substitute mushrooms or lentils for red meat. Or New Orleans’ favorite red beans and rice, which gets its deep layers of flavor from spices like smoked paprika, rather than pickled pork and sausage.
The classes focus on more than tweaking dishes, though. Sarris explains they often must guide students — many of whom do not know how to cook, and may not read beyond a fourth-grade level — through nutritional basics, using lots of visual aids. They also learn how to shop on a budget, use one bag of rice to make multiple meals, and freeze leftovers. “But more than anything,” she says, “we’re teaching them kitchen confidence.”
The second, more scientifically rigorous leg of the study will likely begin this month, and use randomized controls. They’ll enroll 20 CHF patients, half of whom will take classes; the other half will not. Then, says McCullough, “We’ll compare readmissions.” After the first phase, some folks checked back into the hospital. Those numbers, and the reasons for dropouts, have not yet been assessed, but McCullough says most participants have managed to stay readmission-free.
If that continues for the remainder of the study, the Goldring researchers will consider it a win — both for the health of CHF patients, and the center’s fiscal future. Hospitals aren’t reimbursed for CHF readmissions that happen within a month. So even a 10 percent drop in rates, explains Harlan, “would fund all of Goldring’s programming, full stop.”
Other health professionals are also awaiting Goldring’s CHF research outcomes. “Up to this point, we’ve just been focused on disease care,” says Spectrum’s Artz. “If we could implement [culinary] programs as part of standard medical treatment, we could give out food prescriptions. That’s where I hope this leads.”
The Goldring pilot has already engendered small successes. “I had one 50-year-old patient who in 20 years had never cooked for her husband before,” says Sarris. “We gave her the support to try it, and the effects were pretty profound. Before she took classes, chopping veggies seemed overwhelming to her.”
Meanwhile, Burbanks has come close to becoming a vegetarian — even though she hadn’t heard the word before she came to class. “She’s constantly reworking her gumbo recipe now, and she texts me pictures as if she’s asking, “Will you validate this?” says McCullough. “Yeah, I can do that.”
Lela Nargi is a Brooklyn-based journalist and cookbook author. Her writing has appeared in publications including Gastronomica, Civil Eats and Roads & Kingdoms.
Unnecessary Medical Care: More Common Than You Might Imagine

{kind=link}
Drawn Ideas/Ikon Images/Getty Images
It’s one of the intractable financial boondoggles of the U.S. health care system: Lots and lots of patients get lots and lots of tests and procedures that they don’t need.
Women still get annual cervical cancer testing even when it’s recommended every three to five years for most women. Healthy patients are subjected to slates of unnecessary lab work before elective procedures. Doctors routinely order annual electrocardiograms and other heart tests for people who don’t need them.
That all adds up to substantial expense that helps drive up the cost of care for all of us. Just how much, though, is seldom tallied. So, the Washington Health Alliance, a nonprofit dedicated to making care safer and more affordable, decided to find out.
CALLOUT:
Have you worked in the health insurance industry? You have expertise that could help ProPublica’s reporting. Please share your insights with Marshall Allen to help him learn about the industry.
The group scoured the insurance claims from 1.3 million patients in Washington state who received one of 47 tests or services that medical experts have flagged as overused or unnecessary.
What the group found should cause both doctors, and their patients, to rethink that next referral. In a single year:
- More than 600,000 patients underwent a treatment they didn’t need, treatments that collectively cost an estimated $282 million.
- More than a third of the money spent on the 47 tests or services went to unnecessary care.
- 3 in 4 annual cervical cancer screenings were performed on women who had adequate prior screenings – at a cost of $19 million.
- About 85 percent of the lab tests to prep healthy patients for low-risk surgery were unnecessary – squandering about $86 million.
- Needless annual heart tests on low-risk patients consumed $40 million.
Susie Dade, deputy director of the alliance and primary author of the report released Thursday, said almost half the care examined was wasteful. Much of it comprised the sort of low-cost, ubiquitous tests and treatments that don’t garner a second look. But “little things add up,” she said. “It’s easy for a single doctor and patient to say, ‘Why not do this test? What difference does it make?’ “
ProPublica has spent the past year examining how the American health care system squanders money—often in ways that are overlooked by providers and patients alike. The waste is widespread – estimated at $765 billion a year by the National Academy of Medicine, about a fourth of all the money spent each year on healthcare.
The waste contributes to health care costs that have outpaced inflation for decades, making patients and employers desperate for relief. This week Amazon, Berkshire Hathaway and JPMorgan rattled the industry by pledging to create their own venture to lower their health care costs.
Wasted spending isn’t hard to find once researchers—and reporters— look for it. An analysis in Virginia identified $586 million in wasted spending in a single year. Minnesota looked at fewer treatments and found about $55 million in unnecessary spending.
Dr. H. Gilbert Welch, a professor at The Dartmouth Institute who writes books about overuse, said the findings come back to “Economics 101.” The medical system is still dominated by a payment system that pays providers for doing tests and procedures. “Incentives matter,” Welch said. “As long as people are paid more to do more they will tend to do too much.”
Dade said the medical community’s pledge to “do no harm” should also cover saddling patients with medical bills they can’t pay. “Doing things that are unnecessary and then sending patients big bills is financial harm,” she said.
Officials from Washington’s hospital and medical associations didn’t quibble with the alliance’s findings, calling them an important step in reducing the money wasted by the medical system. But they said patients bear some responsibility for wasteful treatment. Patients often insist that a medical provider “do something,” like write a prescription or perform a test. That mindset has contributed to problems like the overuse of antibiotics – one of the items examined in the study.
And, the report may help change assumptions made by providers and patients that lead to unnecessary care, said Jennifer Graves, vice president for patient safety at the Washington State Hospital Association. Often a prescription or technology isn’t going to provide a simple cure, Graves said. “Watching and waiting” might be a better approach, she said.
To identify waste, the alliance study ran commercial insurance claims through a software tool called the Milliman MedInsight Health Waste Calculator. The services were provided during a one-year period starting in mid-2015. The claims were for tests and treatments identified as frequently overused by the U.S. Preventive Services Task Force and the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. The tool categorized the services one of three ways: necessary, likely wasteful or wasteful.
The report’s “call to action” said overuse must become a focus of “honest discussions” about the value of health care. It also said the system needs to transition from paying for the volume of services to paying for the value of what’s provided.
ProPublica is a nonprofit newsroom based in New York. You can follow Marshall Allen on Twitter:@marshall_allen.
CDC Director Brenda Fitzgerald Resigns After Reports Show Investment In Tobacco Stocks

Brenda Fitzgerald, director for the Centers for Disease Control and Prevention, resigned on Wednesday because of financial conflicts of interest. The chief public health official bought stocks in tobacco and health care companies after she started working at the agency.
CDC Director Resigns Because Of 'Complex' Financial Entanglements

{kind=link}
Brenda Fitzgerald, Georgia Department of Public Health commissioner, and Gov. Nathan Deal respond to questions about Ebola victims at Emory University Hospital and efforts to screen for Ebola in 2014. A report in Politico revealed documents showing several new investments, including in a tobacco company, by Centers for Disease Control and Prevention Director Brenda Fitzgerald.
David Tulis/AP
hide caption
toggle caption
David Tulis/AP
Dr. Brenda Fitzgerald, director of the Centers for Disease Control and Prevention, resigned Wednesday following reports that she bought shares in a tobacco company, among other financial dealings that presented a conflict of interest.
“Dr. Fitzgerald owns certain complex financial interests that have imposed a broad recusal limiting her ability to complete all of her duties as the CDC Director,” according to a statement issued by Matt Lloyd, a spokesman for the Department of Health and Human Services. “Due to the nature of these financial interests, Dr. Fitzgerald could not divest from them in a definitive time period.”
A report in Politico published Tuesday revealed documents showing several new investments, including in a tobacco company, that Fitzgerald made after she took over the agency’s top job. The CDC is a lead federal agency in preventing smoking and tobacco-related diseases.
Fitzgerald had come under fire on Capitol Hill for not divesting financial interests in other companies that present potential conflicts of interest, including drugmaker Merck, health insurer Humana and US Food Holding Co.
The Politico report, relying on documents obtained under the Freedom of Information Act, shows that one day after Fitzgerald purchased stock in Japan Tobacco, she toured the CDC’s Tobacco Laboratory, which studies tobacco’s toxic effects. She sold the tobacco shares on Oct. 26 and all of her stock holdings above $1,000 by Nov. 21, well into her term as CDC director.
Fitzgerald previous served as the commissioner of the Georgia Division of Public Health.
What Do Amazon, JPMorgan Chase And Berkshire Hathway Have Planned For Health Care?
Amazon, Berkshire Hathaway and JPMorgan Chase announced a joint company that will use technology to lower health care costs. NPR’s Steve Inskeep talks with Kevin Schulman of Duke University.
What's The 5-Year-Survival Rate For Cancer Patients Around The World?

{kind=link}
Chemotherapy has made a tremendous difference in survival rates for children with acute lymphoblastic leukemia, the most common type of childhood cancer.
FatCamera/Getty Images
hide caption
toggle caption
FatCamera/Getty Images
What happens after a cancer diagnosis?
That’s the question investigated by a study published by the CONCORD program on cancer survival published on Tuesday in The Lancet. The study looks at patient records for adults and children diagnosed with a variety of cancers in 71 countries. The records are from 2010 to 2014. The goal is to compare five-year survival rates, a number used to assess effectiveness of treatment.
The overall message is that there is improvement in cancer survival rates but with a caveat. As lead author Dr. Claudia Allemaninotes, “That is particularly true in developed countries and less so in developing countries.”
Case in point: Childhood cancers in upper–income countries — like the U.S. and much of Europe —are treated so successfully that the five-year survival rate often reaches 90 percent or even higher. That was reflected in the data for acute lymphoblastic leukemia, the most common childhood cancer. By contrast, in some middle-income countries — China, Mexico and Brazil, for example — it’s less than 60 percent.
But there are some surprising revelations. Some countries in Asia do a far better job diagnosing and treating stomach and esophageal cancers than the United States does. Five-year survival rates in South Korea and Japan are 68 percent and 60 percent, respectively, versus 33 percent in the U.S.
To learn more, we spoke with Allemani from the Cancer Survival Group at the London School of Hygiene & Tropical Medicine and Michel Coleman, professor of epidemiology and vital statistics at the same institution. Here are some of the topics we discussed.
Why are children diagnosed with leukemia in Mexico and Brazil not faring as well as children with the same diagnosis in countries like the U.S.?
First, says Coleman, remember that in the 1950s and ’60s, in Western countries, the survival rate for children diagnosed with leukemia was five percent or lower after five years. “There was really no treatment available,” he says.
Today, largely because of chemotherapy as well as some other treatments, like stem cell transplants, survival rates have soared in the West.
But that doesn’t mean that having the right drugs is the solution for countries still struggling with these cancers. “The treatments are quite aggressive and repress the immune system so a child’s ability to defend against infections can be drastically reduced,” he says. “It isn’t simply a question of buying more drugs but a broader upgrading of the health service” to provide supportive care for the child during chemo.
What’s behind the stomach cancer success in parts of Asia?
Countries like South Korea, Japan and Taiwanhave historically had high rates of stomach and esophageal cancer. So local governments as well as companies have set up annual screenings. “They are very skilled at diagnosing very early and at very aggressive surgical techniques to manage those cancers,” says Coleman. But as Allemani points out, the survival rates for other cancers — melanoma and leukemia, for example — “are really quite low.”
Middle-income countries can be as effective in treating cancer as high-income countries.
Allemani points to Costa Rica: “Generally speaking we found very good survival for some cancers” in this upper middle-income nation. It’s one of the countries in the group with a five-year survival rate of 85 percent or higher, including the U.S., Canada, Japan and 16 European countries.
Getting cancer data is harder than you think.
The information in the report comes from registries that cite cancer diagnoses and deaths from cancer. Of the 85 countries contacted, “more than 20 wanted to participate but could not,” says Coleman, because registries have closed or lacked resources to keep reliable data — or did not have legal permission to link data from registries of diagnosis to registries of deaths from cancer. And these problems cropped up in a variety of countries, from low-income to high-income. For example, there is no data from any country in Africa in the childhood cancer section. And, Coleman says, “four of the 13 jurisdictions in Canada were not able to provide data in time for this study.”
That lack of data is “lamentable,” he says.
Without such data, Allemani says, “health ministries are flying blind on cancer control.”
How Amazon, JPMorgan Chase, Berkshire Hathaway Could Reshape Health Care Industry
NPR’s Ari Shapiro speaks with Steven Halper, managing director at Cantor Fitzgerald about Amazon, Berkshire Hathaway and JPMorgan Chase’s announcement that they are creating a new health care company.
Health Stocks Drop After Amazon, Berkshire Hathaway And JPMorgan Chase Announcement
Amazon, JPMorgan Chase and Berkshire Hathaway are launching an effort to make health care simpler and cheaper for their own workers. The announcement sent health company stock prices lower.