Want Help Explaining A Medical Procedure? Ask A 9-Year-Old

Getting ready for a hip replacement? You’ll fare better if you lose the extra weight and get exercise first.
British Medical Journal
hide caption
toggle caption
British Medical Journal
The average American reads at an 8th-grade level, but the patient information that doctors and hospitals provide often presumes that people have much more advanced reading skills.
So some researchers decided to see what happens when 9-year-olds write the patient guides.
Dr. Catrin Wigley at University Hospitals Coventry and Warwickshire NHS Trust and colleagues analyzed six National Health Service patient information leaflets from across England for total hip replacement and found that the average readability level was age 17, even though the average Brit reads at a 4th-grade level. You’d have to have the reading comprehension of a high school senior to understand from these brochures what a hip replacement is, why you need it and what complications might occur.
The researchers recruited 57 nearby elementary school children ages 8 to 10 to help revise the content.

Hey docs, be sure to ask the patient how it went.
British Medical Journal
hide caption
toggle caption
British Medical Journal
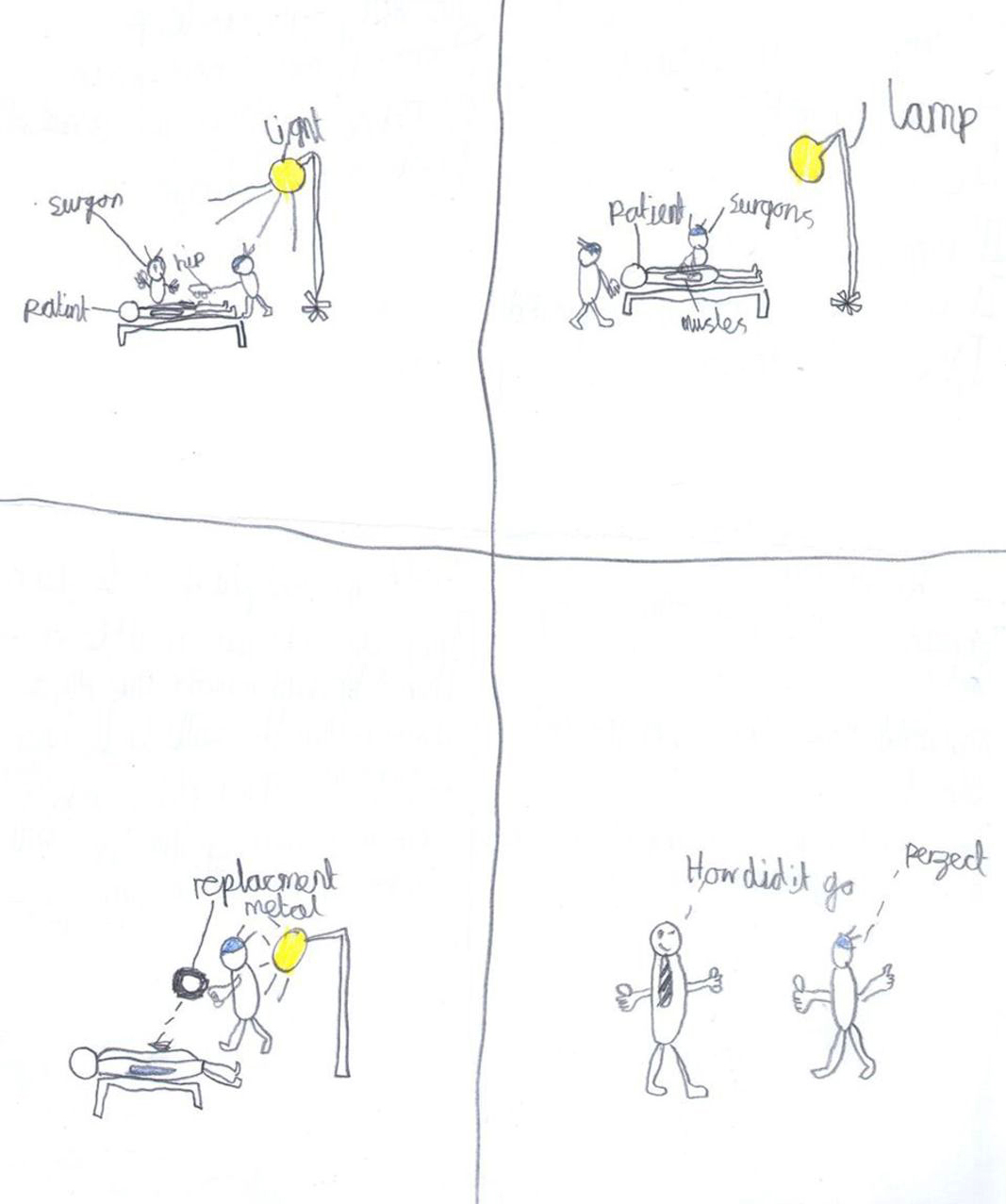
After a lesson about hip replacement, the children were asked to write their own leaflet and draw an image to illustrate it. They were given four headings: indications for surgery, complications of surgery, before the procedure, and the procedure.
What the children came up with was clear, concise and without sugarcoating.
“Your hip is old and rotten,” says Mohammed.
“It is past its sell-by date,” adds Jaime.
What is not allowed before surgery? Coca Cola, fries, and chocolate, according to Lilly.
Of course, no one is suggesting we actually let children write the guides, but maybe we can learn something from their approach.
The authors write: “What better way to write a new leaflet than by engaging with 9-year-old children, so that we can begin to appreciate the disparity in the language we use to convey information through formal patient information leaflets.”
It’s a novel experiment, but can’t really work in practice, according to Cynthia Baur, director of the Horowitz Center for Health Literacy at the University of Maryland’s Public School of Health.
“While children may be able to say things simply, they don’t have the context and experience to recognize aspects of topics that might need more in-depth information or explanation, and they can’t anticipate adult concerns,” Baur says.
But it may shed fresh light on a problem that has been percolating for decades.
Low health literacy leads to poor outcomes for patients and millions of dollars in unnecessary health costs. Countless commissions and organizations have developed plans for improvement. In 2010, the U.S. Department of Health and Human Services published a 73-page action plan to improve health literacy and called for making it a public health priority.
The proliferation of computer-generated patient leaflets was supposed to help. Yet measurement tools with great names like Simple Measure of Gobbledygook (SMOG) and Gunning Fog (GFI) show that these patient education materials are often too complex for the average person.
“I definitely think patient materials have improved, but they are still far from where they need to be,” says Baur, who edited the HHS action plan and created the Centers for Disease Control and Prevention’s health literacy site prior to her appointment at Maryland. “These tools, along with audience testing, of the materials will make health materials much better much faster.”
So can we learn something from the experiment? Maybe simplicity. “Let’s take our cue from the children and begin speaking honestly and to the point with our patients in a language they understand,” Wigley and her colleagues write in their analysis.
What works, says Bauer, is involving the intended recipients. “Health care organizations that truly care about excellent patient experiences and well-being will find ways to involve patients, caregivers and others in the routine development of all types of health communication, even forms and facility signs,” she says.
Sometimes It Takes A 'Village' To Help Seniors Stay In Their Homes
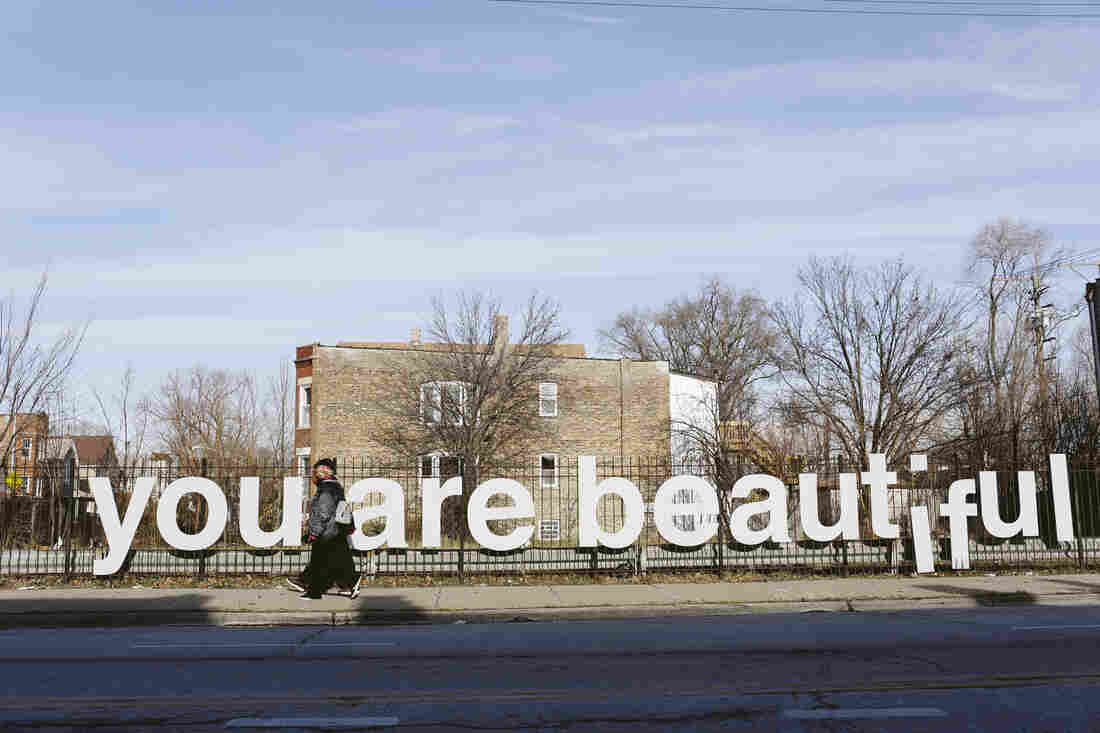
People are seen walking pass the “You Are Beautiful” sign, an art installation, in the Englewood neighborhood on Chicago’s South Side. Nearly half of the people in this African American neighborhood live below the poverty line and many seniors have no idea there are public services that might help them.
Kristen Norman/NPR
hide caption
toggle caption
Kristen Norman/NPR
Debra Thompson is throwing a block party. She’s got good weather for it. That’s never a sure thing in Chicago. It’s a warm and sunny autumn afternoon. Music is playing, hot dogs are grilling.
But this party isn’t just for fun. Thompson is the volunteer chairperson of Englewood Village, an organization that connects low-income older adults on the city’s south side with services from nutrition to job assistance to home repair. And this is how she’s reaching out to potential new members.
“We have flyers, we’re going to knock on doors, spreading the word, getting everybody involved,” says Thompson with her usual boundless enthusiasm.
The Englewood Village has been around since 2015. But its roots go back 17 years and all the way to Boston, where Susan McWhinney-Morse and her friends were grappling with anxieties about aging. They wanted to stay in their homes as long as possible. They wanted to remain in their community on Beacon Hill.
After a couple of years of effort, they produced the concept now known as the Village. It’s a membership-run organization that provides access to services like transportation, help with household chores, even trouble-shooting computer problems, along with classes and social activities.
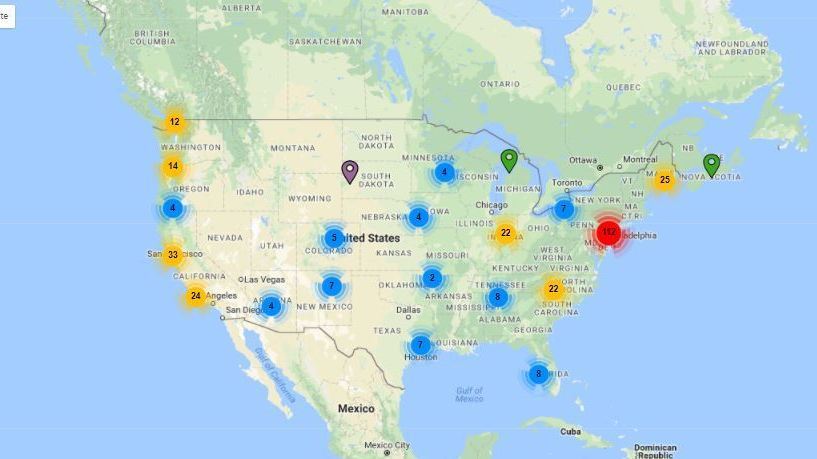
The idea of being able to maintain independence into one’s 80s or 90s is so irresistible, that over the past decade the number of villages across the country has grown from just that one in Boston to 230. Another 130 are in development. An independent organization has been founded to support the expansion of villages. It’s called the Village to Village Network, which has a map on its web site showing where Villages are located.

Debra Thompson in her office at the Englewood Senior Center.
Ina Jaffe/NPR
hide caption
toggle caption
Ina Jaffe/NPR
So far, the overwhelming majority of Village members are middle class or wealthier, according to research from The Center for the Advanced Study of Aging Services at the University of California at Berkeley. That may have something to do with membership dues amounting to several hundred dollars a year. But now the idea is being adapted to serve more varied communities, where dues are not an issue.
Our reporting was inspired by NPR listeners. Earlier this year we asked them to share their stories of how older adults without family caregivers manage when they need help. Many respondents mentioned the Villages in their own communities.
So this past fall, we traveled around the country to take a look at how Villages are evolving. We found an effort in Chicago to create Villages that serve low-income communities of color. We found a Village in rural California where older adults don’t just receive services, they also provide them. Ultimately, what we found was that in practice, the Village model isn’t so much a fixed formula, as an expression of older adults’ desires to age with dignity and independence.
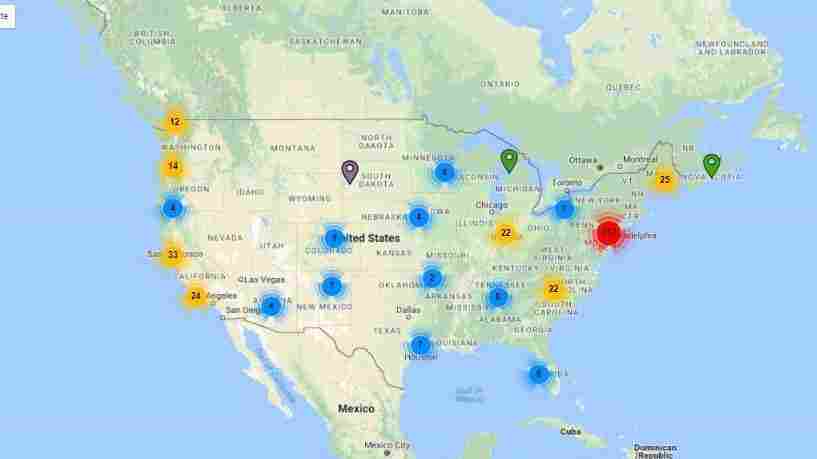
The Village to Village Network tracks the hundreds of villages in the country.
Village To Village Network
hide caption
toggle caption
Or as Susan McWhinney-Morse put it, “a grassroots movement on the part of older people who did not want to be patronized, isolated, [or] infantilized.”
Changing expectations
McWhinney-Morse says that back in 2000 in Beacon Hill, continuing to live independently wasn’t expected after age 65.
“That was the line when one became suddenly old,” she says. “I knew from everything I read that it was the time when I should move: move south, move flat, move warm, move safe, but certainly not stay in my house on Beacon Hill.”
And who wouldn’t want to stay in Beacon Hill, with its colonial-style architecture, cobble stone sidewalks and charming little shops. So McWhinney-Morse and about a dozen friends tried to find a way to get the support they needed as they aged, without having to give up their homes and their community.
Susan McWhinney-Morse, one of the founders of Beacon Hill Village, at the political chat breakfast. She’s the one gesturing. Muriel Feingold is to her right, wearing the scarf.
Ina Jaffe/NPR
hide caption
toggle caption
Ina Jaffe/NPR
The result of two years of effort was Beacon Hill Village. Members pay dues of a few hundred dollars a year. In exchange, they have access to a wide array of discounted services–from home health to home repair to transportation. There’s also a busy calendar of classes, trips, and social events.
There was nothing else around like Beacon Hill Village for several years. Then around 2006, it started to get a little bit of media attention. A little bit was all it took. McWhinney-Morse says once, in a single week, “we literally – this is not an exaggeration—received one thousand telephone calls or emails from across the country from people saying, ‘How do I start a village, is there a village in my neighborhood, what do I do, who can I call, may I come and see you?'”
Beacon Hill Village is no longer novel. It’s been around for 15 years and has more than 300 members. And every Wednesday morning for nearly a decade, at least a dozen of them have met to discuss politics over French toast and oatmeal.
Observations about climate change, DACA, and President Trump’s latest tweet rise above the clink of cutlery and coffee cups.
“It’s made me much more alert,” says 80-year-old Muriel Feinberg. “I have to keep up with stuff because [I know] I’m meeting people on Wednesday. So I think I’ve been more attuned to what’s going on politically and internationally.”
Beacon Hill Village is also providing the kind of help with daily activities that was part of the original vision. Like rides to the supermarket. Tom Moore, 67, drives several days a week for Beacon Hill Village members. He used to be in the travel business. This is his retirement job.
He doesn’t do it just for the money. “I enjoy it,” he says. “I meet a great group of people.”
One of them is 83-year-old Joan Smith. She emerges from her apartment building slowly, using a cane. “I have a problem with balance if I go too fast,” she says. “I didn’t want to use it,” she says of her cane, but the Beacon Hill cobble stones can trip her up and the cane does seem to help.
So the ride to the supermarket is essential for her. It’s also fun. Smith enjoys getting her own groceries, checking the specials, seeing what’s new. But that’s now beyond what 77-year-old Cynthia Beaudoin can do. Tom Moore picks up her groceries from a list and delivers them to her apartment.
A home health aide greets him at the door. Beaudoin remains on the couch, her walker nearby and an emergency call button hanging around her neck. Her life’s been like this since she was in the hospital a few years ago.
When she was discharged, she didn’t want to go to a rehab hospital. “I just wanted to come home directly,” recalls Beaudoin.
Beacon Hill Village was able to connect her with the right services to make it possible for her to return to the apartment she’s lived in for 36 years. It has a view of the Charles River that no one would want to leave.
But for Beaudoin, Beacon Hill Village is more than the sum of its services. “It’s comforting,” she says. “That’s one of the most important things.”
A village for everyone
At her Chicago block party, Debra Thompson cannot be ignored, with her dyed blond hair and a bright yellow T-shirt. She calls out to everyone, hoping they’ll fill out her survey so she can find out what they need. And Englewood seniors have a lot of needs. Nearly half of the people in this African American neighborhood live below the poverty line. But many of them have no idea that there are public services that might help them. Thompson wants to change that.
And she persists even when some people are reluctant to put their names on anything.

A local hardware store is seen in the Englewood neighborhood on Chicago’s South Side.
Kristen Norman/NPR
hide caption
toggle caption
Kristen Norman/NPR
A woman named Bessie Stovall says “my children say don’t sign nothin’ unless I know what I’m signing.”
Thompson reassures her. “This is not a contract.” She explains that Englewood Village can connect her with services to help find a job, for instance, or a place to stay. “Oh yeah, I need a job,” says Stovall. Suddenly, she’s happy to fill out the form and Thompson directs her to an upcoming job fair that focuses on employment for seniors.
Thompson also passes out information on a lottery for free roof repairs, discounts on utilities, and tells people about a service that can help frail older people remain in their homes.
Frances Shedd, 80, knows all about that one. Years ago, she worked for a government service that provides homemaker assistance to older adults up to 12 hours a week. Now she watches the party from her porch, accompanied by her own homemaker, Quintechette Jones.
“I keep everything clean in her atmosphere,” says Jones. “I make sure she gets her nutrition. I groom her sometimes. And then we sit and chat.”

Frances Shedd, 80, seated, with her home aide Quintechette Jones.
Ina Jaffe/NPR
hide caption
toggle caption
Ina Jaffe/NPR
Shedd thinks it’s great that the Englewood Village is telling more people about this service. “When you get to a certain age,” she explains, “you need somebody to see after you because we don’t feel good when we get up in the morning.”
Another observer of the block party is Joyce Gallagher and she likes what she sees. She’s Chicago’s deputy commissioner for senior services. Gallagher loved the Village concept from the first time she heard about it and wanted every older adult to have access to such a supportive community. The hang-up was the dues. The Chicagoans who could benefit the most from a Village, couldn’t fork over a few hundred bucks a year on top of paying for services.
Then Gallagher had her lightbulb moment. What were the dues for? They paid for office space and computers and phones. But her department already had all of that in its 21 senior centers. The city could donate the office space and equipment. But she didn’t want this to be a city-driven program. She envisioned the villages being grass roots organizations run by volunteers. As for services, those would come from government programs available to low-income seniors.
So Gallagher began to call meetings at senior centers around the city to see if anyone was even interested in becoming part of this. She had no expectations about how she’d be received. “You have someone coming from the outside, and saying ‘Listen, we’ve got no proof that this is going to work, but we really feel that you deserve this, that every community deserves this, … are you interested?'”
In Englewood, Debra Thompson was interested. In fact, the Village has become her cause. “I devote every day to my seniors,” she says. “I’m always looking for ways and partnerships and issues that can assist us to assist them in achieving what they need.”

Old victorian style homes are seen along Garfield Blvd. in the Englewood neighborhood on Chicago’s South Side.
Kristen Norman/NPR
hide caption
toggle caption
Kristen Norman/NPR
Thompson’s early enthusiasm is the reason that Englewood is the oldest village in the Chicago system. Currently, there are just six city-wide. Each one operates out of a different senior center. Gallagher wants to have villages reaching out to all 21 neighborhoods where senior centers are located by the end of next year.
A big dependence on government services could make the project vulnerable to the whims of state and federal budget-makers. But Gallagher says that’s not the only focus: volunteers in each village set their own agendas. One is centered on gentrification, another on preventing financial scams targeting seniors, while a third concentrates on dealing with emotional trauma caused by that neighborhood’s many shootings.
People continued to stop by Debra Thompson’s block party even after the hot dogs were gone. Over the course of the afternoon, she signed up close to 50 people who hadn’t known about Englewood Village before. For Thompson, that was one sign that the afternoon had been a success. Another sign? Some people invited her to throw block parties on their streets, making Thompson hopeful that Englewood Village will continue to grow.
Reaching seniors out of reach
Plumas County, Calif. is about the size of Connecticut, with about 19,000 people. It’s in the Sierra Nevada Mountains in northeastern California. There’s no interstate highway, not a lot of chain stores, hardly any stoplights, but lots of pine trees.
“When you live out here, you have to be ready for the winter,” says 75-year-old Jimmie Oneal.
And preparing for the snow and cold is what Oneal is doing on this late autumn afternoon. She directs a handful of volunteers who’ve come to ferry stacks of firewood from a garden shed up to her back porch.
That firewood will help Oneal heat her home when the cold is so severe that her propane heater just isn’t enough.
Both Oneal and the volunteers helping her are members of Community Connections, Plumas County’s version of a Village. It works on what’s known as a time bank model. Members get credits in their time bank accounts for helping each other. Then when they need some help themselves, they draw on those credits to “pay” for the service. And in Plumas County, those services run the gamut from helping to clear trees to serving food at a wedding to teaching welding and other building skills.
Oneal lives alone in a little dome house on a heavily wooded acre of land that slopes down to a creek. Since her husband died eight years ago, help from Community Connections volunteers has been crucial to her ability to remain here. She’s still had to make some changes though: she gave up her chickens.
“I was having to carry buckets of water [for the chickens] down that hill in the wintertime and it gets really icy,” she says. “I finally decided that one bad fall could be real bad news for me. So I decided to find homes for my chickens. And I still miss ’em.”
If Oneal had a bad fall, her options in Plumas County would be limited. There’s only one assisted living facility. It can accept just 4 residents. There are no vacancies. The beds are also full at the two small nursing homes. So around here, helping seniors live independently isn’t just matter of what they want, it’s almost the only option.
And Oneal says she has her own way of contributing to the time bank for the help she receives from Community Connections.
“I guess you could say I’m sort of like a granny. People come to me with all kinds of questions: about gardening, about chickens, about trees, about how to survive with the cold, especially people who haven’t been here that long,” she says.
Community Connections is run by Plumas Rural Services, a large non-profit social services agency. Dues are just $10 a year. Anyone can join. The youngest member is 7 years old, the eldest is 93.
Leslie Wall has run Community Connections since it began 10 years ago. Back then, she wanted to find out what older people wanted from the program.
“We expected seniors would want transportation,” she recalls, “and they would want visitors, and someone to call them weekly. And what we found was the greatest need of our seniors was to be needed. We have seniors who want things to do that are vital, that matter, that make a difference.”
Seventy-seven-year-old Pat Evans’ skills as a seamstress make a difference to Karon Chance. Evans does almost all of the Chance family’s mending, which leaves Karon Chance more time to build her catering business.
Now, Chance believes she has brought Evans a real puzzle. The backing of a cherished old quilt is shredding. It needs to be removed and replaced. But for Evans it’s no problem. As the two women pour over the quilt, Evans explains what kind of replacement fabric will be needed and a couple of different stitching techniques she could use.
There’s nothing like experience. Pat Evans has been sewing since she was 10 years old: made her own clothes, her wedding dress, her late husband’s sport coats, her kids’ clothes. Now she lives alone and sews for her fellow members of Community Connections. Karon Chance says that’s benefited both of them in ways they hadn’t planned.
“Sometimes we just catch up and talk about the dog and about the flowers,” she says. “Pat and I might never have crossed paths, if it weren’t for Community Connections. And now I’ve made a friend.”
Which is an unexpected dividend of credits in the time bank.
What Are The Two Health Bills Sen. Susan Collins Wants Congress To Act On?

Maine Sen. Susan Collins voted for the Senate GOP tax plan despite its repeal of the individual mandate because GOP leadership promised her a vote on her reinsurance bill, and a vote on legislation to restore some payments to insurers. But it’s doubtful getting those provisions enacted would mitigate the damage to exchanges from the mandate repeal.
Heading North: American Doctors Report Back From Canada

Sen. Bernie Sanders, the Vermont independent, joined protesters outside the U.S. Capitol in late November, as Republicans in the Senate worked to pass a sweeping tax bill.
J. Scott Applewhite/AP
hide caption
toggle caption
J. Scott Applewhite/AP
For Peter Cram, an American internist who spent most of his career practicing in Iowa City, Iowa, moving to Toronto in 2014 was an easy decision.
He says he is among a handful of American doctors who went north to practice in Canada’s single-payer system. Now he doesn’t worry about whether his patients can afford treatment. “Everyone gets a basic level of care,” he says, which lets him focus on their medical needs instead of their finances.
Cram treats his move as a sort of life-size experiment. As an American-trained physician and a health system researcher, he is now studying how the United States and Canada – neighbors with vastly different health systems – compare in terms of results. Does one do a better job of keeping people healthy?
For all the political talk, it’s in many ways still an unresolved question.”The Canadian system is not perfect,” Cram said over coffee in Toronto’s Kensington Market. “Anyone who gives you a sound bite and says this system should be adopted by [the U.S.] … I think they’re being almost disingenuous.”
Still, American support for government-run single-payer health care, once a fringe opinion, is picking up momentum. Sen. Bernie Sanders, the Vermont independent who emphasized single-payer health care in his 2016 presidential bid, helped move Canada’s system into the U.S. spotlight.
Polls find that doctors and patients increasingly support single-payer, though the percentages in favor typically drop when questions are focused on paying for such a system.
In Canada, medical insurance is publicly funded. While covering everyone, Canada still spends far less on health care than the United States: just over 10 percent of its GDP, compared with the United States’ 16 percent.
To American advocates, Canada’s health system sounds like an answer to the United States’ challenges.
But in Toronto, experts and doctors say the United States would first have to address a fundamental difference. In Canada, health care is a right. Do American lawmakers agree?
James Sugiyama, a Toronto-based doctor, watched Sen. Sanders’ speech on livestream from a restaurant down the street. The Vermont senator is viewed as a “folk hero” by many Canadians, he said.
Shefali Luthra/KHN
hide caption
toggle caption
Shefali Luthra/KHN
“The U.S. needs to get on with the rest of the world and get an answer on that issue before it answers others,” said Dr. Robert Reid, a health quality researcher at the University of Toronto, who has practiced medicine in Seattle.
It’s an obvious disconnect, said Dr. Emily Queenan, a family doctor now practicing in rural Ontario. Queenan, 41, grew up in the United States and did her residency in Rochester, N.Y. In 2014, after five years of frustrating battles with insurance companies over her patients’ coverage, she found herself asking, why not Canada?
She moved north. Gone, she said, are the reams of insurance paperwork she faced in America. Her patients don’t worry about affording treatment. “We have here a shared value that we all deserve access to health care,” said Queenan. “That’s something I never saw in the States.”
Canadian doctors may earn less than do their American counterparts: A 2011 paper published in the journal Health Affairs found that primary care doctors and surgeons alike make more in the United States than in most other western countries. That’s in part because, overall, American doctors charged more for each service they provide, and in part because they performed more of them.
Critics argue that’s a sign of American inefficiency in paying for health care.
The fee gap is greatest for surgeons. Family doctors in Canada appear to charge similar amounts to their American counterparts.
Meanwhile, the doctors interviewed for this story — internists and family doctors – said they didn’t experience any real change in their standard of living when moving north.
Sanders has pushed the single-payer discussion with a “Medicare-for-All” bill in Congress and in a visit to Toronto this fall. It was part fact-finding mission and part publicity tour. On that trip, doctors, hospital leaders and patients painted a rosy picture of Canada as a place where everyone gets top-notch care, with no worries about its cost to them.
“They have managed to provide health care to every man, woman and child without any out-of-pocket cost,” Sanders told reporters on the ground floor of Toronto General Hospital.
The reality is more complicated.
While progressives tout Canada for efficiently providing universal health care, the Commonwealth Fund puts it just two spots above the United States — which ranks last among 11 developed countries— in the group’s health system assessment. Canada still has room to improve in timeliness, health outcomes and equitable access to care.
“If you deny there are trade-offs, I think you’re living in wonderland,” Cram said.
The Canadian Vibe
In Canada, everyone gets the same, government-provided coverage. Provinces use federal guidelines to decide what’s covered, and there’s no cost sharing by patients.
“Come to our waiting room,” said Dr. Tara Kiran, a family doctor at St. Michael’s Hospital, in Toronto. “You will see people who are doctors or lawyers alongside people who are homeless or new immigrants. People with mental health issues or addiction issues together with people who don’t.”
But that insurance — which accounts for 70 percent of health spending in Canada —addresses only hospitals and doctors. Prescription medications, dentists, eye doctors and even some specialists aren’t covered. Most Canadians get additional private insurance to cover those.
In countries such as Britain or Germany, people can opt out to buy private insurance. Canada prohibits private insurers from offering plans that compete with the government, a restriction some doctors are suing to lift.
In Canada, the debate focuses more on bringing down health spending. Canada’s provinces put, on average, 38 percent of their budgets into health care, according to a 2016 report from the Canadian Institute for Health Information, a nonprofit organization. Canada’s single-payer system is supported by a combination of federal and provincial funds, mostly raised through personal and corporate income taxes. (A few provinces charge premiums, which are based on income and collected with taxes.)
“We make improvements or change things only to have additional debates about other things. Those debates are constant, and they should be,” said the University of Toronto’s Reid. “[But] most of what you hear in the U.S. is back to the tenor of the insurance framework, whether [they] should have Obamacare or not.”
Taxes in Canada are generally higher than in the United States. But many here call that a concession worth making. “We can’t have what we have if we don’t pay the taxes,” said Brigida Fortuna, a 50-year-old Toronto resident and professional dog groomer, while on her way to a medical appointment.
The Trade-Offs
That said, it’s not a perfect system. Canadian health care doesn’t cover prescriptions, physical therapy and psychotherapy. And there’s the concern that Canadians wait longer for health care than would Americans with robust health coverage.
There are cases, Reid said, when cancer care in Canada is delayed enough to yield health problems. Expat Cram pointed to research that suggests low-income people are likely to wait longer for medical care, which can result in worse health outcomes.
“We do have a two-tiered system,” he said. “Most know it. Few will admit it.”
Typically, experts said, people with serious medical needs will jump to the front of the line for medical care. Kathleen Wynne, Ontario’s Liberal premier, said the Canadian government is actively trying to improve wait times.
But so far, it’s unclear how effective that’s been. A 2017 report from the nonprofit Canadian Institute for Health Information found that wait times had dropped for hip fracture repairs. But waits for, say, MRIs and cataract surgery have gotten worse. Depending on the province, the average wait for cataract removal ranged from 37 days to 148 days.
Many patients, though, said the waits were a trade-off they were willing to make. Toronto-based Nate Kreisworth, a 37-year-old music composer and producer, called it an obvious choice.
“You are not going to die because you’re waiting,” he said on a recent sunny morning while walking with his dog near Kensington Market. “Better wait times for everything? Sure, why not. But as long as the major issues are being covered, then I don’t think it’s really much of an issue.”
As Fortuna put it: “If you go for a headache and someone else is going to lose their arm, of course they’re going to take care of that person. I’m OK with that, because someday that could be me, too.”
Waits aren’t the only concern, though. There’s financing – and what it would cost for the United States to implement a system like Canada’s.
Because Americans have higher expectations about what a health plan should cover, it would be more expensive to adapt a Canadian approach, said Dr. Irfan Dhalla, an internist and health quality researcher in Toronto. And the quality may differ from what they are used to.
In Canada, “everyone gets Kmart care,” Cram said. “There’s no Neiman Marcus care.”
Of course, some American amenities that drive up costs — fancier food, softer gowns or private rooms — don’t necessarily produce better results
And there’s perhaps the bigger question: Experts don’t really know whether the Canadian system is an obvious improvement.
The research is limited, and not always recent. A 2006 paper suggests wealthy Canadians and Americans fare similarly, while poor Americans do worse. A 2007 paper found Americans more often liked their quality of health care. More recent research focuses on specific conditions – cystic fibrosis patients did better in Canada, while surgical outcomes were better in the United States. The Commonwealth Fund’s most recent ranking places Canadian health outcomes above America’s, but only two positions higher.
Even so, many Canadians said they couldn’t imagine living with an American system. It’s a question not just of efficiency, but of fairness. Kreisworth compared his experience to that of family members in the United States.
“I talk to my brother’s girlfriend who is a part-time worker who has no [health] benefits — who would just be sick and not go to the doctor because she couldn’t afford to pay,” he said. “I can’t imagine that here. It seems like — it’s so wrong. It just seems utterly wrong.”
Kaiser Health News (KHN) is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
CVS Health CEO On Aetna Deal
Steve Inskeep talks with Larry Merlo, CEO of CVS Health, about his company’s acquisition of the giant insurer Aetna.
Consumers Hunting For Health Insurance Find High Prices — And Some Great Deals
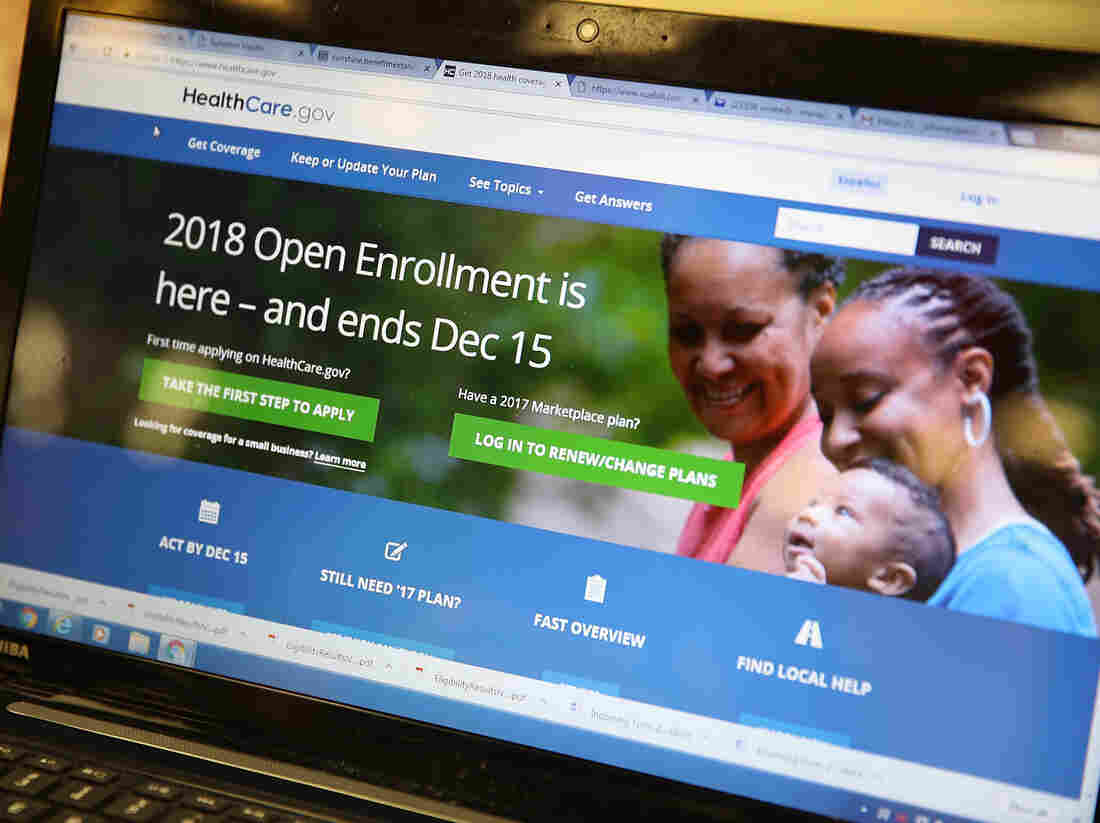
The homepage of the Affordable Care Act exchange on Nov. 1, 2017 in Miami. The open enrollment period to sign up for a health plan on HealthCare.gov runs through Dec. 15; several states with their own health care exchanges have later deadlines.
Joe Raedle/Getty Images
hide caption
toggle caption
Joe Raedle/Getty Images
Gene Kern, 63, retired early from Fujifilm, where he sold professional videotape. “When the product became obsolete, so did I,” he says, “and that’s why I retired.”
Kern lives in Frederick, Md., and has been an enthusiastic enrollee in Maryland’s health exchange since it began in 2014. But this fall he received a letter from his insurer explaining that the cost of his policy’s premium would jump from $800 a month to $1,300 in 2018.
Premiums have risen for many 2018 policies, though most people won’t actually have to swallow those higher costs, because subsidies have gone up, too. Gene Kern is one of the exceptions.
“Because of my income, I am slightly above the 400 percent poverty level,” he says, “and as a result I get no subsidy from the government.”
So Kern has switched to an HMO plan on the insurance exchange for around $900 a month. That’s more than 20 percent of his income, which comes partly from Social Security and partly from his retirement account. But, he says, “It’s the best I can get,” and he wants very much to stay insured for the next two years, at which point he will qualify for Medicare.

Gene Kern of Frederick, Md., shops for health insurance on the ACA exchange. The monthly premium for his policy is going up this year, he says, and he does not qualify for subsidies.
Selena Simmons-Duffin / WAMU
hide caption
toggle caption
Selena Simmons-Duffin / WAMU
Louise Norris is a health insurance broker and analyst in Colorado. She says there are a number of people like Kern who earn too much for a subsidy and will pay more for health insurance next year than they did in 2017. “Rates are high,” she says. “There’s no way to sugarcoat that.”
But she warns her clients against the temptation to get a less expensive plan that doesn’t comply with the minimum standards set out by the ACA.
“It seems like a good deal because it’s cheap,” Norris says. “But then you find yourself being that person who has a heart attack and needs triple bypass. And hundreds of thousands of dollars later you wish you had that ACA-compliant plan.”
Prices for ACA-compliant health policies went up in Tennessee, too, where state regulators approved average rate increases ranging from 20 to 40 percent.
Brenda Linn has already been paying $750 a month just to cover her own medical needs; so the retired kindergarten teacher and her husband logged on to HealthCare.gov to check the price of 2018 plans. To her surprise, the website brought up a great deal.
“And I’m like, ‘Dave, this has to be a mistake,’ ” she says. The price Linn was quoted was less than $5 a month. Why? A slight loss of income had made her eligible for a subsidy for 2018. “Because we didn’t qualify last year, I wasn’t really that hopeful,” Linn says.
But a large majority of marketplace shoppers do get subsidies. And for 2018, on aggregate, these subsidies are larger.
Tony Garr, a volunteer application assistant with the Tennessee Health Care Campaign, says more than ever this year, people should shop around on the exchange to see what kind of subsidies they may be eligible for.
“Generally speaking, they will find out that help is there,” he says.
Any many people who got a price break in the way of a subsidy in the past can get even more for their money this year.
For example, Daniel Prestwood, who is self-employed and cleans fish tanks around Nashville, says he found a better plan for 2018, with monthly premiums that dropped from $300 to $200. He says he tries not to get too frustrated by the political wrangling over health care.
“All I know is that for 2018 I’ll have a good health care plan in place,” he says, “and that’s the best I can hope for at this point.”
And even with the Trump administration’s efforts to hobble the ACA, in Tennessee, the number of applications processed by federally funded insurance guides — known as navigators and certified application counselors — has already surpassed last year’s. As of early last week, with 10 days left in open enrollment, more than 1,200 individuals had applied with official help, eclipsing the total from all of 2016, when the enrollment period was several weeks longer.
While application assistants only work with a tiny fraction of the 235,000 Tennesseans who have marketplace plans, Sandy Dimick of Family and Children’s Services Nashville, says she expects total enrollment will exceed last year’s total, as well. Navigators around the U.S. have worried that cuts to the federal advertising budget in 2017, and a lack of cheerleading from the White House, could drive down enrollment.
Take note: Though enrollment for most states ends Friday night, residents of eight states (California, Colorado, Connecticut, Massachusetts, Minnesota, New York, Rhode Island and Washington) and the District of Columbia have slightly more time to sign up.
This story is part of NPR’s reporting partnership with local member stations and Kaiser Health News. Selena Simmons-Duffin, a producer at NPR’s All Things Considered, is working temporarily with NPR member station WAMU, as part of an exchange program at the network. Blake Farmer can be found on Twitter @FlakeBarmer.
HealthCare.gov Enrollment Ends Friday. Sign-ups Likely to Trail Last Year's

Isabel Diaz Tinoco and Jose Luis Tinoco had some questions for the Miami insurance agent who helped guide them in signing up for a HealthCare.gov policy at the Mall of the Americas in November.
Joe Raedle/Getty Images
hide caption
toggle caption
Joe Raedle/Getty Images
Friday is the last day to enroll in a health insurance plan through the federal government’s insurance exchange, HealthCare.gov.
And in a little office park in Northern Virginia, Brima Bob Deen is dealing with the rush.
He is the president of a church-sponsored job training center called Salvation Academy. But this time of year, he acts mostly as an enrollment counselor for Affordable Care Act health plans.
And this week, his calendar is full.
“Every year when you get close to the end, that’s when you have a lot of people come in,” he says.
Deen has stopped allowing people to stand in line outside his office and instead now requires them to make an appointment. That way, he says, he can give them his full attention, rather than being distracted by impatient people waiting.
As we sit to talk, a client calls with an update. The man had been rejected by the HealthCare.gov system because of issues with his email. He tells Deen that his son has helped him resolve the problem.
“Yesterday I have a client and she has difficulty in choosing a plan based on her tax credits and her qualifications,” Deen says. “She has this bunch of plans — there’s silver, there’s gold, and she’s just confused.”
As of Sunday, about 4.7 million people had enrolled in a health plan and more than a million of them were new customers. That’s about 650,000 more than signed up in the first six weeks of last year, according to Lori Lodes, who ran outreach for HealthCare.gov during the Obama administration and is now leading an effort called Get America Covered.
“We are seeing record demand,” Lodes says. “People want to get health coverage, and people are finding affordable coverage when they actually shop and sign up.”
“The problem is that the enrollment period is cut in half,” she adds.
Friday is the deadline, at least for people buying insurance through the federal marketplace. Several states run their own exchanges and those enrollment periods usually last longer.
The Department of Health and Human Services earlier this year cut the enrollment period, arguing that the shortened period would likely reduce the number of people who buy insurance only when they get sick. And the agency also cut the budget for outreach and advertising for HealthCare.gov by 90 percent.
Trump administration officials declined requests for an interview on this year’s changes to enrollment. But a spokesman says the HealthCare.gov website and call centers are working smoothly and handling the final week’s volume.
Lodes’ group has been enlisting big names to help drum up awareness, including a YouTube video featuring West Wing actors Martin Sheen and Bradley Whitford.
“We are both here to remind you about the Affordable Care Act,” they say. “And here’s what you need to know. You gotta sign up!”
Former President Barack Obama has been on Twitter reminding people to enroll.
“It’s up to all of use to spread the word. Sign up through this Friday,” he tweeted.
Just got off a call to thank folks who are working hard to help more Americans across the country sign up for health coverage. But it’s up to all of us to help spread the word: Sign up through this Friday at https://t.co/ob1Ynoesod. https://t.co/8TYpLCestp
— Barack Obama (@BarackObama) December 11, 2017
And earlier this week, comedian Jimmy Kimmel gave HealthCare.gov a plug on his show.
“Obamacare is not dead,” he said, while holding his son, who recently underwent surgery, on his hip. “It’s very much alive. Millions of people qualify for a reduced rate or even totally free plans.”
Forum: Examining Discrimination Against Native Americans
iStockphoto.com/GracedByTheLight
Editor’s note 1:13 p.m.:The webcast is over. We’ll update the post with an archived video when it becomes available.
How do Native Americans experience discrimination in daily life?
A poll by NPR, the Robert Wood Johnson Foundation and the Harvard T.H. Chan School of Public Health is examining the extent of discrimination against five major ethnic and racial groups in America today. It finds that Native Americans experience very high rates of discrimination in everyday life.
More than a third of Native Americans and their family members have experienced slurs and violence, and close to a third have faced discrimination in the workplace and when interacting with the police. Native Americans who live in majority-Native American areas are significantly more likely to experience this kind of discrimination, the poll finds.
The results for Native Americans in the poll were released earlier this fall and will be highlighted in an expert panel discussion to be live-streamed here at 12 p.m. ET Tuesday, Dec. 12, as part of The Forum at the Harvard Chan School.
With unprecedented documentation, the poll provides results from police interaction, job applications, health care, racial slurs and more. The Forum will explore the results and their implications for society.
This poll is examining discrimination among African-Americans, Latinos, whites, Asian-Americans, women, and LGBTQ adults on their experiences with discrimination.
Joe Neel, deputy senior supervising editor on NPR’s Science Desk, will moderate the discussion with:
Robert Blendon, professor of health policy and political analysis, Harvard T.H. Chan School of Public Health and Harvard Kennedy School
Stephanie Fryberg, associate professor for American Indian studies and psychology, University of Washington
Michael Painter, senior program officer, Robert Wood Johnson Foundation, and former chief of medical staff at the Seattle Indian Health Board
Yvette Roubideaux, director of the National Congress of American Indians Policy Research Center and former director, Indian Health Service
Our ongoing series “You, Me and Them: Experiencing Discrimination in America” is based in part on a poll by NPR, the Robert Wood Johnson Foundation and the Harvard T.H. Chan School of Public Health. We have released results for African-Americans, Latinos, Asian-Americans, whites, Native Americans and women.
Deadline Is Friday For Most ACA Insurance Sign-Ups, With Important Exceptions

A week after Hurricane Harvey swept through southern Texas in August, the streets of Katy, Texas were still flooded. People in the Puerto Rico and the Southeastern U.S. who were affected by the hurricanes are among those who may have extra time to enroll for 2018 health plans.
Justin Sullivan/Getty Images
hide caption
toggle caption
Justin Sullivan/Getty Images
Open enrollment on the federal health law’s marketplace — HealthCare.gov — ends Friday, and most people who want a plan for next year need to meet the deadline.
But some consumers who miss the cutoff could be surprised to learn they have the opportunity to enroll later.
“While a lot of people will be eligible … I am still worried that a lot of consumers won’t know it,” says Shelby Gonzales, a senior policy analyst at the Center on Budget and Policy Priorities.
Under the health law, people are entitled to a special enrollment period when they have specific changes in their lives — such as losing other health insurance, getting married or having a child, or when they have a change in income that affects their eligibility for premium tax credits or cost-sharing reduction subsidies.
Those special enrollment periods generally last at least 60 days.
Other circumstances can also qualify customers for a special enrollment period. But this year, consumer advocates are focused on two that could affect a substantial number of people: consumers whose 2017 marketplace policies are being discontinued in 2018 and people affected by the hurricanes that ravaged Texas, parts of the Southeastern United States and Puerto Rico.
It’s not clear how many consumers this will affect. In past years, people who signed up during a special enrollment period made up a tiny fraction of overall marketplace enrollment.
In the spring of 2016, 11.1 million people had a marketplace plan. Meanwhile, roughly 1.6 million signed up through a special enrollment period during 2015, according to the federal Centers for Medicare & Medicaid Services.
The majority of people who use a special enrollment period do so because they’ve lost coverage under another plan. This applies to people who lose their job-based coverage as well as those with marketplace plans whose insurer discontinues their plan for the upcoming year.
Between 2014 and 2018 the average number of issuers per state declined from 5 to 3.5. Several leading insurance companies, including Anthem, Aetna and Humana, dramatically pulled back in their 2018 offerings.
A growing proportion of people will likely qualify for special enrollment periods now, insurance analysts say, because of a loss of marketplace coverage.
People who are eligible have up to 60 days after their coverage ends on Dec. 31 to sign up for a new marketplace plan. Meeting the regular Dec. 15 sign-up deadline is preferable because it allows coverage to start Jan 1. But eligible people who miss that date can apply through the marketplace for a special enrollment period that will allow them to sign up until the end of February.
Even if the marketplace automatically re-enrolls customers in a plan that’s similar to the one that ended, they’re entitled to a special enrollment period to pick a new policy.
Gonzales fears consumers may not immediately realize that.
“The bottom line here is many consumers experienced a discontinuation of their plan this year,” she says. “Notices are complicated, and these consumers in particular are going to get several notices which may result in more confusion, and it will not be easily understood by many what an S.E.P. [special enrollment period] is, or how and/or when to activate it.”
This year, there are also special enrollment periods for people who were affected by the hurricanes that moved across all or parts of Texas, Florida, Georgia, Puerto Rico and elsewhere last fall.
The special enrollment period for 2018 applies to people who live in or move from counties designated by the Federal Emergency Management Agency as hurricane disaster areas. It gives them an extra two weeks — from Dec. 16 to Dec. 31 — to sign up for January coverage. Officials say they’ll consider extending the timeframe if necessary.
To take advantage of the special enrollment period, people must request it through the HealthCare.gov call center. They’ll be asked to attest that they resided in an affected area, but they won’t have to provide proof.
Consumer advocates who work on outreach for enrollment and help people sign up for coverage aren’t yet talking up the special enrollment periods, says Gonzales.
“They want one clear message for everyone: Open enrollment ends Dec. 15,” she says. Starting Dec. 16, these groups will start getting the word out for people who have missed the deadline and don’t realize they may still have other options.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Follow Michelle Andrews on Twitter: @mandrews110.
Native Americans Feel Invisible In U.S. Health Care System

Anna Whiting Sorrell, a member of the Confederated Salish and Kootenai Tribes in northwest Montana, had hernia surgery a couple of years ago. The Indian Health Service picked up a part of the tab for the surgery but denied coverage for follow-up appointments.
Mike Albans for NPR
hide caption
toggle caption
Mike Albans for NPR
The life expectancy of Native Americans in some states is 20 years shorter than the national average.
There are many reasons why.
Among them, health programs for American Indians are chronically underfunded by Congress. And, about a quarter of Native Americans reported experiencing discrimination when going to a doctor or health clinic, according to findings of a poll by NPR, the Robert Wood Johnson Foundation and Harvard T.H. Chan School of Public Health.
Margaret Moss, a member of the Hidatsa tribe, has worked as a nurse for the Indian Health Service and in other systems. She now teaches nursing at the University of Buffalo.
She says she has seen racism toward Native Americans in health care facilities where she’s worked, and as a mom trying to get proper care for her son.
Once, when she was on a health policy fellowship with a U.S. Senate committee, Moss’ son had a broken arm improperly set at a non-IHS health facility in Washington, D.C.
She asked the physician about options to correct it, but he told her it was fine, she said. “Even when I, as an educated person using the right words was saying what needed to happen, [he] didn’t want to do anything for us even though we had a [health insurance] card.”
Moss then reluctantly pulled out a business card with the Senate logo, she recalled, and was instantly transformed in the doctor’s eyes from “this American Indian woman with my obviously minority son” to someone he could not afford to dismiss.
“It wasn’t until the person … felt they could get in trouble for this … then the person did something,” said Moss. “I felt like it was racism. Not everybody has a card they can just whip out.”
She says she feels discrimination is more overt, “in areas where American Indians are known about,” like the Dakotas and parts of the American Southwest, but also exists in places without big tribal populations.
In the NPR poll, Native Americans who live in areas where they are in the majority reported experiencing prejudice at rates far higher than in areas where they constituted a minority.
In places where there are few American Indians, Moss says, “people don’t expect to see American Indians; they think they are from days gone by, and so you are misidentified. And that’s another form of discrimination.”
Health care systems outside the Indian Health Service generally see very few Native American patients, because it’s so hard for American Indians to access care in the private sector. A lot of that has to do with high poverty and uninsured rates among American Indians, who also often live in rural areas with few health care providers.
“The strikes against people trying to get care are huge: geographic, transportation, monetary,” Moss says.
A persistent myth inside and outside Indian Country is that Native Americans get free health care from the federal government.
“I hear that all the time,” says Moss, sighing.

Sorrell started exercising and going on walks after her experience with hernia surgery.
Mike Albans for NPR
hide caption
toggle caption
Mike Albans for NPR
The federal government promised to take care of Native Americans’ health when it signed the treaties in which tribes gave up almost all of their land.
“Unfortunately, they have not kept up their end of the bargain,” Moss says.
Congress has long failed to allocate enough money to meet Native American health needs. In 2016 it set the Indian Health Service budget at $4.8 billion. Spread across the US population of 3.7 million American Indians and Alaska Natives, that’s $1,297 per person. That compares to $6,973 per inmate in the federal prison system.
Moss says the IHS can be less an aid to people than another bureaucratic barrier. “It is highly complicated,” Moss says, “even if you took out the racism, perceived or real.”
The IHS isn’t insurance. It’s more like the Veterans Administration, running clinics and hospitals where its members can get care. But the IHS is far smaller than the VA.
Federal funding is also supposed to pay for care in the private sector that IHS hospitals can’t provide. But, quoting a sardonic joke familiar to many in Indian Country, Moss says it’s well known that “you’d better get sick by June, because there won’t be any more money, or it’s life and limb only, those are the things that would be authorized.”
Anna Whiting Sorrell, a member of the Confederated Salish and Kootenai Tribes in northwest Montana experienced that firsthand. The IHS picked up part of the tab for her hernia surgery at a hospital outside of the IHS a couple of years ago, but when it was time to schedule follow-up appointments, Sorrell was out of luck.
“It got denied. My follow-up got denied,” Sorrell says. “[The hospital] didn’t even ask if I was willing to pay,” she says, and that felt like discrimination. “They would assume that other non-Indians would pay for it themselves, why do we as Indian people not get to make those decisions ourselves?” Sorrell asks.
She felt like she was falling through a crack in the health care system at a particularly poignant time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anna and her husband, Gene Sorrell, outside their home in Evaro, Mont. Anna eventually received follow-up care for her surgery, but the process took years.
Mike Albans for NPR
hide caption
toggle caption
Mike Albans for NPR
“I was 57 years old. My mom died at 57,” Sorrell says. In Montana, the life expectancy for Native American women is 62, that’s 20 years less than for non-Native American women. The life expectancy for Native American men in Montana is 56.
With help from her tribe, Sorrell eventually got her follow-up care, but her journey from diagnosis to actually getting surgery took years, and the University of Buffalo’s Margaret Moss says a lot of Native Americans just give up.
“That is the idea out there in Indian Country … , ‘I’m not even going to try, because it’s not going to happen.’ Or they hear so many stories of people who did try, and it didn’t happen,” Moss says.
That means a lot of American Indians simply put up with what she calls, “tolerated illness.
“They say they’re fine, but they’re not,” Moss says, and their health problems often progress until it’s too late for treatment to help.
Anna Whiting Sorrell, a health care administrator for her tribes, says she is optimistic that the Affordable Care Act will make a big difference for Native Americans. It gives lower-income people access to affordable insurance coverage outside the IHS. Many Natives Americans who weren’t eligible for Medicaid before the ACA now are, too.
Moss is more skeptical that the ACA will make a big difference, in part because of entrenched institutional discrimination toward Native Americans in healthcare.
“Until attitudes change,” Moss says, “we’re still going to be in a sad situation.”
Our ongoing series “You, Me and Them: Experiencing Discrimination in America” is based in part on a poll by NPR, the Robert Wood Johnson Foundation and the Harvard T.H. Chan School of Public Health. We have previously released results for African-Americans, Latinos, Asian-Americans, whites and women.
You can follow Montana Public Radio’s Eric Whitney on Twitter: @MTPRND