E-Cigarettes Likely Encourage Kids To Try Tobacco But May Help Adults Quit

Vapor from e-cigarettes contains toxins, although fewer than conventional cigarettes.
mauro_grigollo/Getty Images/iStockphoto
hide caption
toggle caption
mauro_grigollo/Getty Images/iStockphoto
Kids who vape and use other forms of e-cigarettes are likely to try more harmful tobacco products like regular cigarettes, but e-cigarettes do hold some promise for helping adults quit.
That’s according to the National Academies of Science, Engineering and Medicine, which published a comprehensive public health review of more than 800 studies on e-cigarettes on Tuesday.
“There is conclusive evidence that most products emit a variety of potentially toxic substances. However the number and intensity is highly variable,” says David Eaton, who heads the committee that wrote the report. He is also the dean and vice provost of the graduate school of the University of Washington, Seattle.
“In some circumstances, such as their use by nonsmoking adolescents and young adults, their adverse effects clearly warrant concern. In other cases, such as when adult smokers use them to quit smoking, they offer an opportunity to reduce smoking-related illness.”
In fact, 15 of the studies NAS reviewed found that when teens and young adults use e-cigarettes, they are more likely to try regular tobacco within a year.
“We found that kids who tried e-cigarettes, hookah, or smokeless tobacco or cigars — any non-cigarette tobacco product — were all twice as likely to try cigarettes a year later, compared to kids who hadn’t used any of those other tobacco products,” says Shannon Lea Watkins, a public policy researcher at University of California, San Francisco. Watkins and her colleagues also found that the effects of using non-cigarette products compound: “Kids using two or more non-cigarette products were four times as likely to report using cigarettes a year later.”
However, it is not yet known how much tobacco they use on a regular basis and whether it became a habit. More long-term studies are needed.
The NAS report also indicates that there is some evidence that e-cigarettes may help adults already smoking regular cigarettes quit, but only if they switch exclusively to e-cigarettes.
Eaton emphasized that there is insufficient evidence on whether e-cigarettes work as well as either no treatment or FDA-approved smoking-cessation treatments, such as nicotine patches or gum, to get smokers to quit.
E-cigarettes are still fairly new and are largely unregulated. The were introduced only in 2003 as an alternative to tobacco-containing cigarettes, which is why the government requested that the analysis be conducted.
The report found that most e-cigarettes contain nicotine, even if they are marketed as flavored like bubble gum and potpourri.
The report also found that emissions from e-cigarettes do contain some harmful byproducts like metal, but far less than conventional cigarettes.
“Conventional cigarettes burn, and in the process of burning tobacco, a large number of fairly toxic chemicals are generated in the tobacco smoke,” Eaton says. So there are more adverse health effects related to these combustible products.
However, a recent national survey suggests adults do not believe that e-cigarette vapor is toxic.
Food and Drug Administration Commissioner Scott Gottlieb says the report “helps identify areas that need further study to better understand the net public health impact of e-cigarettes … . We need to put novel products like e-cigarettes through an appropriate series of regulatory gates to fully evaluate their risks and maximize their potential benefits.”
FDA commissioned the report at the direction of Congress to evaluate evidence of health effects of e-cigarettes after it delayed proposed regulations last year.
Matthew Myers, president of the Campaign for Tobacco-Free Kids, issued a statement expressing disappointment that the FDA has not acted quickly enough to regulate these products. “This report shows what happens when a new product is introduced without meaningful government oversight. It demonstrates why the FDA should fully and aggressively implement the overdue e-cigarette regulations that took effect in August 2016,” it says.
The national academies report calls for more studies.
California Bill Would Mandate On-Campus Access To Abortion Pills

If a bill in the California Legislature become law, campus health centers at public universities would be required to provide abortion pills.
Phil Walter/Getty Images
hide caption
toggle caption
Phil Walter/Getty Images
In California, the state Senate is considering legislation that would ensure that students at four-year public universities in California have access on campus to medication for abortions.
Sen. Connie Leyva introduced the bill, SB 320, in February 2017. It would require all health centers within the University of California and California State University systems to stock the drugs prescribed for medication abortion and ready their campus health clinics to provide them by 2022.
Medication abortion involves two drugs, mifepristone and misoprostol, that a woman can take at a clinic or at home to terminate pregnancies less than 10 weeks along.
The campaign for the bill began at University of California, Berkeley in 2016, when the student government passed a resolution urging the health center there to include medication abortion in its services.
Adiba Khan, co-founder of Students United for Reproductive Justice and the author of the resolution, noticed that the student health service offered 18 forms of contraception, but not abortion. She was also influenced by fellow students’ experiences. “I was able to meet a few peers who attempted to get an abortion through the student health center, and they faced a lot of hurdles, mostly bureaucratic, before they were able to get an abortion,” Khan says.
Members of the group met with the health center administration as well as university leaders to try to make medication abortion available at Berkeley’s health center, but it didn’t happen.
“When they were denied, they brought the issue to us, and I thought that this was something that young women should have access to, because it is their constitutional right,” says Leyva. The Women’s Foundation of California Women’s Policy Institute stepped in to help draft the legislation.
The bill is moving ahead in the California Legislature even as other states have taken steps to limit access to medication abortion.
The Oklahoma Legislature passed a bill that was signed into lawin 2014 that set a strict protocol for the drugs involved in medication abortion; it was initially overturned in the state courts, then upheld and was overturned again in 2017. In Louisiana, a law requiring that all aborted tissue be buried or cremated — an impossible task in the case of medication abortion — is currently suspended as the state court tries it. And as of last fall, the Missouri health department requires any facilities providing medication abortion to contract with an OB-GYN who can be on call around the clock to personally handle any complications.
Opponents of the bill in California are unsure that public university health centers should provide medication abortions. Anna Arend, the Northern California Regional Coordinator for Students for Life of America, testified during the Senate education committee hearing on behalf of student groups across California that oppose the bill. “These students have formed a coalition to oppose SB 320 due to the horrible realities of RU 486, the abortion by medication technique, and the dangers that it would bring to their campus. And the simple fact that abortion pills are not a factor in student success,” Arend said.
California is alone in considering a measure like this, but the legislative push is in line with the state’s previous policies, says Elizabeth Nash, a senior state issues analyst at the Guttmacher Institute. The state also requires all health insurers to provide abortion coverage and sets no waiting period for abortion procedures.
The California Senate committees on health, education and appropriations committee have each approved the bill. Next, the bill will move to the Senate floor for a vote, which is expected by the end of January.
As for funding the abortion services, SB 320 doesn’t specify the use of any state or university money. A private consortium that includes the Women’s Foundation of California, Tara Health Foundation and a private donor has agreed to pay for implementation. The estimated cost is about $14 million, says Dr. Ruth Shaber, president of Tara Health Foundation. That figure “includes the training, any type of new equipment that’s necessary, and training in the processes, billing for the procedure, and making sure that the clinics are really prepared to implement the procedure and to offer the care well,” she says.
Campus health clinics currently provide reproductive health care like testing for sexually transmitted diseases and contraceptives. The risk of complications from medication abortion is low. A University of California, San Francisco study of more than 50,000 abortions provided between 2009 and 2010 found that 0.31 percent of medicated abortions resulted in major complications.
Still, the transition to providing the abortion procedure at campus health clinics may give some people pause. “You can say, well, look at the percentages, but if they’re happening to you, it’s not a fun thing in medicine for you and your patient,” says Dr. Richard Boucher, who directs student Health Services at California State University Fullerton.
Boucher also cited the issue of whether individual providers would feel comfortable administering the procedure, an issue that is in the spotlight now. On Jan. 18, the federal Department of Health and Human Services announced the creation of a Conscience and Religious Freedom Division that would offer protection to medical providers who refuse to participate in certain services, like abortion, on religious or moral grounds.
Even if the California Senate votes in favor of the bill, it has a ways to go before becoming law. The legislation would have to be passed by the state Assembly and be signed by the governor.
Part Of Oregon's Funding Plan For Medicaid Goes Before Voters

A sign in support of Oregon’s Measure 101 is displayed by a homeowner along a roadside in Lake Oswego, Ore. Tuesday’s special election puts decisions over how the state funds Medicaid in voters’ hands.
Gillian Flaccus/AP
hide caption
toggle caption
Gillian Flaccus/AP
Oregon is in a battle royal over how to pay for expanded Medicaid.
The fight revolves around Measure 101, a ballot initiative that you have to go back a few years to understand.
During the 1990s, Oregon’s then-governor, Dr. John Kitzhaber, had a background in health care — he’d worked as an emergency room doctor. His legacy in the state includes the expansion of health insurance for the poor, an idea he managed to sell to both Democrats and Republicans.
So when President Barak Obama proposed expanding Medicaid under the Affordable Care Act, Oregon lawmakers on both sides of the aisle embraced it. As a result, some 95 percent of Oregonians now have health insurance. That’s among the highest rates in the nation.
But now the federal government is trimming its contribution to Medicaid. And legislatures all around the U.S. are scrambling to find money to replace those federal payments.
In Oregon last summer, Democrats joined with Republicans, hospital owners and health insurance CEOs to come up with a tax package that would fund the Medicaid expansion. And hospitals and insurance companies agreed to the plan, though they are on the hook for many of the included taxes.
Here’s where the wrinkle comes: Under state law in Oregon, voters can use the initiative process to collect signatures and force a public vote on any new tax. And that’s what state Rep. Julie Parrish did.
Parrish and others managed to get “Measure 101” on Oregon’s Tuesday ballot — putting part of the Medicaid tax package passed last summer into the hands of voters. If it succeeds not much will happen — the tax package will continue to fund Medicaid expansion. But if it fails, Oregon’s legislature will have to go back to the drawing board and come up with a new way to pay for the health care of its poorest residents and others who rely on Medicaid.
Parrish is a Republican state legislator whose family was on Medicaid when she was a child.
But she doesn’t like the tax package.
“This is about a fundamental disagreement that taxing other people’s insurance is the way to fund Medicaid,” she says. Parrish says the funding package Oregon came up with is inequitable because it doesn’t apply to big corporations and unions. Instead, she says, it hurts the little guy — people who couldn’t afford to hire lobbyists.
“Small businesses — Mom and Pop businesses,” she says, ticking off the groups she thinks would unfairly bear the tax burden under the state’s plan. “Individuals who have to buy their own [health insurance].”
Parrish thinks Medicaid would be better-funded in Oregon with something like a cigarette tax increase — although it’s not clear that would generate enough money or garner enough votes to pass.
Cedric Hayden is a Republican representative from Falls Creek, Ore. He’s a dentist who accepts Medicaid patients and runs a charitable health clinic in Lane County. He’s also a member of Parrish’s Stop Healthcare Taxes committee — the group that collected enough signatures to put Measure 101 on the ballot.
Hayden says if he and other members of his committee had been against funding Medicaid altogether, they could have insisted the legislature’s entire funding plan be put up for a public vote.
“We did not,” he points out.
Instead, if approved, Measure 101 would ratify the Medicaid expansion in Oregon that the state legislature approved last summer. But if Measure 101 fails, a part of that tax package will be eliminated. A no-vote would eliminate the .7 percent increase to an existing tax on hospitals that the state legislature wants. And it would also stop a 1.5 percent tax on health insurance contracts.
It’s unclear how the passage of Measure 101 would affect consumers. That’s because, on the one hand, any new taxes would likely be passed on to consumers. But on the other hand, Measure 101 funds a program that saves consumers of health care $300 a year.
Some Republicans in the state want a ‘no’ vote. They don’t like the new tax and they don’t trust the Oregon Health Authority with the money. They say the OHA wasted millions of dollars on things like Medicaid overpayments and CoverOregon — the webpage that sells Obamacare insurance.
On the ‘yes’ side are all kinds of advocacy groups and the vast majority of Oregon’s health organizations. They say 48 other states have some form of this tax package to pay for Medicaid.
“The alternative of lack of coverage — we’re talking kids, seniors, people with disabilities — is unacceptable,” says Andy Van Pelt, the executive director of the Oregon Association of Hospitals and Health Systems.
He says it’s cheaper to treat people with health insurance, than to treat them without insurance, when they turn up sick in emergency rooms anyway.
“There’s a real possibility that people could lose their coverage. It will just destabilize the Medicaid program for hundreds of thousands of people and that would be utter chaos,” Van Pelt says.
While the Donald Trump administration hasn’t managed to repeal the Affordable Care Act, it has taken several steps to dismantle it. For example, Americans are no longer legally required to buy health insurance.
The effect of Measure 101 on Oregon’s Medicaid expansion remains to be seen. If it fails, state lawmakers will spend the next couple of months searching for new ways to pay for Medicaid expansion.
Tax Credit Aims To Boost Availability Of Paid Family Leave, But Will It Work?

The new tax credit sidesteps a common pitfall in the eyes of many Republicans by avoiding a mandate — it doesn’t require employers to provide paid family leave. Instead, the law offers firms a financial incentive to provide the coverage.
FatCamera/Getty Images
hide caption
toggle caption
FatCamera/Getty Images
Tucked into the new tax law is a provision that offers companies a tax credit if they provide paid family and medical leave for their lower-wage workers.
Many people support a national strategy for paid parental and family leave, especially for workers who are not in management and are less likely to get that benefit on the job. But consultants, scholars and consumer advocates alike say the new tax credit probably won’t encourage many companies to take the plunge.
The tax credit, proposed by Sen. Deb Fischer, R-Neb., is available to companies that offer at least two weeks of paid family or medical leave annually to workers; but two key criteria must be met. The workers must earn less than $72,000 a year and the leave must cover at least 50 percent of their wages.
If the company contributes at the half-wage level, it will receive a tax credit equal to 12.5 percent of the amount it pays to the worker. The tax credit will increase on a sliding scale if the company pays more than 50 percent of wages. It could go up to a maximum credit of 25 percent of the amount the employer paid for up to 12 weeks of leave.
Payments to full- and part-time workers taking family leave who’ve been employed for at least a year would be eligible for the employer’s tax break. But the program, which is designed to test whether this approach works well, is set to last just two years — ending after 2019.
Aparna Mathur, a resident scholar in economic policy studies at the American Enterprise Institute, says the new tax credit sidesteps a common pitfall in the eyes of many Republicans by not requiring employers to provide paid leave. The tax credit also is appropriately aimed at lower-wage workers — who are the ones least likely to have access to paid leave, says Mathur, who co-authored a recent report on paid family leave.
Still, she says, the provision is not a big enticement to companies.
“Providing this benefit is a huge cost for employers,” Mathur says. “It’s unlikely that any new companies will jump on board just because they have a 12.5 to 25 percent offset.”
That view is shared by Vicki Shabo, vice president for workplace policies and strategies at the National Partnership for Women & Families, an advocacy group. Shabo says the provision will primarily benefit workers at companies already offering paid family leave. The new tax credit “just perpetuates the boss lottery,” she says.
Heather Whaling says her 22-person public relations company, Geben Communication in Columbus, Ohio, probably qualifies for the new tax credit. But she doesn’t think it’s the right approach.
Whaling, who is president of the PR firm, says Geben already provides up to 10 weeks of paid leave at full pay for new parents. So far, four employees have taken leave; by divvying up their work to other team members and hiring freelance help, the firm has been able to get by.
“It is an expense,” Whaling says, “but if you plan and budget carefully it’s not cost-prohibitive.”
The tax credit isn’t big enough, she says, to be a strong incentive. Besides, “having access to paid family leave shouldn’t be luck of the draw — it should be available to every employee in the country.”
Still, the tax credit may be appealing to companies that have already been leaning toward adding a paid family and medical leave benefit, says Rich Fuerstenberg, a senior partner at Mercer, a benefits consulting firm.
By defraying some of the cost, the tax credit might help “tip them over” into offering paid leave, he says. But “I’m not even sure I’d call it the icing on the cake,” Fuerstenberg says. “It’s like the cherry on the icing.”
Only 15 percent of private-sector and state and local government workers had access to paid family and medical leave in 2017, according to the Bureau of Labor Statistics’ National Compensation Survey. Eighty-eight percent, however, had access to unpaid leave.
Generally, under the federal Family and Medical Leave Act, employers with 50 or more workers must allow eligible employees to take unpaid leave for up to 12 weeks annually, for specified reasons.
These reasons include the birth or adoption of a child, caring for your own or a family member’s serious health condition, or leave for military caregiving or deployment. An individual’s job is protected during such leaves.
Erik Rettig, an expert on family leave policies at the Small Business Majority, which advocates for those firms on national policy, says a tax credit, claimed at the end of the year, is unlikely to encourage small businesses to offer paid family and medical leave.
“It isn’t going to help the family business that has to absorb the costs of this employee while they’re gone,” Rettig says.
A better solution, according to Shabo and others, would be to provide a paid family leave benefit that’s funded by employer and/or employee payroll contributions. Sen. Kirsten Gillibrand, D-N.Y., and Rep. Rosa DeLauro, D-Conn., last year reintroduced such legislation. Their bill would guarantee workers, including those who are self-employed, up to 12 weeks of family and medical leave with as much as two-thirds of their pay.
A handful of mostly Democratic states — including California, New Jersey, Rhode Island and New York — have similar laws in place, and a program in the District of Columbia and Washington state will begin in 2020.
“We know from states that this approach works for both employees and their bosses,” Shabo says.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Michelle Andrews is on Twitter @mandrews110.
In Trump's First Year, Anti-Abortion Forces Make Strides

Opponents of abortion rights rallied outside the U.S. Supreme Court during The March for Life on Friday in Washington, D.C.
Ricky Carioti/The Washington Post/Getty Images
hide caption
toggle caption
Ricky Carioti/The Washington Post/Getty Images
As a presidential candidate, Donald Trump promised abortion opponents four specific actions to “advance the rights of unborn children and their mothers.”
One year into his presidency, three of those items remain undone. Nevertheless, opponents of abortion have made significant progress in changing the direction of federal and state policies.
Indeed, on Friday, as anti-abortion protesters gathered in Washington for the 45th annual March for Life, the Trump administration announced two new policies. One is a letter to states aimed at making it easier for them to exclude Planned Parenthood facilities from their Medicaid programs; the other is a proposed regulation to allow health care providers to refuse to perform services that conflict with their “religious or moral beliefs.”
“In my administration, we will always defend the very first right in the Declaration of Independence, and that is the right to life,” President Trump said in a video address from the Rose Garden to the marchers.
Marjorie Dannenfelser, president of the anti-abortion group the Susan B. Anthony List, led the Trump campaign’s Pro-Life Coalition. The then-candidate said he was committed to “nominating pro-life justices to the U.S. Supreme Court,” which happened with the nomination and confirmation of Justice Neil Gorsuch in April.
Despite many attempts, Congress did not pass a federal ban on abortions occurring after 20 weeks, didn’t cut off Planned Parenthood’s federal funding and didn’t write into permanent law the Hyde Amendment, which bans most federal abortion funding but needs annual renewal.
Still, there was progress on scaling back abortion and, in some cases, access to contraception at the federal level.
The administration made myriad changes. It reinstituted and expanded the “Mexico City” policy, which forbids funding of international aid programs that “perform or promote” abortion. It issued rules aimed at allowing religious-affiliated and other employers to not offer contraceptive services if they have a “religious belief” or “moral conviction” against them, although federal courts have blocked the new rules from being implemented. And just last week the administration created a new “conscience and religious freedom” division in the Department of Health and Human Services’ Office of Civil Rights. That new division is designed to enforce both existing laws protecting the rights of conscience for medical personnel as well as the new regulations.
Most important, according to many in the anti-abortion movement, the president nominated and the Senate confirmed a dozen and a half federal district court and appeals court judges who are considered likely to rule in their favor.
Abortion rights supporters concede that while the priorities on their opponents’ wish list weren’t accomplished, plenty still happened.
“This administration is the worst we’ve ever seen for women and families,” says Kaylie Hanson Long of NARAL Pro-Choice America in a statement. “Its attacks on reproductive freedom are relentless, under the radar, and aren’t supported by the majority of Americans who believe abortion should remain legal.”
Dannenfelser says one of the biggest changes is the number of anti-abortion advocates now working in the Department of Health and Human Services in key roles. “I can say there is more unity in this administration than there has been in any presidency on this,” she says.
Abortion opponents know their biggest obstacle is the Senate, where they don’t have the 60 votes required for most legislation. “Without making advances in the Senate, it’s going to be really tough,” says Dannenfelser.
Meanwhile, outside Washington, states continued their efforts to restrict access to abortion and family planning. States have passed 401 separate measures since Republicans took over most state legislatures in 2011, according to the Guttmacher Institute, a reproductive rights research and advocacy group.
During 2017, 19 states enacted 63 separate restrictions, says Elizabeth Nash, who tracks state legislation for Guttmacher. Among the notable laws was one in Ohio to outlaw abortions of fetuses diagnosed with Down syndrome. Arkansas and Texas passed laws to ban “dilation and evacuation” abortions, a procedure that uses suction and medical instruments to remove the fetus and is the most common procedure for abortion after the first trimester of pregnancy. Both bans have been blocked by federal courts.
Some of the new restrictions came from states that haven’t been active on the issue in recent years. A Wyoming law requiring ultrasounds to be offered to pregnant women seeking an abortion was that state’s first in 30 years, Nash says.
But 2017 was also notable for states seeking to widen or ensure access to abortion and other reproductive services. For example, Delaware passed a law enshrining abortion rights, while Oregon and New York require private health plans to cover abortion without patients’ cost sharing. Legislators in California, which has a long history of protecting abortion rights, have been pushing a bill that would require public universities to provide abortion pills to female students who are less than 10 weeks pregnant. The bill stalled last year, but it is being picked up again this year.
As a result, says Nash, “we are really living in a bifurcated country. The states that are progressive are looking to protect access” to abortion and contraception. “The states that are conservative are looking to restrict it.”
In other words, a nation that looks a lot like it did 45 years ago, when the Supreme Court legalized abortion nationwide in Roe v. Wade.
Kaiser Health News is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation. California Healthline reporter Ana B. Ibarra contributed to this story.
Cancer Patients Get Little Guidance From Doctors On Using Medical Marijuana

Like most patients, Murphy’s first step was to ask her oncologist. Murphy said she loved her doctor and care team at Mount Auburn Hospital in Cambridge, but they had no advice to offer on medical marijuana.
“They said ‘yes, you can look into it,’ ” she said. “But I felt sad because you’re so lost and you’re so sick and this is so not your area of expertise, that it was very upsetting to me to not get direction one way or the other.”
Only about 1 percent of Massachusetts’ 25,000 doctors are registered with the state and allowed to legally prescribe marijuana. And only a fraction of those know much about cancer care.
Last June, the Massachusetts Medical Society approved a new online curriculum for medical marijuana. Six months later, only 27 medical professionals have taken the section on cancer care and cannabis. Both the Dana-Farber Cancer Institute and the Massachusetts General Hospital Cancer Center said they had no experts on staff to speak with us for this report.
Murphy eventually found her way to Dr. Jordan Tishler, who runs medical cannabis clinics in Cambridge and Brookline, called inhaleMD.
Tishler, a former emergency room physician and music producer, said he treats cannabis like any other therapy, meeting with new patients for an extended conversation and follow-ups. But some cannabis prescribers, he said, just want to sign the state paperwork and move on.
“By and large, physicians are simply saying, ‘yes, you can have it,’ and then stopping the conversation there,” he said.
Tischler explained that medical centers — particularly those that take federal funding — are in a tight spot because federal law still classifies cannabis as an illegal drug, despite its legalization for medical purposes, at a minimum, in 30 states and the District of Columbia.
“Most of those institutions are prohibited and/or afraid of the prohibitions from the federal government, so have opted not to pursue this within their domain,” Tischler said. He set up his private clinic so he could operate outside of those systems, though he said he receives referrals from all the major hospitals.
In early January, Attorney General Jeff Sessions told the nation’s U.S. attorneys to resume aggressively pursuing marijuana growers and distributors, even in states where marijuana has been legalized. It’s not clear yet what that will mean for Massachusetts’ medical marijuana system, but a few days later, Massachusetts U.S. Attorney Andrew Lelling said he cannot and will not rule out prosecuting state-sanctioned marijuana businesses.
As it currently stands, authorized doctors like Tishler have to fill out an online form with the state, which the patient then submits with a $50 check to request a license. Tishler said the process used to take several weeks, but now the state usually issues a medical card within three or four days of receiving a request.
Then, the patient has to take that license to one of the state-approved medical marijuana dispensaries, which offer a wide array of products containing cannabis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
New England Treatment Access in Brookline, Mass., is located in a former branch of Brookline Bank.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
New England Treatment Access, or NETA, whose Brookline dispensary is housed in an old bank building, sells 130 products. Garden Remedies, whose dispensary is in Newton about a block from a Whole Foods, sells 50 items, including bath bombs, lip balm and marijuana-infused honey they make themselves in their cultivation facility.
Murphy said she would have been overwhelmed by those choices if she hadn’t had a doctor like Tishler advising her on what to take. Tishler said he tells cancer patients, for example, that they should avoid using novelty items like bath bombs and creams. They may be fun, but they won’t help with nausea or pain, he says.
Murphy didn’t like the idea of edibles. She had young children at home and was anxious they might find a brownie too tempting to pass up.
Tishler warned his patients against getting advice on care either from the Internet — which he said is loaded with misinformation — or from the counter folks at the dispensaries, who are trained in their products but are not legally allowed to give out medical advice.
“They’re doing the best they can, but fundamentally, they’re salespeople,” he said. “Their level of training, I often say, is about the level of a Starbucks barista. So, I tell patients, ‘look, if you wouldn’t ask your coffee guy about your health, probably you shouldn’t ask these guys, either.’ “
Dispensing Experimental Wisdom
Dr. Karen Munkacy, president and CEO of Garden Remedies, said her staff generally recommends that someone with nausea use a vape pen, to get a quick effect from the cannabis, and then, if they need something longer-lasting, take an edible.
“Inhalation medical marijuana works within a few minutes, and so, now their nausea and vomiting is under control,” she said. “If they want to get a good night’s sleep they’re going to need to get something that they ingest because it’s going to last longer. They won’t wake up vomiting in the middle of the night.”
Munkacy started her company after her own bout with chemo-induced nausea. She was treated for breast cancer a decade ago in New Jersey, where medical marijuana was illegal.
“It was months of feeling a thousand times worse than any flu I’ve ever had,” said Munkacy, who at the time was an anesthesiologist with a 2-year-old son. “Before [medical cannabis] became legal, people would have to choose between breaking the law and suffering terribly.”
Convinced that medical marijuana could help other people avoid her misery, Munkacy worked to help get legalized medical marijuana on the ballot in Massachusetts in 2012, and said she is now committed to educating patients who come to her dispensary.
“Our goal is that when patients leave, they’ve learned everything they need to know,” she said.
Cannabis is generally very safe, Tishler said, as long as patients buy their medical marijuana from a dispensary, because state requirements ensure a safe, consistent product. There is no lethal dose, and the worst side effect for most of his patients, he said, is an unwanted feeling of getting high when they’ve taken too much.
Norton Arbelaez, director of government affairs for NETA, which also has a dispensary in Northampton, said that safety profile means patients can afford to be a little imprecise about what kind of marijuana they use and how much they get.
“There is some room here for the patient themselves to experiment and see what’s right for them,” he said.
In the end, that’s what Murphy did. She experimented. She tried a few joints and smoked a few times with a pipe.
She had already spent $700 paying Dr. Tishler, getting her $50 state license and buying the cannabis, so she didn’t want to invest more in the vaporizer Dr. Tishler recommended.
But even just those few weeks of occasional smoking made a big difference, Murphy said.
“It made me feel like I had an appetite for the first time in probably six months,” she said. “Instead of lying around thinking about how sick I felt all the time — which was not my personality, which was very upsetting to my whole family — I was up and cooking, which was not anything I had done since I hadn’t felt well.”
Murphy, who is now cancer-free, hasn’t smoked since her treatments ended in the summer of 2016. She still wishes patients didn’t have to work so hard to get the information they need about medical marijuana.
Younger Patients and Cannabis
The situation for children and teens with cancer is a little different than for adults, according to Prasanna Ananth, a pediatric oncologist at Yale Cancer Center. Ananth published a study in early December showing that an overwhelming majority of pediatric oncologists, nurses and other health care professionals in Massachusetts, Illinois and Washington state were willing to consider medical marijuana for children with cancer — particularly for those with advanced illness.
There are decades of research showing the potential dangers of marijuana for children and teenagers, but almost none into its possible benefits for young cancer patients, she said.
“Our calculus shifts when we’re talking about children facing serious, life-threatening illness,” Ananth said. “Health care providers must weigh their desire to provide compassionate care for their patients against limited scientific evidence to support use of medical marijuana by children.”
In her survey, nearly 1 in 3 pediatric oncology experts said they had been asked about medical marijuana by at least one patient.
Ananth said she would prefer to talk with her patients about their marijuana use than not know that they’re using it.
“Especially for the purpose of knowing what my patients are on and what the medical marijuana might interact with, it is important for us to maintain open lines of communication,” she said.
With Legal Pot Shops, Medical Use May See Boost
It’s not clear how Massachusetts’ medical marijuana system will change later this year when recreational marijuana sales are set to begin. Patients will pay 20 percent less than recreational users because they won’t have to pay taxes on their cannabis.
But Munkacy said she believes many more people will start using cannabis for their medical problems once recreational use becomes legal.
They may not have wanted to give their name to the state for a license, but the reduced restrictions and added legitimacy of legal marijuana will give them the push they need to start using it, Munkacy explained.
“I’m thinking there’s going to be a lot of people who will no longer have to buy their medicine on the black market.”
The first version of this story appeared on WBUR’s CommonHealth. Karen Weintraub spent 20 years in newsrooms before becoming a freelance writer in January 2010. She contributes to CommonHealth.
When A Tattoo Means Life Or Death. Literally.

{kind=link}
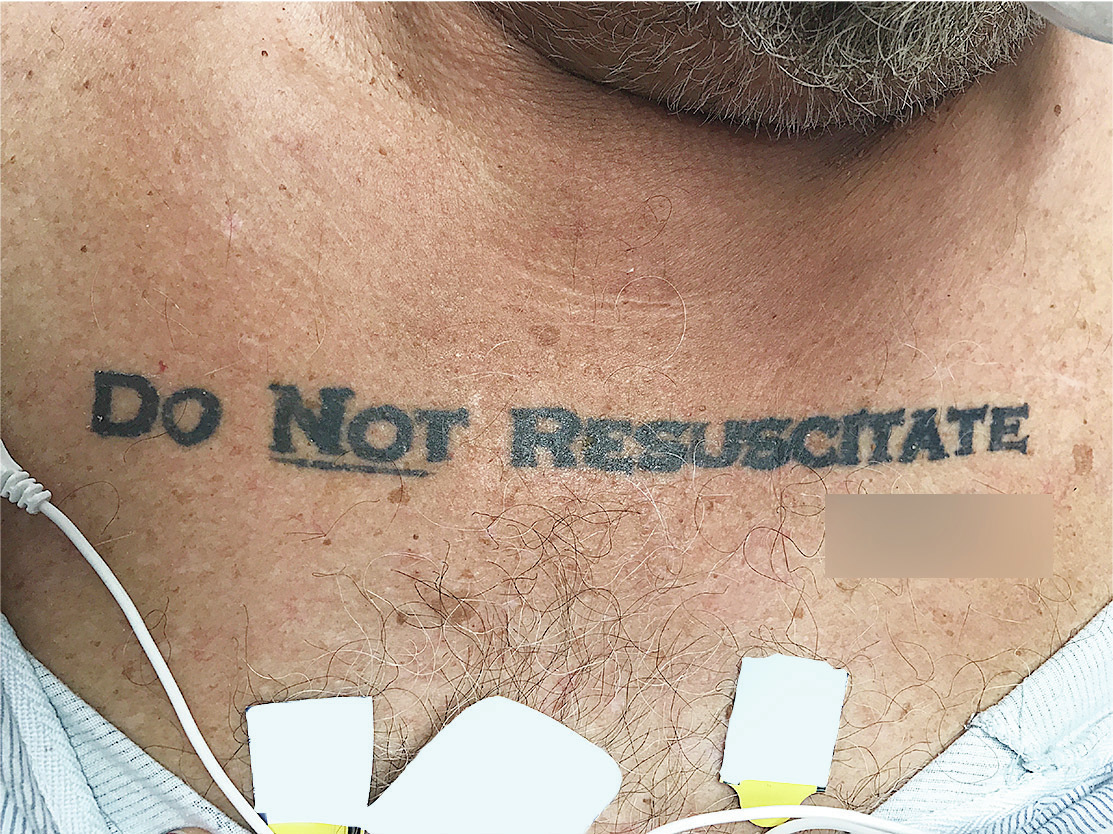
Doctors in Miami found that a man’s tattoo expressing his end-of-life wishes was more confusing than helpful.
Gregory Holt/The New England Journal of Medicine
hide caption
toggle caption
Gregory Holt/The New England Journal of Medicine
The man was unconscious and alone when he arrived at University of Miami Hospital last summer. He was 70 years old and gravely ill.
“Originally, we were told he was intoxicated,” remembers Dr. Gregory Holt, an emergency room doctor, “but he didn’t wake up.”
“He wasn’t breathing well. He had COPD. These would all make us start to resuscitate someone,” says Holt. “But the tattoo made it complicated.”
The tattoo stretched across the man’s chest. It said “Do NOT Resuscitate.” His signature was tattooed at the end.
“We were shocked,” remembers Holt. “We didn’t know what to do.”
The tattoo, and the hospital’s decision about what it required of them, has set off a conversation among doctors and medical ethicists around the country about how to express one’s end-of-life wishes effectively, and how policymakers can make it easier.
In the U.S., the standard way to tell doctors you want to be allowed to die is to sign an official form saying you don’t want to be resuscitated. That means, among other things, you don’t want doctors to do CPR or use a ventilator to keep you alive if you stop breathing.
But signing the official form doesn’t guarantee your wishes will be followed. If you lose consciousness and end up in the emergency room, for example, the form may not come with you, in which case many doctors err on the side of intervening.
“A lot of doctors say, ‘Look, you can always be dead later. Don’t take a course that’s irreversible’,” explains Dr. Kenneth Goodman, a longtime medical ethicist for the University of Miami hospital and the man Dr. Holt called when he saw the man’s tattoo. It was his job to figure out the best course of action, and quickly — the man seemed to be dying.
“Our big concern was, is this real?” remembers Holt. The only previous example they could find in the medical literature was a case from 2012, in which a man with a chest tattoo that read “D.N.R.” told doctors it was the result of a drunken bet, and that it didn’t reflect his wishes.
And, even if this tattoo was real, it was initially unclear whether it should carry the same weight as an official form stating the same thing.
“My thoughts were these,” explains Goodman. “He’s gone through the trouble of getting this tattoo that says please don’t do this to me, and he’s probably seen it pretty frequently since then. I suppose every time one’s looking in the mirror one would see this.”
In that way, the tattoo might be more likely to reflect the man’s current wishes than a form, which he might have signed and forgotten to update. “If we take a piece of paper at face value even if he might have changed his mind, we really should take this tattoo at face value, even if he might have changed his mind,” Goodman says.
Goodman advised the doctors to take the tattoo seriously. The man got sicker and sicker overnight. They didn’t do CPR. The man died. And social workers eventually found the man had an out-of-hospital form on file with the Florida Department of Health that backed up his tattoo.
Holt published a case study about the patient in TheNew England Journal of Medicine in November, thinking it might be helpful for other doctors. Since then, he and Goodman say they have heard from a wide range of doctors ethicists.
“It started a good conversation,” says Holt, about how to help people express their end-of-life wishes in productive ways. Tattoos, he and Goodman both say, are not the answer. Although the tattoo ultimately worked in this case, “the long and short of it is that I don’t think it’s a useful thing. It really gave us more pause than help,” Holt says.
What would really be helpful is an easy way to access official forms from everywhere. Ideally, EMTs and ER docs could both know instantly what care an unconscious person wants.
“Imagine an ordinary patient who has a preference never to be resuscitated, and that is in her record,” says Goodman “Why then, that ought to be something you can call up anywhere.” Some states have attempted to do that by establishing electronic registries for a type of directive called a POLST form, which is meant to be used by very old or sick people.
Oregon’s registry has increased the odds that people get the care they want, and since California launched a pilot registry in 2016, some doctors say they have seen fewer patients who choose to wear their preferences on their bodies — etched in bracelets, mostly, not tattooed on their skin.
What Happens When CHIP Funds Run Out

One of the central issues of the shutdown battle is the Children’s Health Insurance Program. NPR’s Michel Martin talks with Alabama CHIP Director Cathy Caldwell about the program, which covers 9 million low-income kids across the U.S.
MICHEL MARTIN, HOST:
We’d like to turn now to one of the main issues caught in the middle of the spending battle in Congress – the Children’s Health Insurance Program, also known as CHIP. This program helps state insure about 9 million children whose parents can’t afford health insurance but make too much to qualify for Medicaid. At the moment, the program is operating on a temporary funding extension that’s expected to dry up in March, but several states say they could run out of funding before then. One of those states is Alabama.
And joining us now is Cathy Caldwell. She is the director of Alabama’s CHIP program. She’s speaking to us from Prattville, Ala. Cathy Caldwell, thank you so much for speaking with us.
CATHY CALDWELL: Oh, thank you for having me.
MARTIN: So for people who aren’t familiar with the program, could you just describe briefly, you know, what it does – amplify what I said earlier?
CALDWELL: Sure. The Children’s Health Insurance Program provides health insurance to uninsured children whose family income is above the Medicaid level. Currently, in Alabama, we have over 85,000 children insured in that program.
MARTIN: And how exactly does it work? Does it work like any other insurance program – people can go to the doctor that they want, go to the hospital if they need to?
CALDWELL: Absolutely. We have a comprehensive benefit package that provides a wide array of benefits for many services, including WellCare so children can get their preventive visits. They can get their immunizations. Also, (unintelligible) care certainly can go to the doctor when they’re sick. We cover inpatient. We also cover mental health services, vision and dental – so a very comprehensive benefit package.
MARTIN: One of my colleagues spoke with you in December. And you said then that your state could exhaust CHIP funds in February. If those funds run out, what happens if a kid whose family has CHIP gets sick and has to go to the doctor or to the hospital? What happens?
CALDWELL: And we did receive some additional funding. But we’re still worried that it’s going to run out before too long. What will happen when we exhaust our funding – we will dis-enroll children from the program. Many of those children will become uninsured. So for many, they will probably not be able to access all of the services they need.
If they’re sick, for example, and go to the doctor, they’ll be expected to pay for it out of their own pocket. In an emergency situation, it’s a – you know go to the emergency department or even an inpatient stay – the family will be expected to pay for those services which will be quite expensive. So it’ll create a hardship on the family. And like I said, there will be situations, likely, where the children won’t be able to obtain the services they need.
MARTIN: I’m sure you know now that we’re in a bit of a standoff here and that both the Republicans and Democrats in Washington are accusing each other of holding, you know, the country hostage to this or that program. Many of the Democrats are saying that the Republicans are using this as a bargaining chip to, you know, force them to vote for something – other things that they don’t agree with. I’d like to ask, how is this all striking you where you are?
CALDWELL: I would like to say that there is huge urgency. I think some people look at the numbers and think that if we still have a few weeks of funding, then there’s no urgency. That is absolutely not the case. These are large programs with many children enrolled. And so if in fact funding does not continue, then we have to shut down our programs. It is going to take time and many resources to accomplish that. So we need Congress to act and extend funding. And we really need to get that down this month.
MARTIN: That’s Cathy Caldwell. She is the director of Alabama’s CHIP program. We reached her in Prattville, Ala. Cathy Caldwell, thank you so much for speaking with us. We really appreciate it.
CALDWELL: Oh, you’re very welcome. Thanks for having me.
(SOUNDBITE OF KOLOTO’S “LIFE IN CLAY”)
Copyright © 2018 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Missouri Faces Costly Dilemma: How To Treat Inmates With Hepatitis C?

{kind=link}
Jymie Jimerson collects Willie Nelson memorabilia in her home in remembrance of her late husband, Steve, who was a fan.
Alex Smith/KCUR
hide caption
toggle caption
Alex Smith/KCUR
In a corner of Jymie Jimerson’s house in the town of Sparta, in southwest Missouri, she has set up a kind of shrine. It has Native American art representing her Cherokee heritage alongside Willie Nelson albums, books and photos in remembrance of her late husband.
There’s a copy of Willie’s mid-’70s LP Red Headed Stranger. “When Steve was young, he had red hair and a red beard, so he always really identified with Willie’s Red Headed Stranger,” Jimerson says. “I try to keep it up there as a reminder of better days.”
Her husband, Steve Jimerson, was sentenced to life in prison in 1996 for his role in the shooting deaths of two men. Jymie says her husband’s life had been ravaged by drug abuse. But after he entered prison, he got off drugs and become a mentor for other inmates.
“Once he got inside, recovery became his life,” Jymie says. “And that was his passion until the day he died.”
Steve died on Jan. 6, 2017, of complications from hepatitis C, a liver infection that’s especially widespread among prison inmates. He was 59.
While the disease is common among the incarcerated, treatment with the latest hepatitis drugs isn’t.
Civil liberties groups in Missouri and at least seven other states are now suing to get more inmates treated with new-generation hepatitis C drugs that are highly effective but also very costly.
After Steve Jimerson was diagnosed with hepatitis C while in prison, Jymie says he was on the lookout for news of treatment advances.
In 2013, Gilead Sciences introduced Sovaldi, the first of a new generation of drugs called direct-acting antivirals that can cure hepatitis C and with fewer side effects than the previous treatments. But the excitement was dampened by the drug’s price. A full course of treatment cost $84,000.
In 2016, around 5,000 inmates in Missouri’s inmates had hepatitis C, and no more than 14 of them received the drugs, according to internal state data obtained by the MacArthur Justice Center in St. Louis.That’s about 15 percent of the 32,000 people incarcerated in Missouri’s prisons.
Jymie says that her husband wasn’t given direct-acting antivirals. By the fall of 2016, Jimerson’s health was deteriorating rapidly, and he grew pessimistic about the prospects for a cure.
“He told me that if someone had to die to get the DOC [Department of Corrections] to change their policy, he was OK with it being him,” Jymie says.
As recently as 2012, scores of Missouri inmates were being treated with older hepatitis C drugs, including one called interferon that is notorious for its debilitating side effects.
But in 2013, the Federal Bureau of Prisons started changing treatment guidelines to replace the old hepatitis C drugs with new ones.
Many states follow those guidelines, including Missouri, according to a spokesperson from Corizon Health, the private company that provides health care for Missouri’s inmates.
But the updated guidelines gave prisons more leeway to decide when it’s appropriate to provide treatment. And asMissouri phased out the old drugs, it hasn’t used the new drugs nearly as often. That has left only a handful of inmates getting any hepatitis C drug treatment at all.
In December of 2016, the American Civil Liberties Union and MacArthur Justice Center sued to get the Missouri Department of Corrections to provide direct-acting antiviral drugs to inmates with hepatitis C who qualify for treatment.
ACLU lawyer Tony Rothert says the state’s current treatment practices violate the Constitution’s Cruel and Unusual Punishments Clause.
“The Supreme Court has said that in the context of medical care, that means that prisons cannot be deliberately indifferent to serious medical needs,” Rothert says. “Hepatitis C fairly easily satisfies this test, because if left untreated, there’s a fair chance that you will die.”
Advocates making this argument got a big boost for their case in November, 2017, when a federal judge in Florida ordered that state’s prisons to start providing direct-acting drugs to its inmates at least until that state’s case goes to trial in August.
“It was a great victory for people who are incarcerated and have hepatitis C because now we have a federal judge who said, ‘Look, this is just unconscionable,’ and the state is going to have to do something about it,” says Elizabeth Paukstis, public policy director of the National Viral Hepatitis Roundtable.
In July, 2017, the Missouri lawsuit took a leap forward when the judge overseeing the case certified it as a class action on behalf of state inmates with hepatitis C. The Missouri Department of Corrections and Corizon, which are defendants in the lawsuit, have appealed that ruling.
Both the Missouri Department of Corrections and Corizon declined to comment on the suit or answer questions about their hepatitis C treatment protocols beyond saying they are following federal guidelines.
But if Missouri and other states are required to offer the new drugs, they would face a huge problem, says Gregg Gonsalves, an assistant professor of epidemiology at the Yale School of Public Health. “Even if they wanted to treat patients, they would break the bank. They would run out of money to treat every other medical condition,” he says.
For example, if Missouri gave the 2,500 inmates that the ACLU says are candidates for Harvoni, the acting antiviral drug it now uses, the cost would exceed $236 million, based on its list price. That far exceeds the Department of Corrections’ entire budget for inmate health.
Gonsalves says the emergence of newer, cheaper drugs could help, and some state prison systems have managed to negotiate discounts.
Even at a lower cost, though, providing these drugs on a large scale could still cost states a fortune. But advocates insist it’s worth it to stop the disease from spreading.And a 2015 study showed that as many as 12,000 lives would be saved if inmates across the country were screened and treated; preventing liver transplants and liver disease would save money in the long run.
“The impetus for treating infectious disease in the prison system is that it’s a population you can reach, it’s a population you can cure, and it’s a population you can help prevent onward infections from,” Gonsalves says.
Jymie Jimerson understands that many people might be skeptical about providing expensive health care for prison inmates. But she hopes they can see them as more than people convicted of crimes.
“I’m not condoning what they did. I’m not condoning criminals,” she says. “What I’m saying is, they’re human beings. And there are hundreds, hundreds of first-time offenders that this medication would cure them. So that when they went home, they could actually spend time and enjoy a little bit of life with their families.”
This story is part of a reporting partnership with NPR, KCUR and Kaiser Health News. You can find Smith on Twitter: @AlexSmithKCUR.
Roger Severino Discusses The HHS Division Of Conscience And Religious Freedom
NPR’s Kelly McEvers speaks with Roger Severino about the new Department of Health and Human Services Division of Conscience and Religious Freedom, which is intended to protect people from discrimination if they refuse to participate in health services, against their beliefs.