Spot Shortages Of Antiviral Drugs Seen As Flu Season Drags On

People 6 months and older should get vaccinated against the flu, says this government poster on display in a health center in Decatur, Ga.
David Goldman/AP
hide caption
toggle caption
David Goldman/AP
The peak of the flu season could still be several weeks away, federal health officials cautioned Friday.
“We may be on track to break some recent records,” said Dr. Anne Schuchat, acting director of the Centers for Disease Control and Prevention. Nearly all states are still reporting widespread flu activity, with less severe reports only coming from Oregon and Hawaii.
“Flu is incredibly difficult to predict and we don’t know if we’ve hit the peak yet,” Schuchat said in a call with reporters. “We could still see several more weeks of increased activity.”
Health officials don’t directly count flu cases and deaths for the general population. They do track deaths among children, which climbed to a total of 63 for this season.
Another measure is the percentage of deaths attributed to flu or pneumonia, which often accompanies influenza. Last week, 1 in 10 of all deaths reported in the United States were caused by flu or pneumonia.
The rate of flu activity is similar to the rate in 2009, which was the last flu pandemic, “though that doesn’t mean we’re having a pandemic,” Schuchat said.
The strain of flu known as H3N2 remains the dominant form circulating in the United States. It’s a particularly severe strain that isn’t easily stopped by the current vaccine.
Two other strains are on the rise, however, and they generally cause milder symptoms. They’re also more likely to be blocked by the flu vaccine. So, Schuchat said, it’s still not too late to get vaccinated.
The CDC recommends antiviral medications, such as Tamiflu or the generic version called oseltamivir, for vulnerable populations hit by flu. Those groups include young children, pregnant women, the elderly and people with heart or lung disease.
There are spot shortages of the antiviral drugs, Schuchat said. People seeking them may need to call multiple pharmacies to fill their prescriptions.
The CDC has been working with insurers and pharmacies to alleviate those shortages and to make brand-name drugs available at a lower cost when generics aren’t available.
“I wish there were better news this week,” Schuchat said.
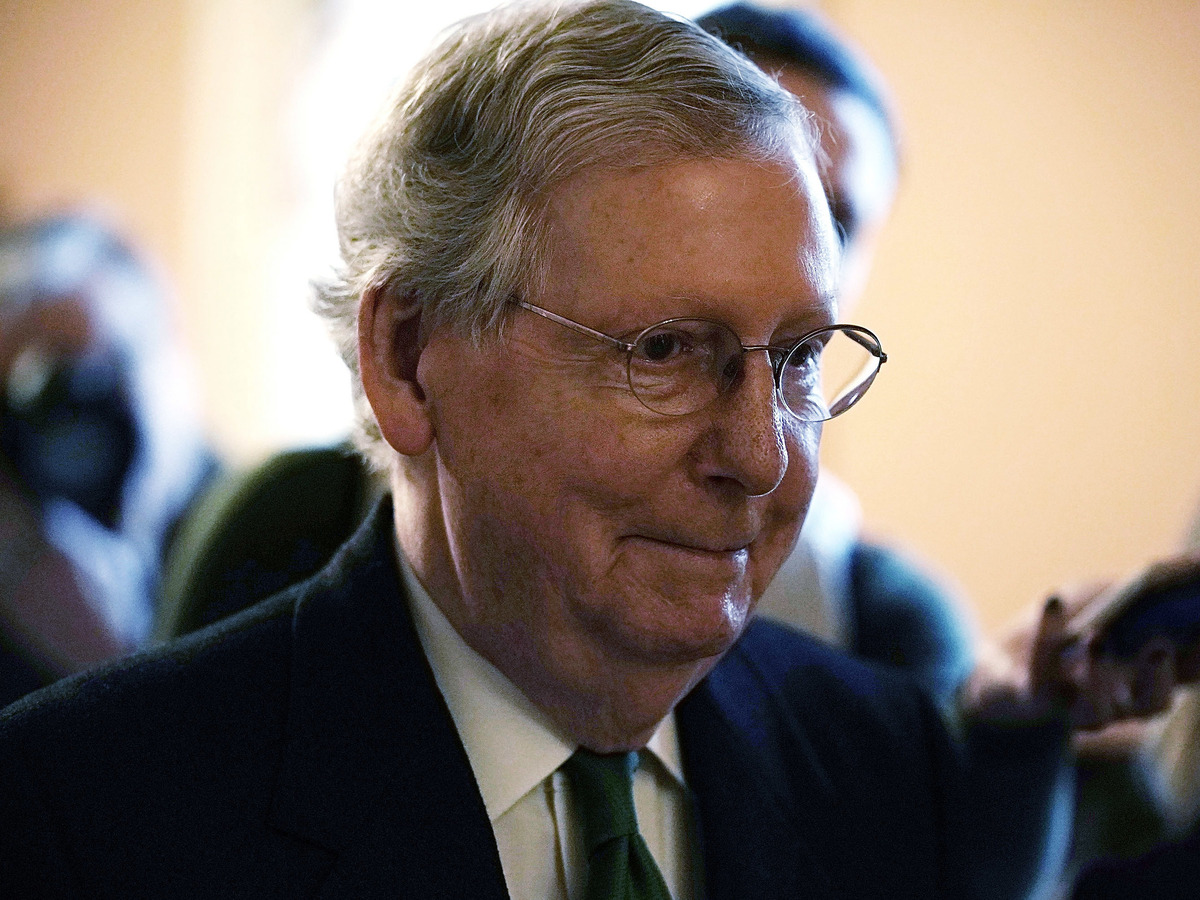
Senate Budget Deal Would Give A Boost To Health Programs

“This bill represents a significant bipartisan step forward,” Senate Majority Leader Mitch McConnell said Wednesday.
Alex Wong/Getty Images
hide caption
toggle caption
Alex Wong/Getty Images
In a rare show of congressional cooperation, Republican and Democratic leaders in the Senate announced a two-year budget deal Wednesday that would increase federal spending for defense as well as key domestic priorities, including many health programs.
Not in the deal, for which the path to the president’s desk remains unclear, is any bipartisan legislation aimed at shoring up the Affordable Care Act’s individual health insurance marketplaces. Senate Majority Leader Mitch McConnell, R-Ky., promised Sen. Susan Collins, R-Maine, a vote on health legislation in exchange for her vote for the GOP tax bill in December. So far, that vote hasn’t materialized.
The deal does appear to include almost every other health priority Democrats have been pushing the past several months, including two years of renewed funding for community health centers and a series of other health programs Congress failed to provide for before they technically expired last year.
“I believe we have reached a budget deal that neither side loves but both sides can be proud of,” said Senate Minority Leader Chuck Schumer, D-N.Y., on the Senate floor. “That’s compromise. That’s governing.”
McConnell said, “This bill represents a significant bipartisan step forward.”
Senate leaders are still negotiating details of the accord, including the size of a cut to the Prevention and Public Health Fund, which would help offset the costs of this legislation.
According to documents circulating on Capitol Hill, the deal includes $6 billion in funding for treatment of mental health issues and opioid addiction, $2 billion in extra funding for the National Institutes of Health, and an additional four-year extension of the Children’s Health Insurance Program, which builds on the six years approved by Congress last month.
In the Medicare program, the deal would accelerate the closing of the “doughnut hole” in Medicare drug coverage that requires seniors to pay thousands of dollars out-of-pocket before catastrophic coverage kicks in. It would also repeal the controversial Medicare Independent Payment Advisory Board, which is charged with holding down Medicare spending for the federal government if it exceeds a certain level.
Members have never been appointed to the IPAB, however, and its use hasn’t so far been triggered by Medicare spending. Both the closure of the doughnut hole and creation of the IPAB were part of the Affordable Care Act.
The agreement would also fund a host of more limited health programs — some of which are known as “extenders” because they often ride along with other, larger health or spending bills.
Those programs include more than $7 billion in funding for the nation’s federally funded community health centers. The clinics serve 27 million low-income people and saw their funding lapse last fall — a delay advocates say had already complicated budgeting and staffing decisions for many clinics.
And in a victory for the physical therapy industry and patient advocates, the accord would permanently repeal a limit on Medicare’s coverage of physical therapy, speech-language pathology and outpatient treatment. Previously, the program capped coverage after $2,010 worth of occupational therapy and another $2,010 for speech-language therapy and physical therapy combined. But Congress had long taken action to delay those caps or provide exemptions — meaning they had never actually taken effect.
According to an analysis by the nonpartisan Congressional Budget Office, permanently repealing the caps would cost about $6.47 billion over the next decade.
Lawmakers would also forestall cuts mandated by the ACA to reduce the payments made to what are called Disproportionate Share Hospitals, which serve high rates of low-income patients. Those cuts have been delayed continuously since the law’s 2010 passage.
Limited programs are also affected. The deal would fund for five years the Maternal, Infant and Early Childhood Home Visiting Program, a program that helps guide low-income, at-risk mothers in parenting. It served about 160,000 families in fiscal year 2016.
“We are relieved that there is a deal for a 5-year reauthorization of MIECHV,” says Lori Freeman, CEO of advocacy group the Association of Maternal & Child Health Programs, in an emailed statement. “States, home visitors and families have been in limbo for the past several months, and this news will bring the stability they need to continue this successful program.”
And the budget deal funds programs that encourage doctors to practice in medically underserved areas, providing just under $500 million over the next two years for the National Health Service Corps and another $363 million over two years to the Teaching Health Center Graduate Medical Education program, which places medical residents in Community Health Centers.
Kaiser Health News correspondent Emmarie Huetteman contributed to this report.
Instead Of Expanding Treatment For Opioids, Trump Says He Will Focus On Enforcing Laws

After declaring opioids a public health emergency, President Trump hasn’t acted on recommendations of a White House Commission on Opioids to expand treatment. Instead of treatment, he says his administration’s focus will be on tougher enforcement of drug laws.
Study Finds 179,000 Nursing Home Residents Needlessly Being Given Antipsychotic Drugs
A new study from Human Rights Watch finds that 179,000 nursing home residents are being needlessly given antipsychotic drugs, despite an FDA warning that they can increase the risk of death for older people with dementia. This is despite a multi-year government campaign to lower the use of antipsychotics in nursing facilities.
Alabama Targets OxyContin Maker Purdue Pharma In Opioid Suit

The state of Alabama is suing Purdue Pharma LP, the maker of OxyContin, for allegedly fueling the opioid crisis by deceiving doctors about prescription painkillers.
Toby Talbot/AP
hide caption
toggle caption
Toby Talbot/AP
Alabama filed a lawsuit in federal court on Tuesday against OxyContin producer Purdue Pharma LP claiming the drug company is fueling the opioid epidemic by deceptively marketing prescription painkillers.
The state alleges that Purdue failed to accurately portray the risks and benefits of opioids, which enabled doctors to widely prescribe them in the treatment of pain. Alabama becomes the latest in a flood of lawsuits by states, counties and cities against drug makers in response to the opioid crisis.
According to Alabama Attorney General Steve Marshall, the state leads the nation in the number of painkiller prescriptions per capita. He tellsHere & Now’s Jeremy Hobson that the lawsuit states Purdue purposely gave doctors misinformation about prescription opioids in order to generate billions of dollars in sales.
“Our average lifespan has reduced in the last two years, and this being the principal reason why,” Marshall says. “We’ve got to be able to make a difference in this issue nationally.”
The lawsuit comes on the heels of a December report by the Alabama Opioid Overdose and Addiction Council. The group of mental health professionals, law enforcement and others was appointed by Alabama Gov. Kay Ivey in August 2017 to devise solutions to the opioid crisis in the state.
At least 30,000 Alabama residents over age 17 are dependent on heroin or prescription painkillers, according to a statement issued by the attorney general’s office.
The opioid council also found the drug overdose death rate in Alabama also increased 82 percent from 2006 to 2014. During that period, 5,128 people died from overdoses. In the U.S, more than 42,000 overdose deaths in 2016 involved opioids, according to the Centers for Disease Control and Prevention.
The lawsuit alleges that marketers persuaded doctors that prescription painkillers weren’t addictive, Marshall says.
“The lies that they were told and trained in over the years whether it be that there was no dosage too high of an opioid … or even this concept of a pseudo-addiction that if somebody appeared in an office demonstrating signs of addiction that just meant that they needed more pain medication,” he says.
Purdue has denied the allegations, writing in a statement that its drugs are approved by the Food and Drug Administration and make up only 2 percent of all opioids prescribed.
“As a company grounded in science, we must balance patient access to FDA-approved medicines, while working collaboratively to solve this public health challenge,” Purdue said in the statement.
Marshall says Alabama targeted Purdue because the company supplies the majority of opioids in the state, according to the lawsuit. Thirteen other states have filed suits against Purdue, according to Reuters.
In its suit against five drug makers, including Purdue, Ohio similarly claimed the drug manufacturers encouraged the idea that the treatment of pain required opioids. As NPR previously reported, the opioid drug industry took off in the 1990s as a result of the health care industry’s effort to better treat chronic pain.
“There was a concerted effort for an extended number of years to really pound this into the heads of doctors,” Ohio Attorney General Mike DeWine told NPR. “And when you’re told something time and time and time again and there’s a lot of advertising that is being spent, yeah, it takes a while to turn that around.”
A federal judge in Ohio is managing more than 200 lawsuits by cities, counties and others over the opioid epidemic, accusing pharmaceutical manufacturers of selling painkillers through deceptive advertising. Forty-one states have also joined forces to investigate the industry.
State and local lawmakers also hope to recover the financial costs of the crisis, echoing successful lawsuits against tobacco companies. Law enforcement, first responders and drug treatment centers across the nation are spread thin trying to combat the opioid epidemic, as noted in the Alabama lawsuit.
While federal regulations led to an 18 percent reduction in 2015 of the amount of opioids prescribed, according to the CDC, the decline has fueled a demand for cheaper options. According to the National Institute on Drug Abuse, about 80 percent of people who use heroin started out with prescription painkillers.
“We continue to see the rise of heroin, fentanyl and carfentanyl in our communities around the country because if we look at the significant reason for the overdoses, those are the drugs that are causing it,” Marshall says. “There is a direct connection between opioids and those particular illicit drugs.”
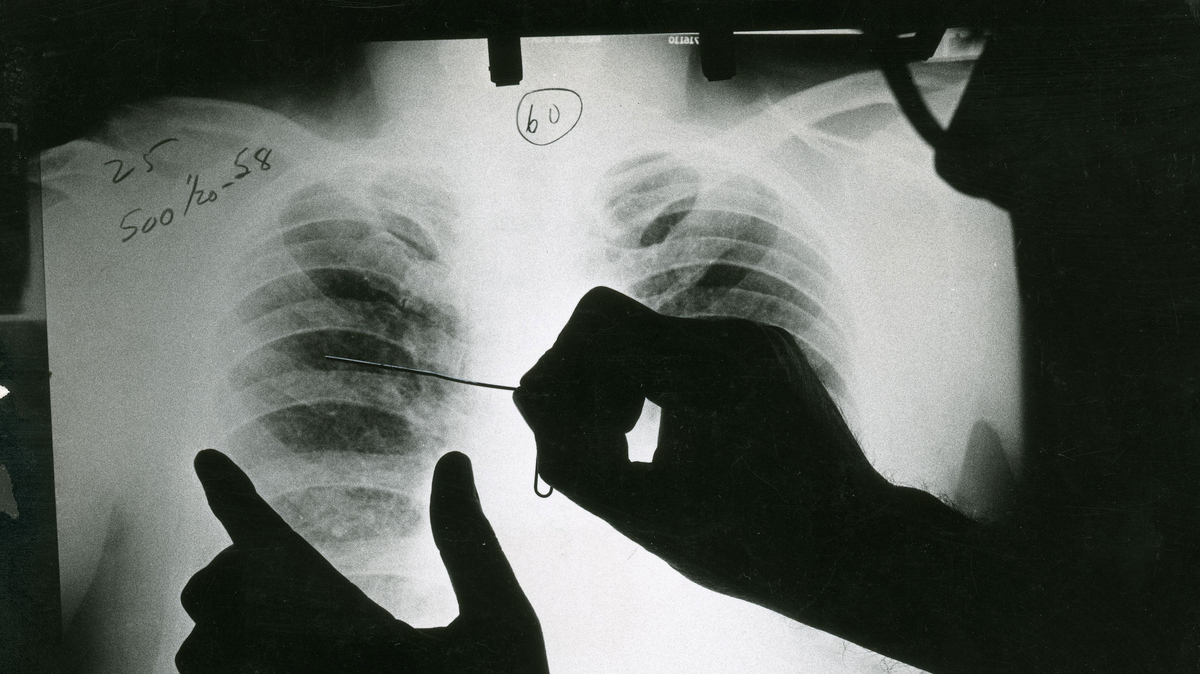
Black Lung Study Finds Biggest Cluster Ever Of Fatal Coal Miners' Disease

In this historical image, a doctor reviews an X-ray of a patient with black lung disease. Federal researchers say they’ve now identified the largest cluster ever recorded of the most advanced stage of the disease.
Michael Sullivan/Getty Images/Science Source
hide caption
toggle caption
Michael Sullivan/Getty Images/Science Source
Updated on Feb. 6 at 3:49 p.m. ET
Epidemiologists at the National Institute for Occupational Safety and Health say they’ve identified the largest cluster of advanced black lung disease ever reported, a cluster that was first uncovered by NPR 14 months ago.
In a research letter published Tuesday in the Journal of the American Medical Association, NIOSH confirms 416 cases of progressive massive fibrosis or complicated black lung in three clinics in central Appalachia from 2013 to 2017.
“This is the largest cluster of progressive massive fibrosis ever reported in the scientific literature,” says Scott Laney, a NIOSH epidemiologist involved in the study.
“We’ve gone from having nearly eradicated PMF in the mid-1990s to the highest concentration of cases that anyone has ever seen,” he said.
The clinics are operated by Stone Mountain Health Services and assess and treat coal miners mostly from Virginia, Kentucky and West Virginia, a region that includes what have historically been some of the most productive coalfields in the country.
“When I first implemented this clinic back in 1990, you would see … five [to] seven … PMF cases” a year, says Ron Carson, who directs Stone Mountain’s black lung program.
The clinics now see that many cases every two weeks, he says, and have had 154 new diagnoses of PMF since the fieldwork for the NIOSH study concluded a year ago.
“That’s an indication that it’s not slowing down,” Carson says. “We are seeing something that we haven’t seen before.”

A slide from a presentation by the National Institute for Occupational Safety and Health shows the progression from a healthy lung to advanced black lung disease.
NIOSH
hide caption
toggle caption
NIOSH
Laney acknowledges that the full scope of what he calls an epidemic is still unknown. “Even with this number, which is substantial and unacceptable, it’s still an underestimate.”
“Nobody looks forward to dying”
PMF, or complicated black lung, encompasses the worst stages of the disease, which is caused by inhalation of coal and silica dust at both underground and surface coal mines. Miners gradually lose the ability to breathe, as they wheeze and gasp for air.

Edward Brown is a 55-year-old former coal miner with progressive massive fibrosis, or complicated black lung disease.
Adelina Lancianese/NPR
hide caption
toggle caption
Adelina Lancianese/NPR
“I’ve seen it too many times,” said Charles Wayne Stanley, a Stone Mountain client with PMF, who spoke with NPR in 2016. “My wife’s grandpa … [I] watched him take his last breath. I watched my uncle die with black lung. You literally suffocate because you can’t get enough air.”
Lung transplants are the only cure, and they’re possible only when miners are healthy enough to qualify.
“[I] can’t breathe, you know. [I] can’t do nothing hardly like I used to,” says Edward Brown, a 55-year-old retired miner from Harlan, Ky., who was diagnosed with PMF at both Stone Mountain and another medical clinic.
“That’s all I got to look forward to is to get worser and worser,” Brown says, pausing for a deep sigh and nervous chuckle. “Nobody looks forward to dying, you know, but it’s a-comin’ and then that worries me.”
Brown’s age and disease fit another finding of the NIOSH study and a trend Carson first disclosed to NPR in December 2016.
“Miners are dying at a much younger age,” he says, noting that in the 1990s, the clinic’s PMF diagnoses typically involved miners in their 60s, 70s and 80s. Now the disease strikes miners in their 50s, 40s and even 30s with fewer years mining coal.
“A high proportion” of the miners in the NIOSH study had severely advanced disease and “coal mining tenure of less than 20 years, which are indications of exceptionally severe and rapidly progressive disease,” the study says.

The lung of deceased West Virginia coal miner Chester Fike was taken out during a double lung transplant when he was 60. He worked in the mines for 35 years.
NIOSH
hide caption
toggle caption
NIOSH
The Stone Mountain study follows a NIOSH review of cases at a small clinic in Coal Run Village, Ky., in 2016. NIOSH researchers confirmed 60 diagnoses of PMF there in 20 months. That alarmed them because NIOSH had earlier reported only 99 cases nationwide in five years.
At the same time, an NPR survey of 11 black lung clinics in Kentucky, Virginia, Pennsylvania and Ohio identified 962 cases, 10 times the original NIOSH count. Since then, NPR’s ongoing survey of clinics has counted nearly 1,000 more cases.
The NPR investigation also found that the likely cause of the epidemic is longer work shifts for miners and the mining of thinner coal seams. Massive mining machines must cut rock with coal and the resulting dust contains silica, which is far more toxic than coal dust.
The spike in PMF diagnoses is also due to layoffs and retirements brought on by the decline in coal mining. Miners who had put off getting checked for black lung earlier began streaming into clinics, especially if they needed the medical and wage replacement benefits provided by black lung compensation programs.
A public health emergency?
There is also concern for the 50,000 coal miners still working.
“They really need to declare this a public health emergency,” says Joe Wolfe, an attorney in Norton, Va., who helps miners file claims for black lung compensation.
“If you had 400 cases of E. coli, [NIOSH] would flood the area with technicians and doctors and nurses checking people’s health,” Wolfe adds. “There are people literally working in the mines right now … that have complicated black lung that do not have a clue.”
NIOSH doesn’t have that authority, according to David Weissman, who directs the agency’s respiratory health program in Morgantown, W.Va. Public health emergencies are declared by the secretary of the U.S. Department of Health and Human Services.
“But I will say that this is a very important problem. We’re very passionate about this problem,” Weissman says. “And we’re going to keep doing everything in our power to address it.”
Multiple NIOSH and independent studies are underway or planned to try to pinpoint the number of miners who have the disease, as well as the causes.
A mining disaster in slow motion

Jess Bishop, a black lung victim, takes his last breaths while his sons — also coal miners — keep vigil in Logan County, W.Va., in 1976. The disease spiked in the 1960s and ’70s but then plummeted with the passage of mine safety laws.
Courtesy of Earl Dotter
hide caption
toggle caption
Courtesy of Earl Dotter
Coincidentally, new federal regulations that are supposed to limit exposure to dangerous levels of coal and silica dust were fully implemented in 2016, a few months before NPR first reported the PMF epidemic. The Trump administration recently announced a “retrospective study” of the new regulations, a move that has mine safety advocates concerned, especially given the epidemic of the disease caused by mine dust.
“It would be outrageous for any undercutting of those regulations that puts miners [back] in harm’s way and subjects even more of them to this terrible disease,” says Joe Main, the former mine safety chief at the federal Mine Safety and Health Administration.
“When we think we know as much as we thought we should know about the disease, the next day [there’s] worse information,” says Main. “It shows that the depth of the disease is worse than what we knew the day before.”
Main pushed for the tougher mine dust exposure limits. His successor at MSHA is David Zatezalo, a former mining company executive.
“We are not proposing to weaken this rule,” Zatezalo tells NPR in a written statement. “We are planning to collect feedback on the rule from stakeholders, which was both a commitment previously made by MSHA, and a directive from President Trump, who strongly supports America’s miners.”
Zatezalo did not respond to requests for an interview. His agency’s formal notice for the “retrospective study” labels it a “deregulatory” action, which implies less regulation.
At a congressional hearing today in Washington, Zatezalo was asked directly about his agency’s “retrospective study” of the tougher mine dust limits imposed by the Obama administration.
“Do you plan to rollback any aspect of the 2014 respirable dust rule?” asked Rep. Bobby Scott, D-Va., the ranking Democrat on the House Committee on Education and the Workforce.

David Zatezalo, the Assistant Secretary of Labor for Mine Safety and Health, was asked about the advanced black lung epidemic at a congressional hearing in Washington, D.C., on Feb. 6, 2018.
Jingnan Huo/NPR
hide caption
toggle caption
Jingnan Huo/NPR
“I do not,” Zatezalo responded.
Zatezalo was also asked about his agency’s own description of the “retrospective study” of the new mine dust regulations as “deregulatory.”
“I can’t tell you why it was listed as a deregulatory item,” Zatezalo responded, unless, he added, that had something to do with the frequency of testing using new dust monitors.
“Each case of advanced black lung disease is an entirely preventable tragedy, and represents mine operators’ unwillingness to adequately control mine dust exposures, and safety regulators failure to set, monitor and enforce standards necessary to protect miners,” Scott said in a statement to NPR.
“MSHA should not bend to pressure from well-connected coal mine executives to roll back the regulations,” Scott added. “The Mine Safety and Health Administration (MSHA) cannot keep looking the other way while the burden of this preventable disease grows.”
The burden is clear on the walls of Ron Carson’s office at the Stone Mountain black lung clinic in St. Charles, Va. They’re lined with photographs and other mementos of clinic patients, some who died from the disease.
Carson describes a kind of mining disaster in slow motion, in which the disease takes years to develop, even though it strikes quicker now, and in which each death is solitary. He points to a half sheet of white paper tacked to his bulletin board. It shows a phrase he printed out from an article about black lung.
“Mining disasters get monuments,” Carson says, his voice softening. “Black lung deaths get tombstones. And I’ve seen many a tombstone in [the last] 28 years from black lung. And I’m seeing more now. A lot more now.”
How Trump's Funding Cuts Threaten 'Basic Health Program' Plans

When President Donald Trump, shown speaking at the White House last week, decided to stop making the “cost-sharing reduction” payments to health insurers, there were side effects. New York and Minnesota, for example, lost significant funding to a health program that covers more than 800,000 low-income residents.
Pool/Getty Images
hide caption
toggle caption
Pool/Getty Images
Comprehensive health care coverage for more than 800,000 low-income people in New York and Minnesota who pay a fraction of the typical cost of a marketplace plan may be in jeopardy, after the federal government partially cut funding this year.
The Basic Health Program, in which these consumers are enrolled, was created under the Affordable Care Act to provide another coverage option for people with incomes up to 200 percent of the federal poverty level ($24,280 for an individual in 2018) who would otherwise qualify for subsidized marketplace coverage. Only New York and Minnesota have set up such programs.
The funding dispute is tied to a high-profile decision by President Donald Trump to stop paying cost-sharing reduction subsidies, which reduce the deductibles and out-of-pocket costs for people in marketplace plans whose incomes are up to 250 percent of the federal poverty level (about $30,000 for one person). Money that would have paid for cost-sharing reduction subsidies also helps fund the Basic Health Program in New York and Minnesota.
These plans must be as comprehensive and affordable as marketplace plans, but for many they’re significantly cheaper, with monthly premiums of either zero or $20 in New York and up to $80 in Minnesota, along with a very small or no deductible, and with nominal copayments.
In November, for example, when May Brown lost her job as a produce repacker — breaking down 40-pound boxes of fruits and vegetables into 10-pound boxes for grocery stores — she also lost her job-based health coverage. On the advice of a friend, the 62-year-old signed up for MinnesotaCare this month. Her $50 monthly premium is about half what she was paying for coverage on the job.
Brown, who lives in St. Paul, says she is pretty healthy. But having this coverage, she says, gives her peace of mind.
“You never know. Life is unpredictable,” she says. “I like to have something.”
Under the Basic Health Program, the federal government is responsible for paying states 95 percent of the amount it would have paid in premium subsidies and cost-sharing reduction payments on the marketplace for these enrollees.
In December, the Department of Health and Human Services notified the two states it would withhold the cost-sharing reduction portion of the payments — nearly $300 million in the first quarter of 2018, about a quarter of the total amount expected.
Over the course of a year, the amount withheld will exceed $1 billion.
When it cut back on funding of the Basic Health Program, the administration cited its October 2017 decision to eliminate cost-sharing reduction payments to insurers.
Last month, the attorneys general of the two states filed suit to restore the federal funding.
Noting that New York’s Essential Plan, as it’s called, covers more than 700,000 low-income New Yorkers, Attorney General Eric Schneiderman said in a press release, “I won’t stand by as the federal government continues to renege on its most basic obligations in a transparent attempt to dismantle the Affordable Care Act.”
In their lawsuit, Schneiderman and Minnesota Attorney General Lori Swanson argue that, among other things, the administration’s decision to cut off CSR payments is procedurally flawed and violates its obligations under the health law. They want the court to restore the states’ Basic Health Program funding.
Regardless of the lawsuit’s outcome, officials in both states have offered assurances that the program is safe — for now.
In New York, Gov. Andrew Cuomo’s budget included sufficient funds to leave the Basic Health Program intact for this year.
Officials at the Minnesota Department of Human Services released a written statement, maintaining that “people enrolled in MinnesotaCare should feel confident in their coverage, based on current information.”
Under the health law, any state can offer coverage under the Basic Health Program. One possible reason New York and Minnesota adopted the program is because they were already covering many in the target population through Medicaid, and typically sharing the cost equally with the federal government. Under the Basic Health Program, the state’s funding responsibility drops to just 5 percent.
So what happens next year? If federal funding isn’t restored, advocates are concerned that costs may rise and coverage shrink.
“It could trigger major changes to the eligibility structure, the benefits or increases in premiums,” says Maureen O’Connell, president of Health Access MN, which helps people enroll in marketplace coverage.
Elisabeth Benjamin says she’s “really worried” about the program next year if the courts don’t order the federal government to start making payments.
Benjamin, the vice president for health initiatives at the Community Service Society of New York, an advocacy group, says there’s a snowball effect as states grapple with the delayed approval of Children’s Health Insurance Program funding for low-income kids amid continued uncertainty over federal funding for community health centers.
“It’s terrifying how much the feds can do, particularly for states like New York that are so reliant on federal funding,” Benjamin says.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Michelle Andrews is on Twitter @mandrews110.
In The U.S. Virgin Islands, Health Care Remains In A Critical State


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Why A Cancer Patient Opposes The 'Right To Try' Experimental Cancer Drugs
Michael Becker is dying from cancer. But he tells NPR’s Scott Simon that he opposes the passage of the Right To Try Act, which gives terminally ill patients access to experimental drugs.
SCOTT SIMON, HOST:
Imagine you’ve been diagnosed with cancer. You’ve been told it’s terminal. Doctors have tried everything. The only option left may be experimental, unapproved drugs. You want these drugs no matter what the risk. This week, President Trump urged Congress to pass what’s called the Right To Try Act in his State of the Union address. But many doctors, scientists and those involved in research think it may be a bad idea. Michael Becker is the former CEO of two biotech firms working to develop cancer treatments. Mr. Becker also has terminal cancer. Michael Becker joins us from Bucks County, Pa. Thanks so much for being with us.
MICHAEL BECKER: My pleasure, Scott. Thanks for having me.
SIMON: And I have to begin by asking you, how are you?
BECKER: (Laughter) Feeling pretty good. The quality of life at the moment is not too bad. And I’m happy to still be here.
SIMON: Why are you suspicious of the Right To Try Act?
BECKER: You know, I agree with President Trump that patients like me that are facing a terminal illness should have an opportunity to access experimental drugs. Fortunately, we already do. It’s the Compassionate Use mechanism for the Food and Drug Administration.
SIMON: Having read about you, you just don’t believe that this would be redundant but could be dangerous.
BECKER: Yeah. If you put the two side by side, there’s only one difference. And that is the FDA. The FDA gets taken out of the equation with the proposed legislation. The FDA is in the equation with the existing regulations. Compassionate Use process is extremely easy. Basically, go to your doctor. Find one who will agree to administer the therapy. Contact the drug company. See if they’re also willing to agree. Fill out the paperwork. And then if the FDA doesn’t object, the patient can get the treatment. And the only difference with the new legislation is that last part. The FDA is taken out of the equation.
SIMON: With respect, why care so much about the FDA if a life is hanging in the balance?
BECKER: So as a terminal cancer patient, I would, you know, obviously love to try something that’s going to prolong my life or cure my cancer. The reality is that that’s a very, very small statistic in terms of drug development discovery. Only 5 percent of drugs that go through phase one development actually go on to be approved. So you’re talking about giving people medications that, in historical context, have only had a 5 percent chance of actually working at the end of the day. And then you’re exposing these patients to, potentially, additional toxicities that could accelerate their death or cause additional problems for them.
SIMON: I’m sure you’ve run all this through your mind. Why not – I was about to ask you, why not let the patient decide? Why not let you decide?
BECKER: Well, the problem becomes that you have a lot of false hope as a terminal cancer patient. You want to cling to anything that’s going to sound like it’s an opportunity to live longer or have a better quality of life. And that hope can sometimes cover up the realities of some of the more sinister aspects of getting a drug, which are things go wrong. So I could take a drug that was purported to help me, and it may actually make my condition worse. It could create other difficulties for me. And then my quality of life may be even worse than it was originally. That’s what I would fear as a – or what I do fear as a patient.
SIMON: Yeah. And would it potentially take advantage of people at their most vulnerable?
BECKER: Absolutely. I can’t tell you how many times I see miracle cures and herbal remedies and everything from unsolicited emails to Internet ads, you know, talking about cures and treatments for cancer. If you take the FDA as the policeman out of that equation, I’m scared to death as to what cancer patients or other patients facing terminal illnesses may be subjected to.
SIMON: Well, Mr. Becker, good luck to you. We are so grateful to speak with you. Thank you so much.
BECKER: Thank you, Scott.
Copyright © 2018 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Indiana Adds Work Requirement To Medicaid, Will Block Coverage If Paperwork Is Late

{kind=link}
Health and Human Services Secretary Alex Azar announced federal approval for changes to Indiana’s Medicaid program Friday in Indianapolis.
Mandel Ngan/AFP/Getty Images
hide caption
toggle caption
Mandel Ngan/AFP/Getty Images
Indiana on Friday became the second state to win federal approval to add a work requirement for adult Medicaid recipients who gained coverage under the Affordable Care Act. A less debated provision in the state’s new plan could lead to tens of thousands of people losing coverage if they fail to complete paperwork documenting their eligibility for the program.
The federal approval was announced by Health and Human Services Secretary Alex Azar in Indianapolis.
Medicaid participants who fail to promptly submit paperwork showing they still qualify for the program will be locked out of enrollment for three months, according to updated rules.
Since November 2015, more than 91,000 enrollees in Indiana were kicked off Medicaid for failing to complete the eligibility redetermination process, according to state records. The process requires applicants to show proof of income and family size, among other things, to see if still qualify for the coverage.
Until now, these enrollees could simply reapply anytime. Although many of those people likely weren’t eligible anymore, state officials estimate about half of those who failed to comply with its re-enrollment rules still qualified for Medicaid coverage.
Indiana expanded Medicaid starting in February 2015, providing coverage to 240,000 people who were previously uninsured. The change helped lower the state’s uninsured rate from 14 percent in 2013 to 8 percent last year.
The HHS approval of the state’s waiver extends the program, which was expiring this month, through 2020.
The new lockout builds on one Indiana already had in place state for people who failed to pay monthly premiums and had annual incomes above the federal poverty level, or about $12,200 for an individual. Locked-out people are barred for six months from coverage. During the first two years of the experiment, about 10,000 Indiana Medicaid enrollees were subject to the lockout for failing to pay the premium for two months in a row, according to state data. In addition, more than 25,000 enrollees were dropped from the program when they failed to make the payments, although half of them found another source of coverage – usually through their jobs.
Another 46,000 were blocked from coverage because they failed to make the initial payment.
“The ‘lockout’ is one of the worst policies to hit Medicaid in a long time,” says Joan Alker, executive director of the Georgetown University Center for Children and Families. “Forcing people to remain uninsured for months because they missed a paperwork deadline or missed a premium payment is too high a price to pay. From a health policy perspective it makes no sense because during that six-month period, chronic health conditions such as hypertension or diabetes are just likely to worsen.”
Indiana’s Medicaid expansion is being closely watched in part because it was spearheaded by then-Gov. Mike Pence, now vice president, and his top health consultant, Seema Verma, who heads the federal Centers for Medicare & Medicaid Services.
The expansion, known as Healthy Indiana, enabled non-disabled adults access to Medicaid. It has elicited criticism from patient advocates for complex and onerous rules that require these poor adults to make payments ranging from $1 to $27per month into health savings accounts or risk losing their vision and dental benefits or even all their coverage, depending on their income level.
Indiana Medicaid officials say they added the newest lockout provision in an effort to prompt enrollees to get their paperwork submitted in time. The state initially requested a six-month lockout.
“Enforcement may encourage better compliance,” the state officials wrote in their waiver application to CMS in July.
The new rule will lead to a 1 percent cut in Medicaid enrollment in the first year, state officials said. It will also lead to a $15 million reduction in Medicaid costs in 2018 and about $32 million in savings in 2019, the state estimated.
The number of Medicaid enrollees losing coverage for failing to comply with redetermining their eligibility has varied dramatically each quarter from a peak of 19,197 from February 2016 to April 2017 to 1,165 from November 2015 to January 2016, state reports show. In the latest state report, 12,470 enrollees lost coverage from August to October 2017.
The Kentucky Medicaid waiver approved by the Trump administration in January included a similar lockout provision for both failing to pay the monthly premiums or providing paperwork on time. Penalties there are six months for both measures. But the provision was overshadowed because of the attention to the first federal approval for a Medicaid work requirement.
Like Kentucky, Indiana’s Medicaid waiver’s work requirements, which mandate adult enrollees to work an average of 20 hours a month, go into effect in 2019. But Indiana’s waiver is more lenient. It exempts people age 60 and over and its work-hour requirements are gradually phased in over 18 months. For example, enrollees need to work only five hours per week until their 10th month on the program.
Most Medicaid adult enrollees do work or go to school or are too sick to work, studies show.
Indiana also has a long list of exemptions and alternatives to employment. This includes attending school or job training, volunteering or caring for a dependent child or disabled parent. Nurses, doctors and physician assistants can give enrollees an exemption due to illness or injury.
Three patient advocacy groups have filed suit in federal court seeking to block the work requirements.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Phil Galewitz is a senior correspondent for KHN.