A Prescription To Reduce Waste In Health Care Spending

Earlier this year, the Gallup organization set out to identify the top concerns everyday Americans have about money. Researchers asked more than a thousand people across the country, “What is the most important financial problem facing your family today?” Their top answer: the cost of health care.
Increases in medical costs have substantially outpaced economic growth for decades. In recent months, ProPublica has shown that it doesn’t have to be this way. It’s been estimated that the U.S. health care system wastes about $765 billion a year — about a quarter of what’s spent. We’ve identified ways that tens of billions of dollars are being wasted, some of them overlooked even by many experts and academics studying this problem.
It’s possible to reduce or eliminate some of the waste, but there are also formidable forces that benefit from it. Excess spending generates revenue and profit for what some have called the “medical industrial complex,” said Dr. H. Gilbert Welch, professor of medicine at the Dartmouth Institute for Health Policy & Clinical Practice. “There are a number of people who can imagine ways to solve things,” Welch said of the wasted spending. “But the political will and the forces at work can stop them pretty easily.”
Still, wasting fewer health care dollars could drive down insurance premiums and out-of-pocket costs and maybe even free up resources for education, retirement and wage increases, among other things.
Here are the ways ProPublica found the medical industry is needlessly gobbling up money, along with steps health care leaders or policymakers say we could take right now to reduce the waste.
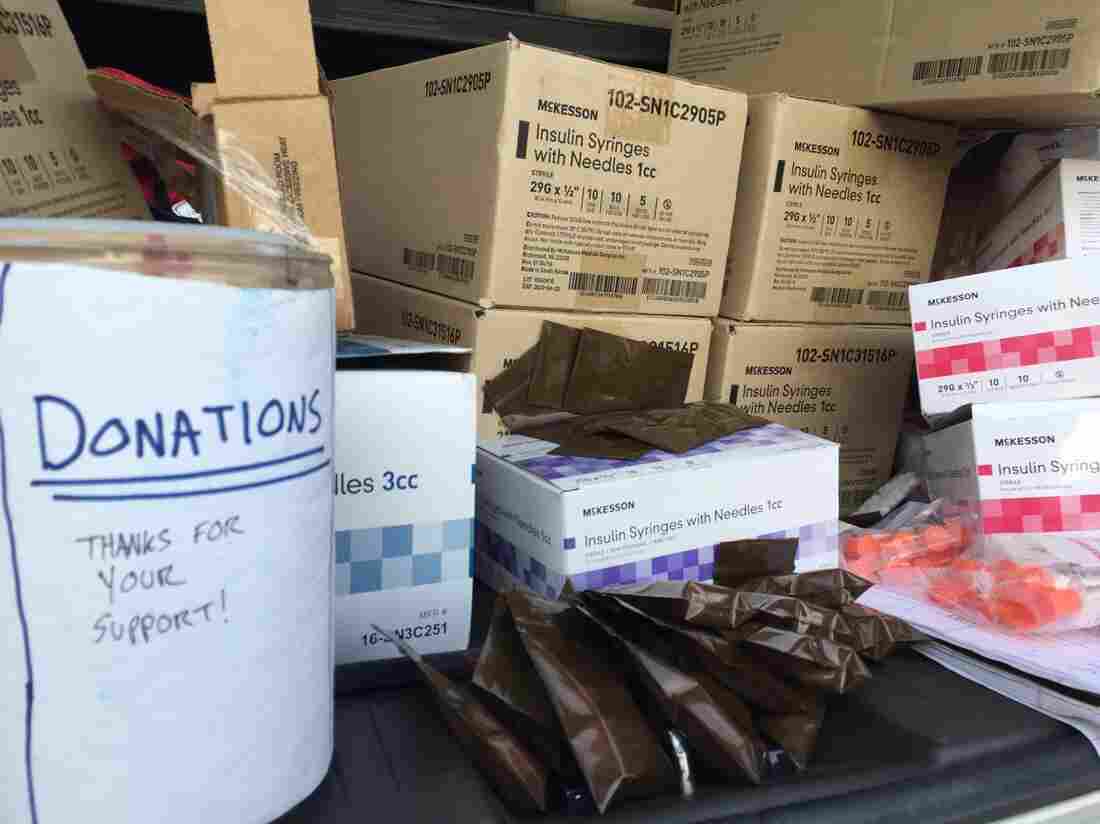
What Hospitals Waste: The nation’s health care tab is sky-high. We’re tracking down the reasons. First stop: A look at all the perfectly good stuff hospitals throw away.
What ProPublica found: Hospitals routinely toss out brand-new supplies and gently used equipment. Most of it goes to the dump, but some gets picked up by nonprofit organizations that ship the goods to the developing world.
How much money is wasted: No one tracks the total, but one charity in Maine had about $20 million worth of discarded goods filling its warehouses. Similar nonprofits operate around the country. The University of California, San Francisco Medical Center studied how much it wasted during neurosurgery operations in one year. The discarded supplies were worth $2.9 million.
How to stop the squandering: UCSF reduced waste by reviewing the lists of supplies each surgeon wanted prepped for an operation. Many items could be taken off the lists. That reduced the number of supplies opened to set up each procedure, said Dr. R. Adams Dudley, director of the UCSF Center for Healthcare Value.
Hospitals could reduce wasted supplies by tracking everything thrown away, said Dr. Robert Pearl, former CEO of The Permanente Medical Group, the country’s largest medical group and author of the book Mistreated. The amount of waste could be reported when each patient is discharged, he said. Seeing the waste quantified would motivate people to prevent it, he said.
Several experts said paying hospitals a lump sum for everything involved in a particular procedure , instead of a la carte for each item, would mean they make more profit by cutting the amount of wasted supplies and equipment.
America’s Other Drug Problem: Every year nursing homes nationwide flush, burn or throw out tons of valuable prescription drugs. Iowa collects them and gives them to needy patients for free. Most other states don’t.
What ProPublica found: Nursing home patients typically have their drugs dispensed a month at a time. So whenever a drug gets discontinued – if a patient dies, or moves out, or has a reaction – there’s excess. Most nursing homes throw away the leftover drugs. They flush them down the toilet, put them in the trash or pay to have them incinerated. Iowa started a nonprofit organization to recover the excess drugs, inspect them and dispense them for free to patients.
How much money is wasted: It’s estimated that hundreds of millions of dollars a year are wasted by throwing out nursing home medications. The CEO of a long-term care pharmacy in Florida said his company incinerates about $2.5 million in valuable medication every year. He estimated the total is $50 million statewide. Colorado officials said the state’s long-term care facilities toss out 17.5 tons of potentially reusable drugs each year, worth about $10 million. Iowa is on pace to recover $6 million in drugs from nursing homes this year.
Other harm to the public: Flushing drugs down the toilet contaminates the water supply. Trace levels of pharmaceuticals have been detected in water throughout the country.
How to stop the squandering: Many states have laws that allow drug donation, but they have not invested in a program to help the process. ProPublica’s story prompted lawmakers in Florida and New Hampshire to introduce legislation to create a program like Iowa’s. Leaders in the Vermont medical community have also shown interest in starting a drug donation program.
How Two Common Medications Became One $455 Million Specialty Pill: After I was prescribed a brand-name drug I didn’t need and given a coupon to cover the out-of-pocket costs, I discovered another reason Americans pay too much for health care.
What ProPublica found: A drug company combined two over-the-counter drugs, naproxen, which goes by the brand name Aleve, and esomeprazole magnesium, also known as Nexium, to create a new pill called Vimovo. My doctor prescribed it to me. The company that makes it, Horizon Pharma, marketed the single pill as an innovation because it was easier to take one pill than two. A month’s supply of the two inexpensive drugs costs about $40. The company billed insurance $3,252 for the Vimovo.
How much money is wasted: My insurance company rejected the bill, but Vimovo has net sales of more than $455 million since 2014. Horizon brought in $465 million more in net sales from a similar drug, Duexis, which combines ibuprofen and famotidine, aka Advil and Pepcid.
How to stop the squandering: Spurred by ProPublica’s story, Connecticut now requires doctors to get prior authorization to prescribe Horizon’s drugs to the 200,000 public employees, retirees and their dependents covered by a state insurance plan. The Connecticut comptroller also urged the attorney general’s office to investigate Horizon’s relationship with pharmacies and physicians. Other insurers have removed the drugs from their formularies.
Welch, the Dartmouth doctor, suggested tongue-in-cheek “warning labels” on drugs that aren’t actually big innovations. In the case of Vimovo, the warning could say that the “specialty” pill is actually just a combination of two cheaper ingredients. “There may need to be public service advertisements that counter the advertising that says everything is the best thing since sliced bread,” he said.
In cases where there are dramatic price increases, state lawmakers could require pharmaceutical companies to justify the higher costs, said Dr. Steven Pearson, president of the Institute for Clinical and Economic Review.
Secret deals and rebates currently cloak the actual price of drugs. Drug companies should have to publish the real prices of their products, said Linda Cahn, an attorney who advises corporations, unions and other payers on how to reduce their costs. Cahn recently proposed in an op-ed in The Hill what she calls a “bid day,” where any drug company that wants to sell its products to Medicare beneficiaries would be required to submit the net cost of each medication. All the companies would be required to submit their price at the same time, say twice a year, and then stick with the price, which Medicare would make public for all to see. The bidding would inform consumers and force competition, she said. The same process could be used for all insurance plans, she said.
The Myth of Drug Expiration Dates: Hospitals and pharmacies are required to toss expired drugs, no matter how expensive or vital. Meanwhile the FDA has long known that many remain safe and potent for years longer.
What ProPublica found: The term “expiration date” is a misnomer. The dates on drug labels are the point up to which pharmaceutical companies guarantee their effectiveness. But that does not mean the drugs are ineffective or dangerous the moment after they “expire.” The Food and Drug Administration and Defense Department created the Shelf Life Extension Program to test the stability of drugs in the federal government’s stockpiles and then extend their expiration dates, when possible. A 2006 study of 122 drugs tested by the program showed that two-thirds of them were stable every time a lot was tested. Each of them had their expiration dates extended, on average, by more than four years. But the same type of drugs in hospitals or pharmacies get thrown away when they “expire.”
How much money is wasted: The total is unknown, but one mid-size hospital in Boston had to destroy about $200,000 in expired drugs in 2016. If hospitals nationwide throw out similar amounts of drugs annually, the total would be about $800 million trashed each year by hospital pharmacies alone.
Other harm to the public: Some expired drugs are in short supply and difficult to replace. On occasion, a pharmaceutical company will extend the expiration date of drugs for which there are shortages, but they are not required to do so.
How to stop the squandering: Drug companies could be required to do studies to determine how long their products actually last, and report the information, said Lee Cantrell, a pharmacist who helps run the California Poison Control System. Also, the government could publish data from the Shelf Life Extension Program, which is funded by taxpayers. The information would help people see “many types of medications are safe and effective much longer than their original expiration dates,” Cantrell said.
Drug Companies Make Eyedrops Too Big – And You Pay for the Waste: The makers of cancer drugs also make vials with too much medication for many patients. The excess drugs are tossed in the trash — another reason health care costs are so high.
What ProPublica found: Drug companies make eyedrops much larger than what the eye can hold. That means patients pay for the excess from each drop, which runs down their cheeks. Vials of cancer drugs are also larger than necessary. The leftover cancer medication is billed to the patient – and thrown in the trash can.
How much money is wasted: It’s unknown how much it costs to waste a portion of each eyedrop, but the industry is huge. Last year, drug companies brought in about $3.4 billion in the U.S. alone for dry eyes and glaucoma drops, according to the research firm Market Scope. A 2016 study estimated that, of the top 20 cancer drugs packaged in single-use vials, 10 percent of the medication is wasted, at a cost of $1.8 billion a year.
How to stop the squandering: Citing ProPublica’s story, two U.S. senators introduced legislation that would require federal agencies to stop the waste associated with eyedrops and single-use cancer drug vials. Drugmakers could reduce the waste of cancer medication by making vials in varying sizes, so that less would be left over from each patient, said Dr. Peter Bach, director of the Center for Health Policy and Outcomes at Memorial Sloan Kettering Cancer Center in New York. Bach led a team that estimated the waste associated with vials of cancer drugs.
A Hospital Charged $1,877 to Pierce a 5-year-old’s Ears. This is Why Health Care Costs So Much: An epidemic of unnecessary treatment is wasting billions of health care dollars a year. Patients and taxpayers are paying for it.
What ProPublica found: It’s common for medical providers to deliver care that’s not needed, or that costs more than necessary, and patients get stuck with the bills. In one case, a Colorado mom said her surgeon offered to pierce her daughter’s ears as an add-on to a different operation. The mom agreed, assuming it would be free. But the hospital stuck her with a bill for $1,877 for “operating room services.” ProPublica also highlighted unnecessary imaging tests, like extra mammograms and ultrasounds, and found it’s common for hospital intensive care to be delivered to patients who are too sick or too healthy to benefit.
“We really don’t have good standards and a good discussion going on about who should receive ICU care,” said Dr. Dong Chang at the Harbor-UCLA Medical Center campus in Torrance, Calif.
Jenna Schoenefeld for ProPublica
hide caption
toggle caption
Jenna Schoenefeld for ProPublica
How much money is wasted: Unnecessary or needlessly expensive care wastes about $210 billion a year, according to the National Academy of Medicine. The cost of false-positive tests and overdiagnosed breast cancer is $4 billion a year, according to a 2015 Health Affairs study. Unnecessary intensive care costs about $137 million a year for about 100 hospitals in two states, one study estimated. That would put the tab of non-beneficial intensive care in the billions nationwide.
How to stop the squandering: Medicare has a fee schedule that sets prices and makes them public, said Welch, the Dartmouth physician who advocates against overtreatment. States could pass laws that establish similar fee schedules, he said, or insurance companies could implement them. Establishing set prices would reduce administrative overhead, he said, and allow patients to shop for the best deals.
Several experts said policymakers need to move medical providers from payment based on volume of services to payment based on value. Right now “fee for service” payment is common, so providers get a fee for everything they do. This gives them the incentive to do more, sometimes more than is necessary, or to provide care that’s more expensive than it has to be. If providers were paid a lump sum to care for individuals or a group of patients, and the outcomes of their performance were measured to ensure quality didn’t suffer, they would cut the waste. “You want to empower organizations to be responsible for improving patient health and reducing costs,” said Dr. Elliott Fisher, director of The Dartmouth Institute for Health Policy and Clinical Practice.
ProPublica is a nonprofit newsroom based in New York. You can follow Marshall Allen on Twitter:@marshall_allen. Have you seen examples of wasted health care spending? Share them with Marshall here.
What Happens To Obamacare If Individual Mandate Disappears?

Republicans’ tax overhaul gets rid of the tax penalty for people who fail to maintain insurance coverage. If it becomes law, what happens to the deficit and the number of uninsured?
GOP Tax Bill Leaves Health Savings Accounts Untouched

Some Republicans see HSAs as a great way of helping consumers deal with mounting medical costs. It’s still possible a change to the rules governing who can have an HSA and what they are allowed to cover could be added to another bill, some analysts say.
Gary Waters/Ikon Images/Getty Images
hide caption
toggle caption
Gary Waters/Ikon Images/Getty Images
The ongoing uncertainty about congressional changes to the health law — and their impact on insurance and the online marketplaces — continues to raise questions among consumers. Here are answers to recent queries.
Does the GOP tax bill affect health savings accounts?
At this time, there are no changes aimed specifically at HSAs. These are savings accounts linked to high-deductible health plans, and are exempt from tax liability.
Congressional Republicans have been very interested in expanding the use of these tax-free accounts; bills to repeal and replace the Affordable Care Act last summer included provisions to increase the maximum amount people could contribute to them or to allow people to use them to pay their health insurance premiums, among other things. The GOP promotes the plans as a way to help consumers play a larger role in controlling their health spending, and says that the tax advantages help people afford care.
But the GOP tax legislation doesn’t incorporate any of those changes, says Roy Ramthun, president of HSA Consulting Services.
Some analysts say it’s still possible that HSA changes could be attached to other pieces of legislation, such as a spending bill or a bill to extend the Children’s Health Insurance Program.
“The GOP would like to get some of these HSA expansion provisions into one of these bills,” says Dorian Smith, a partner at human resources consultant Mercer.
Republicans are seeking to repeal the individual mandate as part of the tax bill. Would that go into effect next year?
Probably not. The joint bill that House and Senate negotiators have agreed to wouldn’t repeal the individual mandate – the ACA’s requirement of most people to have health insurance. What it would repeal is the penalty for not having coverage. And that change wouldn’t take effect until 2019.
So, assuming the bill is enacted, most people will face a penalty if they don’t have health insurance in 2018. The penalty will be $695 per adult, or 2.5 percent of household income — whichever figure is greater.
Many people, however, qualify for one of several exemptions to the mandate. Those include people who have suffered a hardship like eviction or bankruptcy, and those whose earnings are low enough that health insurance is considered unaffordable.
In 2017, health insurance is considered unaffordable if the cheapest comprehensive coverage you can find would cost more than 8.16 percent of your household income.
“Because premiums have gone up so high in 2017 and 2018, there will be more people who qualify for the affordability exemption,” says Timothy Jost, an professor emeritus of law at Washington and Lee University in Virginia who is an expert on health law.
If you’re pondering whether to “go bare” next year, it’s worth noting that the Internal Revenue Service won’t accept electronically filed returns unless you indicate whether you had coverage, had an exemption or will pay the penalty
None of the marketplace plans in my area offer out-of-state coverage or any coverage for non-network providers. Why would an insurer limit what’s offered in that way?
Health plans with broad provider networks have been steadily shrinking. Nearly three-quarters of plans sold on the ACA’s marketplaces in 2018 have restrictive networks, according to an analysis by the consulting firm Avalere Health. The percentage of such plans has steadily increased since 2015, when it was 54 percent, the analysis found.
Health maintenance organization plans and exclusive provider organization plans were categorized as restrictive because they typically have relatively fewer providers and don’t provide coverage for out-of-network care. Preferred provider organization and point-of-service plans, on the other hand, were considered less restrictive because they generally have broader networks of providers and offer some out-of-network coverage.
The reason plans with restrictive networks are proliferating is because they help reduce costs, says Chris Sloan, a senior manager at Avalere.
“One of the ways to do that is to have a narrower network,” he says.
But there may be an upside for consumers. “It’s not just reducing costs for the sake of costs, it’s also to slow the premium growth,” he says.
Kaiser Health News is a nonprofit news service. It is an editorially independent program of the Kaiser Family Foundation, and is not affiliated with Kaiser Permanente. Michelle Andrews is on Twitter @mandrews110.
Fight The Opioid Epidemic, All Agree. But Strategies Vary Widely
The rising number of opioid-linked deaths led Arizona to declare a public health emergency in 2017. Needle exchange programs are not explicitly permitted in Arizona, but one such service operates underground, giving out clean needles and naloxone, a medicine widely used to counter effects of an opioid overdose.
Will Stone / KJZZ
hide caption
toggle caption
Will Stone / KJZZ
It’s no secret why drug users come to George Patterson in a mall parking lot just outside Phoenix to get their clean needles, syringes and other supplies on Tuesday afternoons, instead of heading to the pharmacy down the street.
“It’s really low-barrier the way we are doing it,” Patterson says. “All you have to do is find us.”
Patterson asks for no IDs, no signatures and no questions — all of which can dissuade IV drug users from seeking out clean needles or the overdose reversal drug naloxone, Patterson says. He’s among the volunteers who run Central Arizona’s only syringe exchange program; it’s called Shot in the Dark.
“A lot of [the drug users he sees] have trust issues — understandably — with the health care industry, with what’s going to be put on their record,” Patterson says, as he hands out the medical supplies from the trunk of his car.

George Patterson is one of the volunteers who run Phoenix’s only syringe exchange program, a mobile program called Shot in the Dark.
Will Stone / KJZZ
hide caption
toggle caption
Will Stone / KJZZ
While many states have syringe exchanges, only some have laws that explicitly permit syringe exchanges — and Arizona isn’t one of them. Shot in the Dark operates quietly, without public funding. The group sets up in different corners of the Phoenix metro area for a few hours at a time, Patterson says, and struggles to keep up with demand.
“There are still a lot of people that don’t know even know about it,” says one man who uses the service. “It shouldn’t be so hidden.” NPR agreed not to use his name because his drug use is illegal.
States across the U.S. are pouring resources into fighting the opioid epidemic. According to state data from 2016, two people died every day in Arizona from opioid-related overdoses. Deaths due to heroin tripled between 2012 and 2016.
“It’s a problem that knows no bounds,” Arizona’s Republican governor, Doug Ducey, said in January during his State of the State address. “It affects men and women, young and old, rich and poor.”
Ducey has declared the opioid epidemic a public health emergency — a move that a handful of other states have made, too. In Arizona, the designation allowed public health officials to begin tracking overdose data in real time and set in motion a multi-agency effort to combat the epidemic.
But some public health advocates, including Patterson, feel the governor’s declaration hasn’t necessarily translated into more help for people on the street using drugs.
“Instead of focusing on ways that you can connect with the IV-drug using population — show them that their health matters, and prevent all the people who are likely never going to stop using IV drugs,” Patterson says, “they, like, leave them out here to pick up dirty needles out of parks and give themselves diseases.”
Needle exchanges are based on a concept known as harm reduction — they seek to reduce the negative consequences of drug use without forcing abstinence. The U.S. Surgeon General has determined such programs don’t promote drug use and do improve health outcomes, including lower HIV rates.
But that hasn’t convinced some of Arizona’s most influential law enforcement figures.
“It’s a well-intentioned, misguided program,” Maricopa County Attorney Bill Montgomery says. “We don’t have a free-case-of-beer-a-month program for alcoholics,” he points out. “It sends the wrong message — and it’s not providing the treatment.”
This is a common argument against syringe exchange programs — that they enable drug use. Proponents of harm reduction, however, point to research showing that people who use these programs are actually more likely than others to seek treatment.
Despite his lack of faith in needle exchange programs, Montgomery says he is sympathetic to people who are addicted to opioids — he is not out to prosecute drug users when he doesn’t have to.
“Law enforcement really does look at ‘treatment first’ as an option for those who are addicted,” Montgomery says. He points to a pretrial diversion program that is expanding statewide, and the Arizona Angel Initiative, which lets drug users turn to the police and opt for treatment.
Expanding those kinds of programs is part of the state’s wide-ranging Opioid Action Plan, which treatment specialists helped craft.
The 100-page policy roadmap recommends improving access to treatment and naloxone, as well as enacting a Good Samaritan law that gives immunity to those who call 911 to report an overdose.
But the plan also proposes more regulation of doctors and their prescribing practices, including a 5-day limit on initial opioid prescriptions for patients who are taking the drug for the first time.
That kind of focus on prescribers is “misguided” says Dr. Jeffrey Singer, an Arizona surgeon, and senior fellow at the libertarian Cato Institute.
“Our policies right now are aimed at the supply side,” Singer says. “And all they are doing is driving the death rate up. They’re not driving use down.”
Opioid users are increasingly turning to heroin and fentanyl, Singer says. He points to research that shows the rate of opioid prescriptions has fallen in recent years while the deaths associated with illicit drugs continue to rise.
Singer believes even labeling the state’s opioid crisis as a public health emergency could backfire.
“That tends to create a sense of panic,” Singer says. “History has shown us every time we have a panic we end up passing laws and doing things in haste that are not well thought out.”
Singer thinks Arizona should embrace harm reduction strategies like syringe exchanges, instead of tamping down prescribing.
“My job is to save lives and to ease suffering,” Singer says. “The law enforcement people need to have that same attitude. We’ve got to take out personal biases out of it and just focus on the goal, which is less death and less disease.”
Earlier this year, the Arizona Department of Health Services asked a group of treatment providers who were working on the state’s action plan for their top recommendations. Legalizing syringe exchanges was one of the group’s priorities, according to interviews and draft documents obtained by KJZZ News.
But that priority didn’t make the final version of the plan; only a broad reference to using “harm reduction strategies” survived.
A spokesperson for the department says the recommendation was omitted because it “doesn’t directly reduce opioid-related overdoses or deaths.”
This story is part of a reporting partnership with NPR, KJZZ and Kaiser Health News. You can find Will Stone on Twitter at @WStoneReports.
Food And Drug Administration Plans Crackdown On Risky Homeopathic Remedies

The Food and Drug Administration plans to take action against risky homeopathic remedies under a policy unveiled Monday.
Alexander Baumann/EyeEm/Getty Images
hide caption
toggle caption
Alexander Baumann/EyeEm/Getty Images
Updated at 4:17 p.m. ET to include comment from homeopathic pharmacists.
The Food and Drug Administration said it plans to crack down on the sale of some homeopathic products.
The agency unveiled a new, risk-based approach to regulating homeopathic treatments Monday that aims to protect the public from dangerous products.
“In recent years, we’ve seen a large uptick in products labeled as homeopathic that are being marketed for a wide array of diseases and conditions, from the common cold to cancer,” FDA Commissioner Scott Gottlieb said in a statement announcing the new policy.
“In many cases, people may be placing their trust and money in therapies that may bring little to no benefit in combating serious ailments, or worse — that may cause significant and even irreparable harm because the products are poorly manufactured, or contain active ingredients that aren’t adequately tested or disclosed to patients,” Gottlieb says.
Homeopathy is an ancient practice based on the idea that small traces of substances that cause diseases can actually be used to treat illness. But critics have long charged that there is no scientific evidence to support homeopathy and that some homeopathic products could be dangerous.
Critics have been especially concerned about products being contaminated with dangerous substances, or sold for serious conditions for which other, proven treatments work.
The FDA has issued warnings about specific products in the past, and the Federal Trade Commission has required better labeling of homeopathic products.
But over the past decade, the homeopathic drug market has grown “exponentially,” according to the FDA, becoming a nearly $3 billion industry in the United States.
The FDA has seen a “corresponding increase in safety concerns, including serious adverse events” resulting from homeopathic products, the FDA says.
In response to the growth and continuing concerns, the FDA convened a public hearing to revisit a 1988 decision not to regulate homeopathic products like standard medical treatments.
Under the new policy, the FDA will more carefully scrutinize these products, especially those sold to treat infants and children, those containing ingredients with significant safety concerns, such as belladonna, and those sold for serious conditions such as opioid addiction, heart disease and cancer.
“We respect that some individuals want to use alternative treatments, but the FDA has a responsibility to protect the public from products that may not deliver any benefit and have the potential to cause harm,” Gottlieb says.
Mark Land, president of the American Association of Homeopathic Pharmacists, said in an email that the group “shares the FDA’s commitment to protecting public health,” and noted the action “would not materially affect the vast majority of homeopathic drug products available in the United States.”
“As always, AAHP is committed to ensuring that consumers have access to natural, safe, homeopathic medicines in the United States and throughout the world,” Land said.
During a briefing for reporters about the proposed new policy, FDA officials stressed that the agency had no intention of requiring most homeopathic products that are on the market to undergo formal FDA review, however, or to remove most homeopathic products. So people who believe such products help them will still have access to many of them, the officials said.
The proposed policy will be open for public comment for 90 days. The agency will review the comments before making the policy final.
The agency’s move was praised by long-term critics of the industry.
“I think that it’s about time that these snake oil salesmen were held accountable for what they’re selling,” says Paul Offit, a pediatrician at the Children’s Hospital of Philadelphia. “The consumer will clearly benefit.”
In Election Year, Drug Industry Spent Big To Temper Talk About High Drug Prices

With drug prices in the election spotlight, the pharmaceutical industry’s main trade group raised its revenue and spending.
PeopleImages/Getty Images
hide caption
toggle caption
PeopleImages/Getty Images
Facing bipartisan hostility over high drug prices in an election year, the pharmaceutical industry’s biggest trade group boosted revenue by nearly a fourth in 2016 and spread the millions collected among hundreds of lobbyists, politicians and patient groups, new filings show.
It was the biggest surge for the Pharmaceutical Research and Manufacturers of America, known as PhRMA, since the group took battle stations to advance its interests in 2009 during the run-up to the Affordable Care Act.
“Does that surprise you?” said Billy Tauzin, the former PhRMA CEO who ran the organization a decade ago as Obamacare loomed. Whenever Washington seems interested in limiting drug prices, he said, “PhRMA has always responded by increasing its resources.”
The group, already one of the most powerful trade organizations in any industry, collected $271 million in member dues and other income in 2016. That was up from $220 million the year before, according to its latest disclosure with the Internal Revenue Service.
PhRMA spent $7 million last year to prepare its ubiquitous “Go Boldly” ad campaign and gave millions to politicians who were up for election in both parties in dozens of states. It lavished more than $2 million on scores of groups representing patients with various diseases — many of them dealing with high drug costs. PhRMA has also provided financial support to NPR.
Some of the biggest patient-group checks went to the American Autoimmune Related Disease Association, for $260,000; the American Lung Association, for $110,000; the Juvenile Diabetes Research Foundation, for $136,150; and the Lupus Foundation of America, for $253,500.
PhRMA also gave big money to national political groups financing congressional, presidential and state candidates. The conservative-leaning American Action Network got $6.1 million. The Republican Governors Association got $301,375. Its Democratic counterpart got $350,000.
PhRMA’s state and federal lobbying spending rose by more than two-thirds from the previous year, to $57 million.
“That’s PhRMA. They do it all” to protect drug companies from potential policy risks, said Sheila Krumholz, executive director of the Center for Responsive Politics, which tracks political financing. “And they’re going to marshal even more resources when they perceive that these threats or opportunities are most imminent.”
The association’s 37 members include the biggest and best-known drug companies including Johnson & Johnson, Celgene, Merck, Pfizer, Eli Lilly and Amgen. Holly Campbell, a PhRMA spokeswoman, declined to make an executive available to discuss the IRS report, saying it doesn’t comment on contributions.
“PhRMA engages with stakeholders across the health care system to hear their perspectives and priorities,” she said in an email. “We work with many organizations with which we have both agreements and disagreements on public policy issues.”
Nonprofit organizations such as PhRMA must file detailed disclosures with the IRS. PhRMA, which submitted its 2016 report in early November, shared a copy with Kaiser Health News.
Threats to PhRMA members seemed especially dire in 2016. Storms of bad publicity hit the industry in the form of stories about arrogant executives and thousand-dollar pills.
Democratic presidential candidate Hillary Clinton said some pharma companies were “making a fortune off of people’s misfortune.” Then-candidate Donald Trump, a Republican, suggested he could save $300 billion annually by requiring drugmakers to bid on business.
The group also aimed money at states where policymakers were considering drug-related measures such as price limits or greater price transparency, the document shows.
It gave $64 million to a California fund established to defeat a proposal requiring state agencies to pay no more for drugs than does the federal Department of Veterans Affairs. Also supported by direct contributions from drug companies, the fund spent $110 million last year to defeat the initiative, California regulatory filings show.
This year, California established a less comprehensive law requiring drug firms to give notice and explanation when they substantially raise prices. PhRMA recently sued to block that measure.
In Louisiana, where policymakers were considering proposals to make drug prices clearer to consumers, PhRMA gave campaign contributions directly to scores of state legislators last year. The group also gave hundreds of thousands of dollars to help defeat a ballot proposal for single-payer health care in Colorado.
Last year’s massive mobilization underscores how besieged the industry felt over complaints about soaring medicine prices and high profits.
PhRMA’s $271 million in revenue for the year represented its biggest budget since 2009, when it recorded $350 million in dues and other revenue.
The $57 million it spent on lobbying was also the most since 2009, when the lobbying bill was $70 million. So was the $7 million spent on advertising, a cost that should rise this year, since the “Go Boldly” ads aired in 2017. PhRMA employed 237 people last year, up from fewer than 200 in 2011.
Patient groups receiving PhRMA money often deny that it influences their policies or keeps them from criticizing high drug prices.
The Lupus Foundation has policies to ensure there is no conflict of interest, a spokeswoman said. At the Juvenile Diabetes Research Foundation, donors such as PhRMA “have no role” in the group’s decision-making process, a spokeswoman said.
“No funder influences our position, agenda or science-based messages” at the American Lung Association, its spokeswoman said.
The American Autoimmune Related Disease Association did not respond to requests for comment.
During negotiations over Obamacare, PhRMA agreed to support overhauling health care relatively early in the process, in mid-2009. Then it threw its muscle into promoting the measure, which promised billions in new revenue for members. President Obama signed it into law in March 2010.
PhRMA shrank substantially after that, taking in around $205 million for several years in a row starting in 2010.
Last year it agreed to increase dues by 50 percent to raise an extra $100 million, Politico reported. In an attempt to distance itself from drug companies earning bad headlines, it also decided to bar members that don’t invest a minimum in pharmaceutical research.
Kaiser Health News (KHN) is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente. You can follow Jay Hancock on Twitter: @jayhancock1
Older Adults' Forgetfulness Tied To Faulty Brain Rhythms In Sleep
As people age they may forget more because their brain waves get out of sync, new research finds.
PhotoAlto/Frederic Cirou/Getty Images
hide caption
toggle caption
PhotoAlto/Frederic Cirou/Getty Images
Older brains may forget more because they lose their rhythm at night.
During deep sleep, older people have less coordination between two brain waves that are important to saving new memories, a team reports in the journal Neuron.
“It’s like a drummer that’s perhaps just one beat off the rhythm,” says Matt Walker, one of the paper’s authors and a professor of neuroscience and psychology at the University of California, Berkeley. “The aging brain just doesn’t seem to be able to synchronize its brain waves effectively.”
The finding appears to answer a long-standing question about how aging can affect memory even in people who do not have Alzheimer’s or some other brain disease.
“This is the first paper that actually found a cellular mechanism that might be affected during aging and therefore be responsible for a lack of memory consolidation during sleep,” says Julie Seibt, a lecturer in sleep and plasticity at the University of Surrey in the U.K. Seibt was not involved in the new study.
To confirm the finding, though, researchers will have to show that it’s possible to cause memory problems in a young brain by disrupting these rhythms, Seibt says.
The study was the result of an effort to understand how the sleeping brain turns short-term memories into memories that can last a lifetime, says Walker, the author of the book Why We Sleep. “What is it about sleep that seems to perform this elegant trick of cementing new facts into the neural architecture of the brain?”
To find out, Walker and a team of scientists had 20 young adults learn 120 pairs of words. “Then we put electrodes on their head and we had them sleep,” he says.
The electrodes let researchers monitor the electrical waves produced by the brain during deep sleep. They focused on the interaction between slow waves, which occur every second or so, and faster waves called sleep spindles, which occur more than 12 times a second.
The next morning the volunteers took a test to see how many word pairs they could still remember. And it turned out their performance was determined by how well their slow waves and spindles had synchronized during deep sleep.
“When those two brain waves were perfectly coinciding, that’s when you seem to get this fantastic transfer of memory within the brain from short term vulnerable storage sites to these more permanent, safe, long-term storage sites,” Walker says.
Next, the team repeated the experiment with 32 people in their 60s and 70s. Their brain waves were less synchronized during deep sleep. They also remembered fewer word pairs the next morning.
And, just like with young people, performance on the memory test was determined by how well their brain waves kept the beat, says Randolph Helfrich, an author of the new study and a postdoctoral fellow at UC Berkeley.
“If you’re like 50 milliseconds too early, 50 milliseconds too late, then the storing mechanism actually doesn’t work.” Helfrich says.
The team also found a likely reason for the lack of coordination associated with aging: atrophy of an area of the brain involved in producing deep sleep. People with more atrophy had less rhythm in the brain, Walker says.
That’s discouraging because atrophy in this area of the brain is a normal consequence of aging, Walker says, and can be much worse in people with Alzheimer’s.
But the study also suggests that it’s possible to improve an impaired memory by re-synchronizing brain rhythms during sleep.
One way to do this would be by applying electrical or magnetic pulses through the scalp. “The idea is to boost those brain waves and bring them back together,” Helfrich says.
Walker already has plans to test this approach to synchronizing brain waves.
“What we’re going to try and do is act like a metronome and in doing so see if we can actually salvage aspects of learning and memory in older adults and those with dementia,” he says.
Weighing The Impact Of Repealing The Health Insurance Mandate
The tax bill being considered by Congress includes a repeal of the Affordable Care Act’s individual mandate. Julie Rovner of Kaiser Health News talks to guest host Ray Suarez about how that could affect the health insurance market.
RAY SUAREZ, HOST:
We’re going to continue our conversation about the Republican tax bill and focus on specific provisions in the bill affecting health care. As we just heard, the bill will repeal what’s called the individual mandate, a key part of the Affordable Care Act that requires people to buy health insurance or face a tax penalty. To understand what effect this could have on the insurance market, we’re joined now by Julie Rovner, Washington correspondent for Kaiser Health News. Good to have you with us, Julie.
JULIE ROVNER: Nice to be here.
SUAREZ: So what would be the most immediate effect of the repeal?
ROVNER: Well, the most immediate effect is that people will be confused because they’re actually repealing the penalties but not until 2019. So for next year, people will still be required to either have health insurance or pay a penalty. And, of course, yesterday was the end of open enrollment for most people in most states.
SUAREZ: Now, when people leave the insurance market, it must have some effect on the numbers that are very, very carefully balanced for this law to work.
ROVNER: That’s right. That’s the biggest concern that insurers have. Insurance – said when the Affordable Care Act was passed, that if you’re going to require us to accept sick people and not to charge them more, you’re going to have to have some way to get more healthy people into the pool. That’s what this mandate penalty was about. Insurers said at the beginning it wasn’t big enough. And, in fact, it hasn’t really driven that many healthy people to sign up. But there is a concern that if you take it away and don’t replace it with anything – and at the moment there is no replacement in this bill – that literally only sick people will buy insurance. The only response for insurers at that point is either to raise premiums dramatically or to drop out altogether.
SUAREZ: One senator for whom the repeal of the mandate had been a sticking point was Republican Susan Collins of Maine. Originally, she noted that repealing the mandate would have consequences for the future stability of the individual market. Now, she says she’ll back the tax bill if Congress acts on other health measures. What are they?
ROVNER: Well, there’s two. And one of them would restore these payments that the president cut off last fall that go to insurers to reimburse them for discounts they have to give to their lowest-income enrollees on the exchanges. They’re called cost-sharing reduction payments. But basically, the insurers have already figured out how to get that money back. They’ve raised premiums strategically, and that made premium subsidies higher. So basically, the federal government is giving them back the money in other ways. So most analysts think that it’s probably too late for that to help.
The other thing that Susan Collins asked for was a reinsurance pool. That would help insurers pay for their sickest customers. Most analysts think that would help but that the money that’s being talked about is probably not enough. Also, it’s not entirely clear that they could get this through the House even if they can get it through the Senate.
SUAREZ: The tax bill, it’s understood widely, will increase the deficit. The argument is about how much, but that means entitlement programs may be under some pressure. Do we know how the bill could affect Medicare?
ROVNER: Yes, we do. Medicare could be cut by billions of dollars. That can be waived by Congress but it takes 60 votes. The Republicans assume the Democrats will come along because they don’t want cuts to Medicare, which the Democrats don’t. But Democrats are warning that they may play hardball on this and that Republicans should not assume that they’re going to vote to waive these cuts which are automatic if the deficit is raised to the extent it would be by this tax bill.
SUAREZ: Julie Rovner is Washington correspondent for Kaiser Health News. Julie, thanks for joining us.
ROVNER: You’re most welcome.
Copyright © 2017 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Trump Administration Reportedly Instructs CDC On Its Own Version Of 7 Dirty Words

A report from The Washington Post said the health agency was issued a list of prohibited words from the Trump administration.
Kevin C. Cox/Getty Images
hide caption
toggle caption
Kevin C. Cox/Getty Images
Updated at 3:34 p.m. ET
Trump Administration officials at the Department of Health and Human Services are pushing back on a report saying the Centers for Disease Control and Prevention issued a mandate to no longer use words and phrases including “fetus,” “transgender” and “science-based.”
According to The Washington Post, the directive was delivered to senior CDC officials responsible for overseeing the health agency’s budget. The Post broke news of this Friday evening.
By Saturday afternoon, HHS, which includes the CDC, issued a statement, calling the existence of a set of banned words a “complete mischaracterization.” Spokesperson Matt Lloyd adds:
“The assertion that HHS has ‘banned words’ is a complete mischaracterization of discussions regarding the budget formulation process. HHS will continue to use the best scientific evidence available to improve the health of all Americans. HHS also strongly encourages the use of outcome and evidence data in program evaluations and budget decisions.”
The seven words that were to be stricken from official documents being drafted for the 2019 fiscal year budget, according to the Post, are:
- diversity
- entitlement
- evidence-based
- fetus
- science-based
- transgender
- vulnerable
According to an unnamed CDC analyst in the Post’s write-up, the list of the prohibited words was unveiled at the agency’s headquarters in Atlanta during a Thursday meeting that lasted 90 minutes. The meeting was reportedly led by Alison Kelly, a top official with CDC’s Office of Financial Services. The Post adds that Kelly did not give a reason why the words were being banned, only that she was simply relaying the information. The Post adds:
“In some instances, the analysts were given alternative phrases. Instead of ‘science-based’ or ’evidence-based,’ the suggested phrase is, ‘CDC bases its recommendations on science in consideration with community standards and wishes,’ the person said. In other cases, no replacement words were immediately offered.”
If the report is true, it raises concerns about censorship under the Trump administration. As NPR’s Rebecca Hersher reported last month, an NPR analysis found a decline in the number of grants awarded by the National Science Foundation with the phrase “climate change” either in the title or the summary.
Hersher also reported:
“The change in language appears to be driven in part by the Trump administration’s open hostility to the topic of climate change. Earlier this year, President Trump pulled the U.S. out of the Paris climate accord, and the president’s 2018 budget proposal singled out climate change research programs for elimination.”
According to the Union of Concerned Scientists, it is not uncommon for career staff at government agencies to self-censor in order to avoid being a political target.
“It is unclear whether the directive came from Trump administration officials or from career staff self-censoring to avoid falling into political traps. Career staff at government agencies often modify language to stop their work from being politicized.
“Yet there’s a fine line between necessary self-preservation and needless self-censorship.”
Reverberations Of War Complicate Vietnam Veterans' End-Of-Life Care

Ron Fleming, who served as a door gunneron helicopters in the Vietnam War, was admitted to the veterans hospital in San Francisco recently because of an asthma attack. Fleming has PTSD, but told his doctors he doesn’t want to take medicine for it. He’s concerned the pills might dull the emotional connection he feels to his wartime past.
April Dembosky / KQED
hide caption
toggle caption
April Dembosky / KQED
Ron Fleming is 74 now, but he’s spent most of his life trying to recapture what life felt like when he was 21, fighting in Vietnam.
Fleming was a door gunner in the war, hanging out of a helicopter on a strap with a machine gun in his hands. He fought in the Tet Offensive of 1968, sometimes for 40 hours straight, firing 6,000 rounds a minute. But he never gave much thought to catching a bullet himself.
“At 21, you’re bulletproof,” he says, as he sits on the edge of his hospital bed at the San Francisco VA Medical Center. “Dying wasn’t on the agenda.”
Now it is. Fleming has congestive heart failure and arthritis, and his asthma attacks often land him in the hospital. Ten years ago, he was diagnosed with post-traumatic stress disorder, which makes him quick to anger and hyper-vigilant, as though he’s still in that helicopter.
Fleming’s physical and mental health symptoms, combined with his military history, are a challenge to the VA’s palliative care team, which is coordinating his care as his health deteriorates. It is a challenge they are facing more often as Vietnam veterans age and develop life-threatening illnesses.
For some veterans, the stoicism they relied on in battle returns full-force in the hospital; they’re less willing than other patients to admit they are afraid or in pain, and less willing to accept treatment. Other vets with PTSD are even more reluctant to take pain-relieving opioids because the drugs can actually make their symptoms worse, triggering frightening flashbacks.
About 30 percent of Vietnam vets have had PTSD in their lifetime, the highest rate among veteran groups from all eras, according to the U.S. Department of Veterans Affairs’ National Center for PTSD. Their rate is higher, according to numerous studies, because of the unique combat conditions they faced and the negative reception many received when they returned home.
Since the war, many vets have developed coping strategies to keep disturbing memories and other PTSD symptoms at bay. But facing a terminal illness — the severe pain of cancer, the nausea of chemotherapy or the breathlessness of heart failure — can drain their energy so much that they’re unable to maintain their mental defenses. Vets previously diagnosed with PTSD can slip out of remission, and some may experience the condition for the first time.
“They’re so distracted trying to cope with their physical symptoms that they might have flashbacks,” says Dr. VJ Periyakoil, a palliative care physician at the VA Palo Alto Health Care Center and director of palliative care education at Stanford University. “War memories start coming back; they start having nightmares.”
Gasping for breath can induce panic for anyone, but it can make vets feel as threatened as they did in a combat zone, says Dr. Eric Widera, director of hospice and palliative care at the San Francisco VA and professor of geriatrics at the University of California, San Francisco.
Earl Borges, now 70, conducted river patrols in the Navy during the Vietnam War. These days, he says, symptoms from chronic obstructive pulmonary disease and ALS can intensify the anxiety he experiences as a result of PTSD.
Courtesy of Shirley Borges
hide caption
toggle caption
Courtesy of Shirley Borges
That’s what happens to navy vet Earl Borges, who logged 240 24-hour river patrols in Vietnam with three other men in a plastic boat, constantly watching the riverside brush for enemy soldiers.
Ever since, he’s been easily startled by loud noises and fast-moving shadows. Now, at age 70, Borges has Lou Gehrig’s disease – the progressive disease of motor neurons that is also called amyotrophic lateral sclerosis, or ALS — and chronic obstructive pulmonary disease, which can intensify the anxiety from his PTSD.
If he lies down without his breathing machine, he says, he panics, then hyperventilates.
“I have to talk him through it, tell him he’s OK, ‘just breathe,’ ” says his wife, Shirley Borges, 67.
They both say Earl’s PTSD is under control — as long as he doesn’t talk about the war — and his ALS is progressing very slowly, without pain.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Earl Borges in the late ’60s in the missile launch room of the USS Stoddard. Borges served as a petty officer in the U.S. Navy during the Vietnam War.
Courtesy of Shirley Borges
hide caption
toggle caption
Courtesy of Shirley Borges
But for patients who are in severe pain, the go-to treatment is opioids, which can also make PTSD symptoms worse. This forces vets to choose between physical pain and mental anguish.
“Oftentimes, pain medications like morphine or oxycodone make some people feel a little bit fuzzy,” Widera says. “That may contribute to that feeling of a loss of control.”
That’s why Periyakoil isn’t surprised when vets refuse pain medications.
” ‘Don’t you try and give me none of those narc pills, doc,’ ” she recalls one of her patients saying while he grimaced in pain.
Some vets also refuse medication because they feel like they deserve the pain.
“We see a lot of feelings of guilt over what they’ve seen and done during their experience in Vietnam,” Widera says, “and they don’t want to blunt that.”
At the end of life, this sense of guilt can be amplified as veterans look back and review their lives and, perhaps, contemplate the consequences of their actions in the line of duty. This is even true for vets like Fleming, whose overriding feeling about his service is pride.
“Sometimes I think that now I’m being paid back for all the men I killed,” he says. “And I killed a lot of them. Fleming says he has not needed opioids for his condition, and has declined other medications.
“If there is a judge, I figure I’m going to hell in a hand-basket,” he says.
Watching vets choose to endure their pain can be hard for families, as well as for palliative care doctors and nurses. Just like soldiers, doctors hate doing nothing.
“Staff [members] suffer terribly because they feel like, ‘what good are the hospice experts if we can’t take care of patients’ pain?’ ” Periyakoil says.
Often, the only thing they can do is stand back and respect a veteran’s choice to bear their pain, she says.
Once, when Periyakoil was dressing the ulcer wounds of the patient who refused what he called “narc pills,” he began talking about the war. She didn’t press him, just kept working quietly, tending his wounds. As he stared at the ceiling, wincing, he confided in her about a time he was forced to kill a pregnant teenager.
But this kind of revelation is unusual, she says. With weeks or months left to live, after a lifetime of silence about their most horrifying memories, there often isn’t enough time for veterans to talk about those experiences at all.
That’s one reason the VA has been trying to start end-of-life care earlier, Widera says — to address veterans’ PTSD or moral distress years before they land in hospice.
Fleming’s doctors, for instance, have urged him to consider mental health counseling or antidepressants. He refuses.
“I don’t want to take psychiatric drugs,” he says. “The vets call them ‘the happy pills.’ I don’t want any of those, because they change you. I don’t want to change.”
The emotional pain connects Fleming to his past.
He was awarded 18 Air Medals for meritorious acts and heroism in flight. The loss and grief he experienced in Vietnam are woven into those memories of victory and glory.
“You see all the combat. There’s a charge to it,” he says. “And after a while, it bites you right in the ass. And once you’ve been bit, you’re bit for life. Nothing else works.”
This story is part of a partnership with NPR, KQED and Kaiser Health News.