Trump Admin Will Protect Health Workers Who Refuse Services On Religious Grounds

The Department of Health and Humans Services is adding a Division of Conscience and Religious Freedom to protect doctors, nurses and other health care workers who refuse to take part in some kinds of care because of moral or religious objections.
Mark Wilson/Getty Images
hide caption
toggle caption
Mark Wilson/Getty Images
Updated at 12:39 p.m. ET
Health care workers who want to refuse to treat patients because of religious or moral beliefs will have a new defender in the Trump administration.
The top civil rights official at the Department of Health and Human Services is creating the Division of Conscience and Religious Freedom to protect doctors, nurses and other health care workers who refuse to take part in procedures like abortion or treat certain people because of moral or religious objections.
“Never forget that religious freedom is a primary freedom, that it is a civil right that deserves enforcement and respect,” said Roger Severino, the director of HHS’s Office for Civil Rights, at a ceremony to announce the new division.
The establishment of the division reverses an Obama-era policy that barred health care workers from refusing to treat transgender individuals or people who have had or are seeking abortions.
That Obama rule was challenged in court by the Franciscan Alliance, a Christian health care organization in Texas, and a judge in 2016 blocked enforcement as the case played out in court.
The new division appears to be primarily aimed at preventing health care workers from participating in abortion services that go against their religious beliefs. The division cites a 2011 federal regulation guiding the enforcement of conscience protections that mentions abortion more than 30 times.
Louise Melling, deputy legal director at the American Civil Liberties Union, said those conscience objections could expand to allow health workers to refuse some services to gay, lesbian and transgender people.
“This administration has taken a very expansive view of religious liberty,” she said in an interview. “It understands religious liberty to override antidiscrimination principles.”
HHS makes clear that it won’t allow gender discrimination that is banned by federal law. The question, according to Melling, is whether the administration includes gender identity and sexual orientation in the definition of gender.
She says there are many examples of health workers refusing care on religious grounds, including a nurse who didn’t want to provide post-operative care to a woman who had an abortion, a pediatrician who declined to see a child because his parents were lesbians and a fertility doctor who didn’t want to provide services to a lesbian couple.
Acting HHS Secretary Eric Hargan said Thursday that is the point.
“For too long too many of these health care practitioners have been bullied and discriminated against because of their religious beliefs and moral conviction,” he said.
The government, he said, has “hounded religious hospitals and the men and women who staff them, forcing them to provide and refer for services that violate their consciences.”
The new division won’t have to wait to get to work. A pediatric nurse at the Winnebago County Health Department in Illinois filed a complaint with HHS on Tuesday because she objects to her employer requiring that she be trained to make referrals to providers of abortion services or to help woman get abortion drugs, according to the Rockford Register Star.
This isn’t the first time in the Trump administration that HHS’s Office of Civil Rights has moved to protect people with moral or religious objections to some kinds of health care. In October, the agency allowed employers to refuse to pay for birth control coverage.
“Health providers should have the ability to live their religious beliefs without fear of workplace discrimination,” said Sen. James Lankford, R-Okla., in a statement.
Lankford has long advocated for such protections and has sponsored a bill called the Conscience Protection Act to codify the rules.
HHS To Protect Health Workers With Religious Objections

The Department of Health and Human Services is expected to announce the creation of a new division to protect health workers who object to procedures like abortions for religious reasons.
Home Care Agencies Often Wrongly Deny Medicare Help To The Chronically Ill

Colin Campbell last month in his home near Los Angeles, Calif. Campbell was diagnosed with Lou Gehrig’s disease — ALS — eight years ago. He gets Medicare because of his disability, but was incorrectly told by several agencies that he couldn’t use it for home care. So, instead, he pays $4,000 a month for those services.
Heidi de Marco/Kaiser Health News
hide caption
toggle caption
Heidi de Marco/Kaiser Health News
Colin Campbell needs help dressing, bathing and moving between his bed and his wheelchair. He has a feeding tube because his partially paralyzed tongue makes swallowing “almost impossible,” he says.
Campbell, 58, spends $4,000 a month on home health care services so he can continue to live in his home just outside Los Angeles. Eight years ago, he was diagnosed with amyotrophic lateral sclerosis, or “Lou Gehrig’s disease,” which relentlessly attacks the nerve cells in his brain and spinal cord and has no cure.
Because of his disability, he has Medicare coverage, but he can’t use it for home care — as the former computer systems manager has been told by 14 home health care providers.
That’s an incorrect but common belief. Medicare does cover home care services for patients who qualify but, according to advocates for seniors and the homecare industry, incentives intended to combat fraud and reward high quality care are driving some home health agencies to avoid taking on long-term patients, such as Campbell, who have debilitating conditions that won’t get better. Rule changes that took effect this month could make the problem worse.
“We feel Medicare coverage laws are not being enforced and people are not getting the care that they need in order to stay in their homes,” says Kathleen Holt, an attorney and associate director of the Center for Medicare Advocacy, a nonprofit, nonpartisan law firm. The group is considering legal action against the government.

Because of his ALS, Colin Campbell needs to wear a brace, and relies on help from a home health worker to get bathed and dressed every day.
Heidi de Marco/Kaiser Health News
hide caption
toggle caption
Heidi de Marco/Kaiser Health News
Federal law requires Medicare to pay indefinitely for home care — with no copayments or deductibles — if a doctor ordered it and patients can leave home only with great difficulty. They must need intermittent nursing, physical therapy or other skilled care that only a trained professional can provide. They do not need to show improvement.
Those who qualify can also receive an aide’s help with dressing, bathing and other daily activities. The combined services are limited to 35 hours a week.
Medicare affirmed this policy in 2013 when it settled a key lawsuit brought by the Center for Medicare Advocacy and Vermont Legal Aid. In that case, the government agreed that Medicare covers skilled nursing and therapy services — including those delivered at home —to maintain a patient’s abilities or to prevent or slow decline. It also agreed to inform providers, those who audit bills, and others that a patient’s improvement is not a condition for coverage.

Campbell is able to move around his house with the help of a walker.
Heidi de Marco/Kaiser Health News
hide caption
toggle caption
Heidi de Marco/Kaiser Health News
Campbell says some home health care agencies told him Medicare would pay only for rehabilitation, “with the idea of getting you better and then leaving,” he says. They told him that Medicare would not pay them if he didn’t improve, he says. Other agencies told him Medicare simply did not cover home health care.
Medicaid, the federal-state program for low-income adults and families, also covers home health care and other home services, but Campbell doesn’t qualify for Medicaid.
Securing Medicare coverage for home health services requires persistence, says John Gillespie, whose mother has gone through five home care agencies since she was diagnosed with ALS in 2014. He successfully appealed Medicare’s decision denying coverage, and afterward Medicare paid for his mother’s visiting nurse as well as speech and physical therapy.
“You have to have a good doctor and people who will help fight for you to get the right company,” says Gillespie, of Orlando, Fla. “Do not take no for an answer.”
Yet a Medicare official did not acknowledge any access problems. “A patient can continue to receive Medicare home health services as long as he/she remains eligible for the benefit,” says spokesman Johnathan Monroe.
But a leading industry group contends that Medicare’s home health care policies are often misconstrued. “One of the myths in Medicare is that chronically ill individuals are not qualified for coverage,” says William Dombi, president of the National Association for Home Care and Hospice, which represents nearly half of the nation’s 12,000 home care providers.
Part of the problem is that some agencies fear they won’t be paid if they take on patients who need their services for a long time, Dombi says. Such cases can attract the attention of Medicare auditors who can deny payments if they believe the patient is not eligible, or they suspect billing fraud. Rather than risk not getting paid, some home health agencies “stay under the radar” by taking on fewer Medicare patients who need long-term care, Dombi says.
And those companies may have a good reason to be concerned. Medicare officials have found that about a third of the agency’s payments to home health firms in the fiscal year ending last September were improper.
Shortages of home health aides in some areas might also lead an overburdened agency to focus on those who need care for only a short time, Dombi says.
Another factor that may have a negative effect on chronically ill patients is Medicare’s Home Health Compare ratings website. It includes grades on patient improvement, such as whether a client got better at walking with an agency’s help. That effectively tells agencies who want top ratings “to go to patients who are susceptible to improvement,” Dombi says.
This year, some home care agencies will earn more than just ratings. Under a Medicare pilot program, home health firms in nine states will start receiving payment bonuses for providing good care and those who don’t will pay penalties. Some criteria used to measure performance depend on patient improvement, Holt says.
Another new rule, which took effect last Saturday, prohibits agencies from discontinuing services for Medicare and Medicaid patients without a doctor’s order. But that, too, could backfire.
“This is good,” Holt says. “But our concern is that some agencies might hesitate to take patients if they don’t think they can easily discharge them.”
This article was written with the support of a journalism fellowship from New America Media, the Gerontological Society of America and the Silver Century Foundation. Kaiser Health News (KHN) is a nonprofit news service. It’s an editorially independent program of the Kaiser Family Foundation, and not affiliated with Kaiser Permanente. You can find Susan Jaffe on Twitter @susanjaffe.
White House Doctor Says Trump Is In 'Excellent' Physical, Cognitive Health

President Trump shakes hands with White House physician Dr. Ronny Jackson, following his annual physical at Walter Reed National Military Medical Center on Jan. 12.
Saul Loeb/AFP/Getty Images
hide caption
toggle caption
Saul Loeb/AFP/Getty Images
President Trump is in excellent health with “no indication” of “any cognitive issues” — but he could afford to lose a few pounds and start exercising over the coming year, according to the president’s physician.
Dr. Ronny Jackson, a Navy rear admiral who directs the White House medical unit, conducted Trump’s annual physical last Friday. He told reporters on Tuesday that the president’s cardiac health is strong and that there are no concerns about any memory or cognitive issues.
“I found no evidence that the president has any issues whatsoever with his thought process,” Jackson told reporters during Tuesday’s White House briefing.
The tabloid-style book Fire and Fury by journalist Michael Wolff, published this month, led to speculation about Trump’s mental fitness for office. Trump responded to the criticism by calling himself a “very stable genius.”
Jackson said on Tuesday that Trump asked Jackson to perform the cognitive exam, which the doctor did not plan to do, having deemed it unnecessary. Jackson said Trump performed “exceedingly well” and is “very sharp.”
Jackson said the president enjoyed good health despite a subpar diet and no exercise routine.
“It’s called genetics. I don’t know,” Jackson said. “Some people have great genetics. I told the president if he had a healthier diet over the last 20 years he might live to be 200.”
Jackson also noted that Trump has abstained from alcohol and tobacco for his entire life, which contributed to his relatively good health.
Trump, 71, is 6’3″ and weighs 239 pounds, Jackson said, which is classified as overweight and is one pound away from being obese, according to the NIH’s body mass index calculator.
Jackson said he will work with Trump to exercise more over the coming year, to eat better and lose between 10 and 15 pounds.
Trump does take Crestor to lower his cholesterol, daily aspirin for heart health, Propecia for male pattern baldness, a skin cream for rosacea and a daily multivitamin. His blood tests and other vitals were all normal.
Jackson said that there is no reason Trump wouldn’t be able to complete his first term health-wise, in addition to a second term if re-elected.
During the presidential campaign, Trump’s longtime personal physician, Dr. Harold Bornstein, famously declared that Trump would be “the healthiest individual ever elected to the presidency.” Trump released his health history in 2016 on controversial TV host Dr. Mehmet Oz’s show.
As Flu Season Strains Hospitals, Doctor Offers Advice For How To Stay Healthy
An unusually severe flu season has strained hospitals around the country with overflowing emergency rooms. In California alone, at least 42 people have died from the flu. NPR’s Kelly McEvers speaks with Dr. Adrian Cotton, chief of medical operations at Loma Linda University Health System, about the influx of patients and what people can do to protect themselves.
How Active Duty Military Are Navigating Changing Attitudes Toward Marijuana
California is the latest state to begin legal recreational sale of marijuana. That presents a challenge to the thousands of active duty military — and their families — who must navigate changing attitudes toward marijuana use, which is still prohibited under federal law.
For Now, Sequencing Cancer Tumors Holds More Promise Than Proof

Ben and Tara Stern relax at home in Essex, Md. Ben was diagnosed with glioblastoma in 2016. After conventional treatment failed to stop the tumor, Ben tried an experimental drug.
Meredith Rizzo/NPR
hide caption
toggle caption
Meredith Rizzo/NPR
People diagnosed with cancer understandably reach for the very best that medical science has to offer. That motivation is increasingly driving people to ask to have the DNA of their tumors sequenced. And while that’s useful for some malignancies, the hype of precision medicine for cancer is getting far ahead of the facts.
It’s easy to understand why that’s the case. When you hear stories about the use of DNA sequencing to create individualized cancer treatment, chances are they are uplifting stories. Like that of Ben Stern.
In the spring of 2016, Stern was diagnosed with a deadly brain cancer, glioblastoma. His doctors at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins promptly treated him with surgery, then over the months, chemotherapy and radiation. He even got on a clinical trial to see if a leading edge drug called a checkpoint inhibitor would work.
Ben Stern found out abruptly that wasn’t doing the trick either, when he was struck with a seizure. “My whole right side clenched up and [my wife] Tara had called 911 in the middle of it.”
The tumor had grown back, so surgeons went in again to remove what they could. Tara said the next month’s appointment showed the surgery hadn’t worked, either.
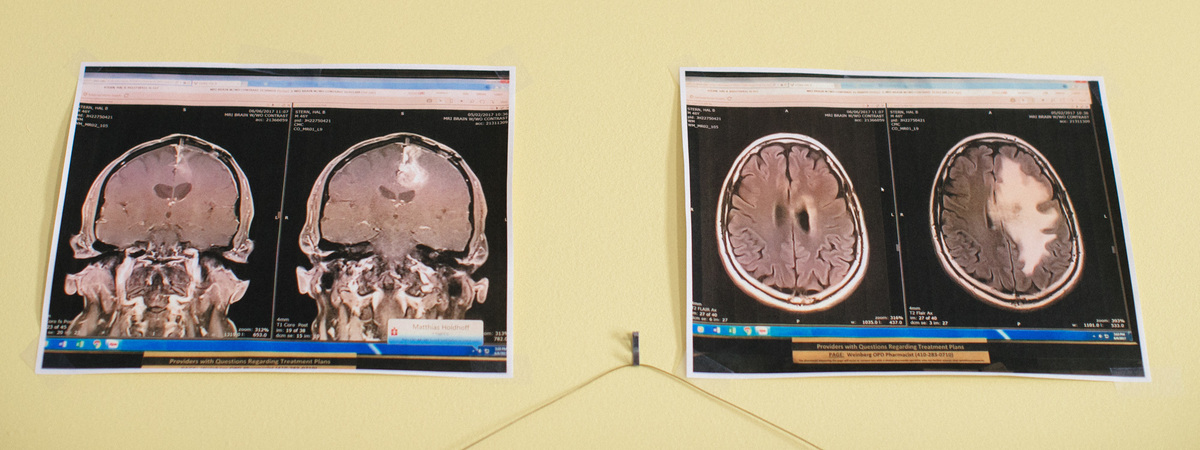
“The tumor had already grown back and it was already bigger than the original size tumor that we had found the previous May,” Tara Stern says. This staggering regrowth took only five weeks.

The Sterns hang up images of Ben’s brain tumor, shown on the right (white) in each image, and also five weeks after treatment.
Meredith Rizzo/NPR
hide caption
toggle caption
Meredith Rizzo/NPR
Stern’s doctor got a sample of the tumor and sent a genetic analysis of it to what Hopkins calls its “molecular tumor board.” It’s a small group of doctors who meet Mondays to review these genetic tests. They found an overactive gene in his tumor that’s only rarely associated with brain cancer. But that mutation in other cancers sometimes responds to a particular drug. So Ben went on it as part of his ongoing treatment.
“He started his next round of chemotherapy that Monday but he didn’t seem to get weaker,” Tara says, “He was getting stronger almost every day. It was almost miraculous.”
Ben says the drug even reversed his deteriorating mental state brought on by the brain tumor. At the next monthly appointment, following a brain scan, Ben and Tara got more good news.
“The tumor was immeasurable on that next MRI,” Tara says. “It wasn’t there, to put it bluntly.”
Ben’s eyes well up as he hears his wife telling the story. “I was basically as I am now, which is in tears.”
Eight months later, Ben was thinking ahead about his future, rather than wondering whether his life is ending.

Ben and Tara on their wedding day in 2014. Two years after they got married, Ben was diagnosed with a brain tumor.
Meredith Rizzo/NPR
hide caption
toggle caption
Meredith Rizzo/NPR
“We have to use this result with caution because we don’t know how long this effect might wear on, but for the time being this is a clinically very meaningful benefit,” says his doctor at Hopkins, medical oncologist Matthias Holdhoff.
And while it’s a good-news story for the field of precision medicine, it is also not the way most of these stories end.
“We’re getting better, but like many things in life, there’s hope and hype. And that’s also the reality with precision medicine right now,” says Ben Park, an oncology professor at the Sidney Kimmel Comprehensive Cancer Center at Hopkins. After noticing how much confusing genetic information was flooding doctors at Hopkins, he founded the molecular tumor board there.
“The reason I started this tumor board [in 2013]… was simply because there was a patient, a young woman who had metastatic breast cancer who had a mutation on one of these reports and decided to forego standard-of-care therapies, which have been proven to actually prolong life in this setting,” Park says. Instead, the woman enrolled in a clinical trial that didn’t really make sense for her particular type of cancer and “she almost died. She had really bad toxicity from the experimental drug.”
She was drawn, Park says, by the allure of precision medicine. Patients and doctors alike are clamoring for these tests. But interpreting the results isn’t easy because different companies offer these tests and interpret the DNA signatures differently, “and that can make a huge difference,” Park says.
“That’s where we’re having difficulty right now as a field,” he says, harmonizing test results that often disagree with each other.

Ben’s tumor recently grew back and he’s now undergoing further treatment.
Meredith Rizzo/NPR
hide caption
toggle caption
Meredith Rizzo/NPR
At Hopkins, the genomic tests usually don’t offer any suggestion for treatment. Only about one quarter of patients at Hopkins are steered toward particular drugs or toward ongoing clinical trials. Other top medical centers find they can identify potential treatments only about 10 percent of the time.
So far there’s only been one randomized study of this approach to precision cancer care — and it did not show a survival advantage for people who went through all this genetic testing.
“If you have this knowledge, it’s not enough,” Park says. “You have to prove that acting on that knowledge — some medical intervention — will actually afford benefit for patients. That’s the trickiest, toughest part about looking at all these types of genomic tests, to really prove that this is making a difference in the lives of our patients.”
Park has since passed on leadership of the molecular tumor board to his colleague, oncologist Josh Lauring. Lauring says there are a few cancers where DNA analysis does make a clear difference, say in melanoma and certain types of lung cancer.

Tara keeps detailed notes of Ben’s progress and also keeps track of his treatment schedule on a daily basis.
Meredith Rizzo/NPR
hide caption
toggle caption
Meredith Rizzo/NPR
“In other cancers, it’s really kind of an open question. At the same time, this testing is available commercially as well as at academic medical centers, and is being done. Patients want it, providers want it.”
So what’s happening, in effect, is a huge, unorganized experiment, involving real patients, treated differently in all sorts of settings. Lauring and colleagues at Hopkins are trying to keep track of all their patients: what treatment they got, how long it was successful, and how long the patients lived.
“We think it’s really important to capture that information as well, to try to learn from it,” Lauring says, “because in many cases it’s not going to be effective, but in some it is, and it’s important for us to figure that out.”
Therapies that target specific genetic patterns are appealing because medical scientists have some sense of the biology underlying their drugs — they aren’t just killing fast-growing cells, as conventional chemotherapy does.
“Unfortunately in many cases these responses, if they occur, are relatively brief.”
That unfortunately turned out to be the case for Ben Stern as well. Five months after his remarkable response, Ben started feeling weaker again. An MRI suggested the cancer might be on the move. So he went back to the hospital for another round of chemotherapy and radiation.
They’re hoping for the best.
Contact Richard Harris at rharris@npr.org.
The Call-In: The Nursing Industry
Depending on where you live, nurses can be in short supply. NPR’s Lulu Garcia-Navarro talks to Peter Buerhaus, a nursing professor at Montana State University, about the changing nursing industry.
LULU GARCIA-NAVARRO, HOST:
Now it’s time for the Call-In. Last week, we put nurses on call. Depending on where you live, nurses can be in short supply with potentially big consequences for patient care. What does it mean for the nursing industry, and how is the job changing? Well, we heard from a lot of you.
Here’s Ed Stern of Falls Church, Va., Gina DeMarco of Colorado Springs, Jennifer Steele of Milwaukee, and Christopher Todd of Big Pine Key, Fla.
ED STERN: I think nursing has changed. It’s evolved. It’s not just fluffing pillows and passing medications.
GINA DEMARCO: It’s physically demanding. It’s stressful. The hours are long. There’s days it’s rewarding, but I would say I second guess what I’m doing.
JENNIFER STEELE: This has been the most challenging and rewarding work. Nursing is not what I do; it is who I am.
CHRISTOPHER TODD: There’s always been a nursing shortage. And it’s only going to get worse because the average age of a nurse is getting up there.
GARCIA-NAVARRO: Twenty years ago, the nursing industry was in danger of a serious shortage, but that’s changed more recently.
PETER BUERHAUS: The good news is we have had a surge of people coming into nursing over the past 10 years such that we believe we’ll be able to avoid a large massive shortage of registered nurses that would cause access to care difficulties and delay care.
GARCIA-NAVARRO: Peter Buerhaus is a professor of nursing and a healthcare economist at Montana State University. He says around the country, though, there could be regional shortages in the near future.
BUERHAUS: I get a little bit worried around both coasts. New England, particularly, there’s a large number of nurses who are going to be retiring in the New England region but not as many new replacement nurses coming in. The West Coast could also be a troublespot. We just don’t see the growth there as we do in the middle part of the country. So I’m a little bit worried about future shortages developing there.
GARCIA-NAVARRO: I’d like to focus on nurse practitioners because we’re hearing a lot more about them. Explain what they are and why they’re becoming a more important part of the workforce.
BUERHAUS: Nurse practitioners are nurses who have gone back to graduate school for advanced education. They choose a specialty. It could be primary care, or it could be caring for individuals in the emergency room or in acute-care settings. And what’s happening is that when we are looking at projections of physician shortages, we’re seeing that nurse practitioners can fill many of those medical roles that are opening up.
So NPs are growing very rapidly. They also are more likely to be working in rural areas of the country where we have some of the biggest shortages of primary care physicians. So there’s a lot of good reasons to be backing that sort of initiative in the nursing workforce. It’s helping out quite importantly.
GARCIA-NAVARRO: So you’ve mentioned this expanding world of opportunity for nurses. But might it also not be the case – and we heard this from some of our callers that they feel overworked, overstretched – that they’re being asked to do much more than they might have been previously? And that has been a burden.
BUERHAUS: Yeah. What we’ve seen, I think, over the past 10 years, is a significant push to improve quality and safety in our hospitals particularly. Oftentimes, though, this means that a nurse will come to work complying with so many regulations, so many check-off forms to note that they did a particular procedure in accordance with the qualifications that are important. Hospitals are under pressure to document that because this is how they’re going to get paid. So it it shifts down on to nurses, and it’s taking them away from the essence of establishing a relationship with a patient.
GARCIA-NAVARRO: And is there another issue, as well? We’re seeing, as you mentioned, younger nurses coming into the workforce, but they don’t have the institutional knowledge. They don’t have the experience, quite frankly. Is that a problem when you see senior-level nurses retiring?
BUERHAUS: It’s a great question, and it does concern me. It’s not that these nurses are not qualified or unprepared. But what concerns me about this, Lulu, is at the same time we have younger people coming in to replace the exiting baby-boom RNs, we’re going to have a surge of older people qualifying for Medicare. Many of them will be hospitalized. And they’re coming in to institutions with multiple chronic conditions – heart disease, stroke, cancer, diabetes. They’re complicated patients. A lot is going on. And they’re coming in just as the newer, less experienced nurses are coming in to take care of them.
GARCIA-NAVARRO: That was Peter Buerhaus, a nursing professor at Montana State University.
(SOUNDBITE OF MUSIC)
ASHLEE DOVER: Hey, Monica.
MONICA COFFEY: Hi, Ashlee.
DOVER: I am a nurse for about two years. So I’m a baby.
COFFEY: Well, congratulations.
DOVER: Thank you.
COFFEY: I’m Monica. And I’ve been a nurse for 41 years, which is probably older than you are (laughter).
GARCIA-NAVARRO: We brought two nurses together to share their experiences in nursing. Ashlee Dover is 24. Monica Coffey is 65. She remembers having a strong mentor when she got started decades ago.
COFFEY: I had a head nurse, Alice McGee (ph). Her office was on the floor. If things got busy, she came and helped pass meds. She gave lunches. And not only did she help me become a better nurse, she helped me to become a better human being. Now I think young nurses are not supported when they are starting out. They come into nursing with far less clinical background than I did as a new grad.
GARCIA-NAVARRO: Ashlee, does that sound right?
DOVER: Yes. That is absolutely correct. Most of the time, it’s just me, a bunch of other new nurses and maybe one or two senior nurses if I’m lucky enough that week to work with them. When you have 6 patients each – all of us – there’s really no time to really say, hey, how are you doing mentally, emotionally? What’s nursing like for you right now? It’s more of – do you need help passing meds, or cleaning up this patient? Can I help you like this?
GARCIA-NAVARRO: Ashlee, do you have any advice that you’d like to ask Monica?
DOVER: How did you mentally and emotionally make it through as a young nurse and, like, keep yourself emotionally, mentally put together for your patients and your family?
COFFEY: Well, I had other interests – an avid reader, hiker. But the thing about nursing is that, every day, I always felt like I was getting to do good work. I feel like the ethics of nursing sustain me. And even when it’s hard, even when it’s discouraging, I always feel like I’m getting to do the best I can do as a human being.
GARCIA-NAVARRO: Does that resonate, Ashlee?
DOVER: That completely resonates because I didn’t go into nursing to try to save lives or anything like that. I went to – I went into nursing to provide care, a shoulder, a listening ear to people in their times where they felt like nobody was listening or they didn’t know what was going on. And that’s my motivating factor is to be there for them. And sometimes it’s hard. You know, you’ve got six patients to take care of, and three of them require head-to-toe, like, complete care. And you just wonder, like, I don’t want to hurt them. I want to be there for them.
COFFEY: Yeah.
GARCIA-NAVARRO: So listening to this, it’s obviously really stressful and also very rewarding. And I just want you both to briefly talk to the patients right now. What do you want them to know?
COFFEY: You go first, Ashlee.
DOVER: OK. I am so privileged to be a part of your care. And I am so absolutely thankful that you let me into your life during these darkest moments. And I want you to know even if I’m late or if I haven’t checked on you in over an hour or two hours, I have not forgotten about you. Your care and everything about you means so much to me. And I promise to give you the best care possible.
COFFEY: That’s a beautiful sentiment and well stated. I would speak to the patients in this country and say, please, get informed about the issues surrounding health care. Think about improving and maintaining access to health care for all Americans.
GARCIA-NAVARRO: That was Ashlee Dover of Nashville, Tenn., and Monica Coffey of Ellsworth, Maine.
(SOUNDBITE OF MUSIC)
GARCIA-NAVARRO: And next week on the Call-In – it’s been a year since the women’s march movement brought huge numbers of demonstrators to the streets across the country. Did you participate last year or did you skip it? What have you done since then? Call in at 202-216-9217. Be sure to include your full name, where you’re from and your phone number. And we may use it on the air. That’s 202-216-9217.
(SOUNDBITE OF THE ANTLERS’ “INTRUDERS”)
Copyright © 2018 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Mapping How The Opioid Epidemic Sparked An HIV Outbreak

A needle exchange program at the Austin Community Outreach Center in Austin, Ind., is aimed at stopping spread of HIV.
Darron Cummings/AP
hide caption
toggle caption
Darron Cummings/AP
When people started to show up to Dr. William Cooke’s primary care office in Austin, Ind., in 2014 with HIV, Cooke knew it was probably related to the region’s opioid epidemic. But what he and the rest of the public health community didn’t know was who they were missing or how long the HIV outbreak had been going on.
Now they’ve got a clearer picture — literally. In visualizations published in the Journal of Infectious Diseases, dots and lines define the constellations of Indiana’s HIV outbreak. Using genetic sequencing, they show how long the outbreak had been going on, connected people who hadn’t previously been linked by traditional methods, and showed how the virus jumped from a slowly spreading infection to a virus transmitted quickly via needle sharing and other, smaller sub-epidemics.
Genetic data has been used to track HIV before. But now, the technology is being used to map HIV outbreaks in real time, lending molecular weight to the in-person interviews that public health officials have used for centuries to track and stop outbreaks. The Austin reconstruction is an example of what it can do.
“This is an instrumental tool for bringing new infections down to zero,” says John Brooks, senior medical advisor at the Centers for Disease Control and Prevention’s Division of HIV/AIDS Prevention. “We have the tools, in terms of treatment reducing transmission to nearly zero. We have prevention… and now we know how to find people.”
The CDC released data Jan. 12 showing that more than 1 in 4 people who inject drugs reuse needles and many not have had an HIV test in the last year, the new data is particularly relevant.
A map to the future of testing
The visualizations aren’t typical maps. There are no boundaries in space. Instead, they map connections, communities and time, using color, lines and dots.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
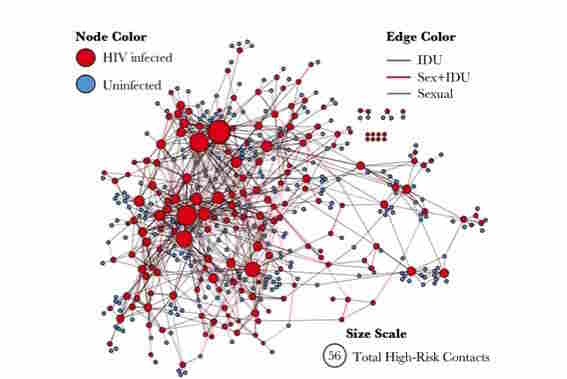
Interviews with people in Scott County, Ind., identified people at high risk of HIV infection (blue circles), and people with HIV (red circles). Larger circles represent people with more high-risk contacts.
CDC/Oxford University Press
hide caption
toggle caption
CDC/Oxford University Press
The maps go through two iterations, linking the traditional shoe-leather epidemiology of painstaking interviews with every person caught up in the outbreak, called contact tracing, to tracking the virus as it evolves.
Interviews yield one vision of the outbreak: a mass of heavily clustered red and blue dots representing people who acquired HIV and people who are at risk but still HIV negative. Some dots are large and red, representing people with HIV and multiple high-risk contacts. Others are closer to pinpoints — in red and blue — showing people with lower risks but also living within the constellation of the outbreak. There are a few outliers with just one or two connections with the larger mass, but it’s a largely undifferentiated huddle of connections and risk.
That’s because as good as person-to-person interviews can be at assessing what made a person vulnerable to HIV and who else should be tested, it inevitably misses people, says Ellsworth Campbell, a CDC computational biologist and the lead author on the paper.
“When the [transmission] is anonymous or they don’t know someone’s status, we miss them,” he says. Public health officials also can miss people outside county lines, since so-called partner tracing ends at the jurisdiction.
Partner interviews can be misleading, also. For instance, flight attendant Gaétan Dugas had long been named “patient zero” in the U.S.’s HIV epidemic. But molecular tracing done in 2016 showed that Dugas’s virus wasn’t the originator of the U.S. epidemic.
So the CDC decided to use the same kind of molecular sleuthing that ferreted out Dugas’s real place in the epidemic, and layer those results over the data health workers collected in interviews. The idea was that they’d test it on the Indiana outbreak first, and then offer the technology, which uses multiple programs and takes partner interviews into account, for free to public health departments across the country.
The DNA tracking found seven different major mutations of the virus as it moved through Scott County, Ind. This included smaller clusters of five or fewer people and three new subgroups that may not have been connected otherwise.
Finding HIV’s fingerprints
HIV is a virus uniquely well suited to this kind of detective work, according to according to Dr. Felipe García, an HIV vaccine researcher in Barcelona, because it mutates rapidly.
“The HIV variability in one person is higher than all the flu variations in the world in one season,” he says. “When you live with HIV, you don’t live with one virus. You live with a population of viruses.”
Researchers knew if the virus DNA sequences were closely related, those infections were connected. They also knew that more distantly related infections either came earlier or later in the outbreak. Using another test, they estimated how recent the infections were. Put those results together with the shoe-leather epidemiology results, and you have the final visualization.
What Campbell and his team found was sometimes surprising. For instance, they found that the progenitor virus — the one that started the epidemic — belonged to a man who had acquired HIV nearly a decade before.
Plus, there were people diagnosed around the same time as the outbreak who had been assumed to be part of it, but the genetic data revealed they were not.
The researchers also wanted to find out what risk factors, such as needle-sharing or unprotected sex, helped spread the virus, so they mapped those, too.
The initial infections were among people who mostly didn’t inject drugs, but did have more than two sex partners. But they accounted for only 1 percent of the infections.
Next, the virus jumped to what would turn out to be the largest group affected: people who shared needles.
But then it shot off in another direction: people who said they shared needles with someone who reported trading sex for drugs or money. This was a discovery: People who traded sex for a fix or a place to stay, but who weren’t necessarily commercial sex workers, turned out to be one of the drivers of the epidemic.
The map suggests multiple times and places that the outbreak could have been stopped, Campbell says. “This can help us respond in the future.”
Early warning signs
The visualization impressed epidemiologist Patrick Sullivan at Emory University. Sullivan works on AIDSVu.org, another HIV visualization tool that maps where the greatest untreated need is, and where the services are. Often, they don’t overlap.
“As the numbers [of new infections] go down, it will be more and more important to be really targeted and as efficient as possible with helping to find folks exposed to HIV and getting them into care,” he says. “This is an exciting new chapter.”
But others aren’t quite as convinced. Indiana physician Cooke treated many of the people in that HIV outbreak. And he said he didn’t need DNA sequences to see it coming.
He rattled off the statistics: Scott County, where Austin is located, was second in the state for hepatitis C rates, which can reflect syringe sharing. In 2014, Scott County had the third-highest rate of drug poisoning deaths — a marker of overdose — and had no syringe access program until most of the people in the outbreak had already been infected. And Scott County had the lowest quality of life in the state, according to Robert Wood Johnson Foundation data.
What’s more, Cooke says, the area was in the top three in the state for measures of childhood abuse and neglect — a marker of adverse childhood experiences that is associated with higher rates of injection drug use and HIV diagnosis.
At each step in this outbreak, officials could have intervened without the DNA map, Cooke says. If that early person with HIV were able to access treatment, the risk of transmitting the virus in the first place would have been negligible. If there had been a syringe access program, there would have been less needle sharing and even injecting drugs wouldn’t have transmitted the virus. If there was adequate mental health care, people might deal with childhood traumas differently. If addiction treatment were more readily available, if HIV prevention tools like Truvada were available everywhere — all of these could have deescalated the outbreak, he says.
Cooke points to another CDC paper, this one from 2016, listing 220 counties, primarily in Appalachia, that face similar risks for HIV outbreaks as Austin.
“If we already know what communities are at risk; why aren’t we doing more?” he says. “There’s more than HIV at stake. There’s infective [skin disease associated with reusing syringes]. There’s OD deaths. There’s hepatitis B and hepatitis C, and lots of other things. The focus shouldn’t just be on the next HIV outbreak, but helping people at risk not get sick and die as much. We can do that without fancy tests in a lab. That’s great for tracking things, but we have real people dying.”
Heather Boerner is a health care and science journalist based in Pittsburgh, and author of Positively Negative: Love, Pregnancy, and Science’s Surprising Victory Over HIV. She’s on Twitter: @HeatherBoerner.
Kentucky Gov. Matt Bevin On Requiring Medicaid Recipients To Work
Kentucky is the first state to require Medicaid recipients to work or get job training in order to qualify for aid. NPR’s Scott Simon talks to Gov. Matt Bevin about the new requirements.
SCOTT SIMON, HOST:
Kentucky’s poised to become the first state to require its residents to work, volunteer or prepare for jobs in order to receive Medicaid benefits. This is after the Trump administration announced it would allow states to begin imposing such rules. The changes will be phased in throughout the coming year. We’re joined now by the governor of Kentucky, Governor Matt Bevin, from his office.
Governor, thanks so much for being with us.
MATT BEVIN: Grateful for the opportunity, Scott.
SIMON: And why is this issue important to you?
BEVIN: This matters to me for a couple of reasons. One thing I want to clarify is that this requirement is for those that Medicaid was not originally designed for. Why is it important to me? I’m a person who grew up with no access to this type of health care. I grew up well below the poverty level, never had the access to the health care system until I was an active duty Army officer in my 20s. So it’s a very personal thing. And I recognize that people in those positions don’t need, as Administrator Verma said, to be treated with the soft bigotry of low expectations. She’s exactly right.
SIMON: Have you considered the effect of requiring people to work in areas that, right now, have a high unemployment rate?
BEVIN: Go through any community anywhere, I promise you will see at least one sign where people want an able-bodied person who is not on drugs and will show up on time to apply for and do a job. There are plenty of jobs in America. There are 100,000-plus available in Kentucky right now. And this will start to connect people who want a job and need a job with the jobs that exist.
SIMON: Governor, as I’m sure I don’t have to tell you, Kentucky has one of the highest rates of death from opioid overdoses in the country. What would you do with people who are struggling with addiction and do need help from Medicaid and other services but are probably in no position to work?
BEVIN: Here’s the wonderful thing. These folks will be identified through this requirement. If, in fact, they’re already receiving benefits, they’re going to an office somewhere to get something, they won’t have to go to anywhere new. They will now be given an opportunity to get treatment. We will continue to invest like this state has never invested in helping people with recovery.
SIMON: And what about those who just, in good faith, can’t meet the requirements? Do they get no care, no coverage?
BEVIN: Think about this. The requirements are for people who are able to meet the requirements. For those who cannot because of a mental disability or a physical disability, it does not apply to them.
SIMON: But will some people lose their coverage? Is that is that the bottom line?
BEVIN: Time will tell. I would hope that they do for all the right reasons. If a person gets a job and is now covered through their employer, then they don’t need it anymore. And those that we project that will no longer be needing it will not be needing it because they will actually be making enough money. They don’t qualify, or they will have coverage through their employers.
SIMON: Is that being hopeful? I mean, in – I don’t have to tell you, Governor, that you can make a pronouncement. But three or four months from now, news organizations might be doing stories about people who couldn’t find jobs and have lost their coverage and have nowhere to turn.
BEVIN: It is hopeful thinking, you bet it is. But I’ll tell you what, as Ralph Waldo Emerson once noted, nothing great was ever achieved without enthusiasm. Enthusiasm springs from hope. And why should we wallow in misery in the belief that we don’t have an alternative other than the failure that we already have? You bet it’s hopeful. And the greatness of the human condition is that it’s always been improved by exactly that.
SIMON: The governor of Kentucky, Matt Bevin – thanks very much for being with us.
BEVIN: Thank you, sir.
Copyright © 2018 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.