A 1960s 'Hippie Clinic' In San Francisco Inspired A Medical Philosophy

Inside the Haight Ashbury Free Medical Clinic in its earliest days. The clinic opened on June 7, 1967, and treated 250 patients that day. It’s motto, then and now: “Health care is a right, not a privilege.”
Courtesy of Gene Anthony/David Smith Archives
hide caption
toggle caption
Courtesy of Gene Anthony/David Smith Archives
Unlike many things from the 1967 “Summer of Love,” the Haight Ashbury Free Clinic survived.
The clinic, now part of a larger network, still operates out of a second-floor office overlooking Haight Street in San Francisco. A steep wooden staircase leads to a warren of small but airy rooms.
One exam room still has a wall covered by a faded psychedelic mural, featuring a collage of famous rock stars, naked bodies and peace signs.
The decor used to be even more colorful, according to lab manager Pam Olton. She has worked at the Free Clinic for more than 40 years.
“Pink, aqua, Day-Glo orange … all of these exam rooms were painted in those Day-Glo colors,” she says.
The colors helped the young patients feel welcome, Olton explains, easing their drug-induced paranoia or just reassuring them that the clinic was a safe and sympathetic space. In the summer of 1967, and for years after, the Free Clinic treated the countercultural denizens of the Haight-Ashbury neighborhood. They were often the patients that nobody else wanted.
“You had a big flash mob of kids coming to this neighborhood from all over — from everywhere in America,” Olton says. Most had no health insurance, and some were living in parks, on the street or sharing crowded apartments.
“They’re kids, they’re dirty, they’re a mess and they’re addicted,” Olton says. “But we have to take care of their medical needs first. And we have to be nonjudgmental. They’re human beings — they’re somebody’s kid and we need to take care of them.”
Dr. David Smith was a young faculty member at the University of California, San Francisco when he started the free clinic 50 years ago. He’s now 78 and still works in addiction medicine.
“We were kind of the caregivers to the love generation,” Smith says. At the beginning of 1967, he had one foot in the world of academic medicine and one foot in the burgeoning counterculture. He lived in the Haight and had experimented with drugs.
“I had an LSD spiritual experience, and a vision that denial of health care to one segment of the population is a denial to all,” Smith recalls. “So there was a transformation of me in that period, in ’67, like what happened to so many young people. I just happened to have a medical skill when that transformation occurred.”

Dr. David Smith (second from left) helps a young woman by bandaging her feet as part of the clinic’s street medicine in 1968.
Courtesy of David Smith Archives
hide caption
toggle caption
Courtesy of David Smith Archives
‘Health care is a right, not a privilege’
Smith knew that thousands of young adults would flood into San Francisco that summer, and he was worried about who would treat them and how these young people would be treated by people in mainstream medicine.
“Some of us went to the city [health officials] and said, there’s going to be a huge problem this summer, and we need what we called then ‘a hippie clinic,’ ” Smith recalls. “And it was soundly rejected by the health department. They had no interest in this. They said, ‘We don’t want to take care of them. We want them to go away.’ “
Smith and some colleagues, along with residents of the Haight, started getting ready anyway. It was during one of their planning meetings that Smith stood up and declared: ” ‘Health care is a right, not a privilege.’
“It became the founding slogan of our Haight Ashbury Free Clinic,” he says.
The clinic opened on June 7, 1967, to a line of people stretching down the block. The team worked through the night and treated 250 people, Smith says. The next day, the staff treated 350 more.
At that time, the staff was entirely volunteer — a mix of sympathetic doctors, nurses and students from the local medical and pharmacy schools.
Keeping the clinic going was a struggle. Money for rent and supplies was in short supply. Police officers would frequently show up and search the rooms, looking for illicit drugs and underage runaways.
But Smith was determined to keep the clinic open. If hippies hurt themselves, many mainstream doctors thought they got what they deserved. Sometimes hospitals turned them away. And when they got sick from taking illegal drugs, or overdosed, or became psychotic, they were often shamed, restrained or thrown in jail. The Free Clinic offered a safe space.
“If you were taken to the Haight Ashbury Free Clinic, you would be put into a room … with a talk-down guide and a lava lamp,” he says. “You’d be examined by a physician to see if you needed medication to help you come down.”
After 1967, the clinic continued as a medical refuge and its compassionate approach endured through the harder drugs of the 1970s, and the AIDS epidemic of the 1980s.
Eric Smith (no relation to the clinic’s founder) remembers visiting the Free Clinic about 15 years ago. He was living on the streets of San Francisco and using heroin. He can’t remember why he went there for care, but he does remember what it felt like to be there.
“I went in there — there was a whole bunch of people hanging out. It was cool,” Eric says. He remembers the staff and others asking, ” ‘How can we help you out?’ “

Eric Smith, left, talks to a homeless couple in San Francisco during neighborhood rounds. He’s patient coordinator at the Haight-Ashbury Free Clinics, and wants to make sure they know they can get health care and addiction treatment there.
Carrie Feibel / KQED
hide caption
toggle caption
Carrie Feibel / KQED
“People were eating,” he recalls. “Some girl asked if I was hungry. She brought me a vegetarian burrito. It was very welcoming, and I didn’t feel nervous or ashamed being in there. You know? I felt like these are my people, they’ll help me out. I can be honest with them. I think that carries on right now.”
Meeting modern challenges
Eric Smith eventually got off drugs, and for the last two years has worked for the clinic as a patient coordinator.
When patients come to the clinic, Smith makes sure they are connected to the services they need — whether that’s medical or dental care, therapy, detox or a drug recovery program.
And he walks the neighborhoods of San Francisco, doing outreach.
He brings naloxone for opioid overdoses and a CPR mask. He has a big backpack full of snacks to hand out, along with gloves, socks, condoms and toothbrushes.
On the day I join him for his rounds, Eric stops by a row of tents on Folsom Street. Men gather around as he passes out supplies.
“You guys know who I work with, right?” he asks as he hands out socks and granola bars. “So, you guys need any services at all? Is there anything you need?”
On this particular day, none of the men are interested in visiting the clinic.
Eric just smiles and moves on. No encounter is ever wasted, he tells me.
“I have to build a trust and rapport with the individual, so they know — no matter what they tell me — that it’s safe,” he says.
“You want the best for everybody, but you can’t really push yourself too hard on them,” he added. “You’ve got to meet them where they’re at, and in their time they’ll come around eventually, you hope.”
Erie Street is just one block from the Haight Ashbury Free Clinic’s location in the Mission district. It’s a long alleyway of sharp shadows and slants of sunlight. On the day we walk past, there is a tent at the far end, and a guy on a stepladder, spray-painting a mural on a large blank wall.
“It’s heartbreaking — I used to get high in this alley, too,” Eric says. “I feel for these individuals.”
He spots some new faces.
“Hey, guys,” he booms, smiling and striding over. “You need any socks?”
A man and a woman are cuddled together with just thin sleeping bags against the hard sidewalk.
Nearby is a shopping cart stuffed with belongings and a cooler. A pit bull puppy flops across their legs. They sit up and happily accept everything Eric offers.
“Hey, so you guys, you guys need any medical attention at all?” Eric asks. “Do you got Medi-Cal?” he asks, referring to the Medicaid program in California — the health insurance for low-income people.
The young couple — Sean and Kat — are from Mendocino County, they tell us, and have been in San Francisco for only a month. They are trying to a quit a drug habit, and NPR agreed not to use their last names. They need advice, and Eric has plenty: They talk about places to get day-old pastries; charities that offer free breakfast or lunch; and places to shower. Eric points out the nearby clinic. They discuss getting the puppy fixed at the SPCA, which is also in the neighborhood.
“You guys use?” Eric asks. “I mean I’m an old junkie, all right?”
“We’re working on quitting,” Kat says.
“Oh what, heroin?”
“No,” says Sean.
“Meth?”
“Yeah.”
“Slamming it?”
“No.”
“Smoking?”
“Yeah, we smoke.”
Kat tells Eric she used to slam, meaning she used to inject the drug. But after meeting Sean, she was able to stop that. He helped her “get off the needle.”
Eric jumps on this point: “Really? So you guys are together. And you’re supporting one another, all right?”
Giving up the needle is a small step, but a positive one. It’s a little less harmful. Eric wants them to know he gets it: They’re trying.
“So, you guys, come and talk to me, OK?” he tells them. “Seriously, if you want help at all. I don’t care if you don’t want recovery or not, but just to know that there’s someone out there. I used to get high right here in this alley, dude — back in the day.”
Survival in consolidation
Today, the Haight Ashbury Free Clinics are part of an umbrella organization called HealthRIGHT 360. It’s a large network of social service agencies tackling a variety of issues besides health care: domestic abuse; rehabilitation for ex-inmates; gay, lesbian and transgender health issues, and addiction.
Consolidating with other agencies helped the Haight Ashbury Free Clinic survive.
Seven years ago, in 2010, it was struggling financially. Some staffers had been caught embezzling, and the clinic couldn’t afford the transition to electronic medical records — a requirement of the Affordable Care Act.
In 2011, the Free Clinic joined forces with Walden House, a nearby addiction recovery center. Other nonprofits soon joined as well, and HealthRIGHT 360 became the umbrella brand, allowing the smaller agencies to pool resources for administration, electronic records and fundraising.
Dr. David Smith, who started it all, applauds the decision to consolidate with other nonprofits. But he does miss the intimacy of those early days, he says, when volunteers from the neighborhood worked at the clinic.
When money got tight back then, they held benefit concerts, featuring local bands — like Big Brother and the Holding Company, during the time Janis Joplin was the lead singer.
After 1967, free clinics opened in Seattle, Los Angeles and Berkeley. By the end of the 1960s, the U.S. had dozens of free clinics — a third of them in California.
This story is part of a NPR’s reporting partnership with KQED and Kaiser Health News.
Opioid Policy Becomes Personal For One Health Official After Husband's Death


Precision Medical Treatments Have A Quality Control Problem

Careful custody of blood tests and tissue samples is essential to the success of precision medicine.
David Silverman/Getty Images
hide caption
toggle caption
David Silverman/Getty Images
You might not suspect that the success of the emerging field of precision medicine depends heavily on the couriers who push carts down hospital halls.
But samples taken during surgery may end up in poor shape by the time they get to the pathology lab — and that has serious implications for patients as well as for scientists who want to use that material to develop personalized tests and treatments that are safer and more effective.
Consider the story of a test that’s commonly used to choose the right treatment for breast cancer patients. About a decade ago, pathologists realized that the HER2 test, which looks for a protein that promotes the growth of cancer cells, was wrong about 20 percent of the time. As a result, some women were getting the wrong treatment. The trouble wasn’t with the test itself — problems arose because the samples to be tested weren’t handled carefully and consistently.
To reduce the error rate, doctors established guidelines in 2007 to assure that breast cancer specimens are handled correctly. But a decade later, that’s still the only test that has such strict guidelines.
The weakest link in the quality chain
“Why are breast cancer patients special?” asks Dr. Carolyn Compton, a pathologist and professor at Arizona State University. She has been pressuring her colleagues to improve tissue-handling standards for all types of cancer.
That means collecting samples quickly from the operating room, monitoring their condition, and getting them through the hospital to the pathology lab without delay.
“I don’t think physicians think this way about their entire medical system,” she says. The process of delivering tissue samples to the pathology lab “may be the weakest link in the quality chain.”
This is not just a question about making sure each and every patient gets the most appropriate treatment. It affects the science behind new tests and treatments. Those tissue specimens often end up being preserved in huge collections called biobanks, which are a foundation for the field of precision medicine.
“I don’t see how we’re going to get precision medicine at the end of the day, when everything under the hood is so imprecise,” Compton says.
She is not alone in her concerns.
“We need to be sure that the stuff they’re looking at is valid, accurate, reliable and reproducible,” says Dr. Richard Friedberg, who has just finished his term as president of the College of American Pathologists. He is also chairman of pathology at the University of Massachusetts Medical School-Baystate.
And he agrees with Compton that the quality of samples ending up in biobanks is simply unknown.
‘Garbage in, garbage out’
This isn’t just about surgical samples. For example, he says, you can’t tell just by looking at a tube of blood whether it’s OK. “If it was left on a window sill and hit 100 degrees, a lot of things change.”
The fact is, you can still run a test and still get what looks like a valid result, “but if it’s garbage in, it’s garbage out,” Friedberg says.
Compton’s concerns also extend to the complex, expensive equipment at the core of precision medicine, including machines that read DNA sequences. Results from one test are not necessarily comparable to results from another, run on an identical sample. And because each company that makes a sequencer uses proprietary algorithms to identify genetic mutations, it’s not possible for laboratory scientists to make an independent judgement about which reading is more likely to be correct, she says.
The good news is that DNA samples are less sensitive to being affected by poor treatment, so sample handling is less of an issue for genetic studies. But when there are problems, “you can’t make up for a bad sample,” Compton says. “So even with all of this technological magic, you can’t turn straw into gold with this machine.”
And results from pathology labs are not even the biggest source of error in the growing field of precision medicine. Compounding the uncertainty is that patients’ electronic medical records are littered with all sorts of errors, and that further complicates efforts to extract reliable results from this pool of “big data.”
But not everyone in the new world of precision medicine is so concerned about these quality-control issues.
“I am not a believer in garbage-in, garbage out at all,” says Dr. Atul Butte, director of the Institute of Computational Health Sciences at the University of California-San Francisco. (He also holds a chair endowed by Mark Zuckerberg, who made himself rich by exploiting big data with Facebook).
“I know that no one scientist, no one clinician or pathologist is perfect,” Butte says. “But I’d rather take 10 or 100 so-called mediocre data sets and find out what’s in common, then to take one who says they’re perfect at doing this kind of measurement.”
Finding meaning in the ‘noise’ of big data
It’s easier to find real things in clean data. But in the real world, he says, data are always full of errors. So when you find something in noisy data, it’s more useful in real-world settings.
In Butte’s view, it’s far more important to make lots of noisy data available, and to as many scientists as possible. “To me, I really want to see a world where I don’t just see five or 10 or 20 companies working in particular area, I want a thousand drug companies. I want 10,000 drug companies.”
Butte himself used noisy public data to identify genetic markers he says could be the basis for a test to help diagnose a serious complication of pregnancy, high blood pressure or preeclampsia. He founded a company to exploit that idea and then sold the company, so Butte considers his discovery a qualified success, even though human studies have not yet determined whether the test will be valid and useful.
Carolyn Compton says she’s heard similar arguments about the value of noisy data from colleagues. She says one argued that if you have a pile of manure, maybe there’s a pony in there somewhere. “I don’t see bending over backwards to create algorithms to do all the work to sort through all the manure when, in fact, you could have a pile of diamonds from the outset,” she says.
Funding agencies prize exploration over quality control research
Compton has been pushing for more rigorous standards in specimen handling since she was an official at the National Cancer Institute a decade ago. But she says funding agencies are more interested in providing support for exploring new ideas than in funding basic research on a seemingly boring subject, such as understanding the consequences of mishandling tissue samples.
Concerns about quality control of tissue samples were a major subject of conversation at the College of American Pathologists’ annual meeting in October. “We are moving faster and faster and faster as this whole precision medicine train is moving down the track,” says Dr. Tim Allen, a pathologist at the University of Texas Medical Branch in Galveston.
The struggle now is that there simply isn’t enough data to make science-based recommendations, but “I suspect standardization of these things is going to become a reality much quicker than I would have expected even a few years ago,” Allen says.
In the meantime, samples of unknown quality continue to flood into biobanks. That’s problematic because discoveries based on noisy data often turn out to be just plain wrong. So this enterprise inevitably will generate many false leads. And the expensive and most time-consuming part of research is finding out whether something that looks great in the lab actually works in people.
You can contact Richard Harris via email.
Pain Management Clinic Offers An Alternative To Opioids

Robert Kerley is recovering from an opioid addiction with help from Kaiser Permanente’s pain management program in Colorado.
John Daley / Colorado Public Radio
hide caption
toggle caption
John Daley / Colorado Public Radio
Seven years ago, Robert Kerley, who makes his living as a truck driver, was loading drywall onto his trailer when a gust of wind knocked him off. He fell 14 feet and hurt his back.
For pain, a series of doctors prescribed him a variety of opioids: Vicodin, Percocet and Oxycontin.
In less than a year, the 45-year-old from Federal Heights, Colo., says he was hooked. “I spent most of my time high, laying on the couch, not doing nothing, sleeping, dozing off, falling asleep everywhere,” he says.
Kerley lost weight. He lost his job. His relationships with his wife and kids suffered. He remembers when he hit rock bottom. One night hanging out in a friend’s basement, he drank three beers and the alcohol reacted with an opioid in his system.
“I was taking so much morphine that I respiratory arrested because of it,” Kerley says. “I stopped breathing.”
An ambulance arrived, and EMTs administered the overdose reversal drug naloxone. Kerley was later hospitalized. As the father of a 12-year-old son, he knew he needed to turn things around. That’s when he signed up for Kaiser Permanente‘s Integrated Pain Service.
“After seven years of being on narcotics and in a spiral downhill, the only thing that pulled me out of it was going to this class,” he says. “The only thing that pulled me out of it was doing and working the program that they ask you to work.”
The program he refers to is an eight-week course, available to Kaiser Permanente members in Colorado for $100. It’s designed to educate high-risk opioid patients about pain management.
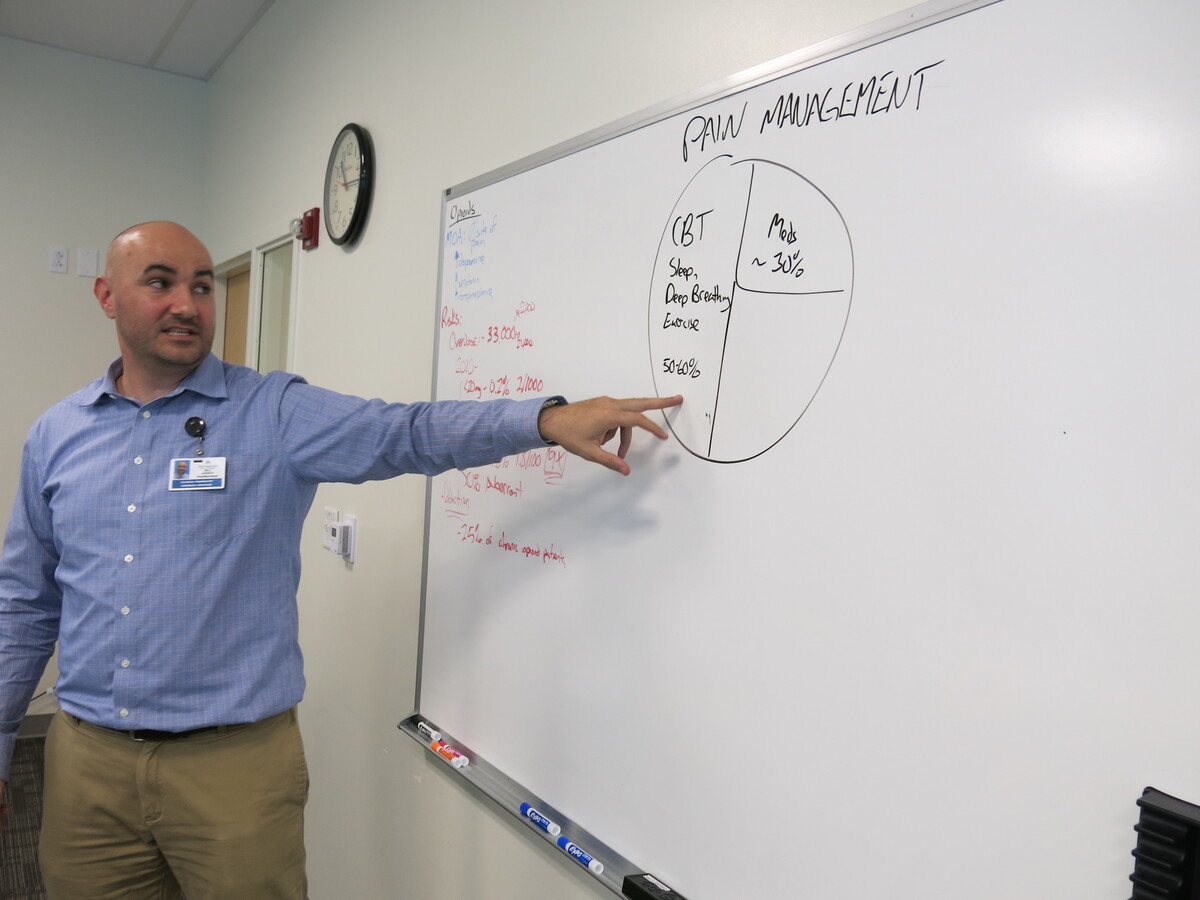
A recent class met at Kaiser’s Rock Creek medical offices in Lafayette, Colo., a town east of Boulder. Will Gersch, a clinical pharmacy specialist, was teaching several students battling addiction about the science behind prescription drugs. “So basically the overarching message here is: the higher the dose of the opioids, the higher the risk,” he tells the group as he jots numbers on a whiteboard.
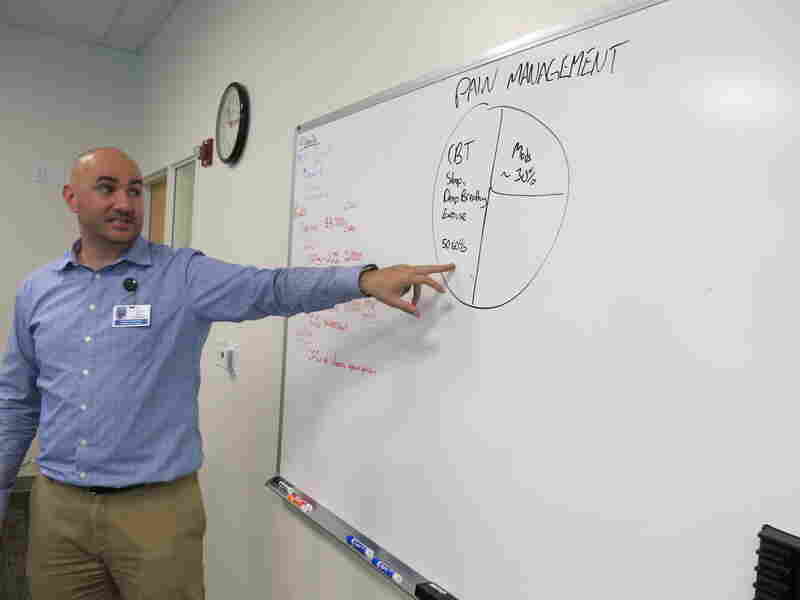
Will Gersch teaches a class as part of a Colorado Kaiser Permanente pain management clinic.
John Daley / Colorado Public Radio
hide caption
toggle caption
John Daley / Colorado Public Radio
Upstairs, his colleague Amanda Bye, a clinical psychologist, highlights a key element of the program: It’s integrated. For patient care, there’s a doctor, a clinical pharmacist, two mental health therapists, a physical therapist, and a nurse all on one floor.
Patients can meet with this team, either all at once or in groups. They don’t have to deal with a series of referrals and making appointments with doctors in different facilities.
And it seems to be working. Kaiser researchers tracked more than 80 patients over the course of a year and found the group’s ER visits decreased 25 percent. Inpatient admissions dropped 40 percent and patients’ opioid use went way down.
“We brought in all these specialists. We all know the up-to-date research of what’s most effective in helping to manage pain,” Bye says. “And that’s how the program got started.”
Bye says the team helps patients use alternatives to drugs like exercise, meditation, acupuncture and mindfulness. Still, some patients do need to go to the chemical dependency unit for medication-assisted treatment.
Amanda Bye, a clinical psychologist, works as part of an integrated medical team to treat people with chronic pain at Kaiser Permanente.
John Daley / Colorado Public Radio
hide caption
toggle caption
John Daley / Colorado Public Radio
Benjamin Miller is an expert on integrated care with the national foundation Well Being Trust. He says Kaiser is on the right track.
“The future of health care is integrated and unfortunately, our history is very fragmented and we’re just now catching up to developing a system of care that meets the needs of people,” he says.
Similar projects in California showed a reduction in the number of prescriptions and pills per patient, says Dr. Kelly Pfeifer, director of high-value care at the California Health Care Foundation. Her group released case studies of three state programs similar to Kaiser’s in Colorado.
“We’ve seen great success with these models that are integrating complementary therapy, physical therapy, behavioral health, and medical care,” Pfeifer says. A key strategy is to gradually decrease the amount of opioids a patient takes, rather than cut them off before they’re ready. “It works so much better when the patients have access to these complementary therapies,” she says. “And it works even better when those complementary therapies are part of an integrated team.”
But it can be difficult to implement universally. One challenge is scale. Big systems like Kaiser have ample resources and can afford to run programs like this. Another is payment. Some insurers won’t pay for alternative treatments, others have separate payment streams for different kinds of care.
“Frequently, behavioral health and medical health are paid for by entirely different systems,” Pfeifer says.
The need for programs like Kaiser’s is urgent. In 2016, a record 912 people died from an overdose in Colorado, according to data recently released by the state health department. Three hundred of those people died from an opioid overdose. Opioid use often leads to an addiction to heroin, which claimed another 228 lives last year. Those two causes together now rival the number of deaths from diabetes, car accidents, or chronic liver disease.
Colorado faces a severe shortage of treatment options. Making matters worse, just this month, the state’s largest substance abuse treatment provider, Arapahoe House, announced it would close Jan. 2.
Kaiser Permanente’s Integrated Pain Service has given some patients a second chance. Robert Kerley, now a veteran of the program, recently shared his story with other patients. “I got my life back. I can sleep. I can eat. I can enjoy things,” Kerley told them.
To cope with pain, Kerley starts his morning with stretching and a version of Tai-chi that he calls “My-chi.” He practices deep breathing. His advice to others suffering from pain or addiction?
“Do whatever it takes to walk away from it, like no matter what,” Kerley says. “Trust me, it gets better. It gets 100 percent better than where you’re at right now.”
Better for Kerley means his relationships with his family have improved. And he’s back at work, once again able to make a living as a truck driver.
This story is part of a reporting partnership with NPR, Colorado Public Radio and Kaiser Health News, which is not affiliated with Kaiser Permanente.
Will Gathering Vast Troves of Information Really Lead To Better Health?

Scientist Michael Joyner rides his bike to work every day because he believes the exercise has more of an impact on people’s BMI than their genetic profile.
Richard Harris/NPR
hide caption
toggle caption
Richard Harris/NPR
The Mayo Clinic is building its future around high-tech approaches to research known as “precision medicine.” This involves gathering huge amounts of information from genetic tests, medical records and other data sources to ferret out unexpected ideas to advance health.
But one longtime scientist at the Mayo Clinic isn’t playing along. Dr. Michael Joyner is a skeptical voice in a sea of eager advocates.
Joyner’s lab studies exercise. It is, fittingly enough, in a hospital building founded in the 1880s. While Mayo has built all sorts of new labs at its sprawling campus in Rochester, Minn., Joyner can conduct his work without glitzy DNA sequencers and other high-tech tools of precision medicine.
And it’s not simply that he’s an old-school devotee. He believes that the solution to our most pressing health problems lies in thinking about whole human beings, not breaking everything down to DNA sequences.
“The enthusiasm for this [precision medicine] is occurring in a country where life expectancy is actually falling,” he says as he walks through the old linoleum-tiled halls of St. Mary’s hospital.
That fact alone leads Joyner to ask whether the money being poured into high-tech medical research is really solving the nation’s stark health problems, like obesity, heart disease, high blood pressure, diabetes, Alzheimer’s disease and cancer.

Volunteer Greg Ruegsegger is outfitted with monitors, a catheter threaded into a vein and a mask to capture his breath in an experiment run by Joyner to measure human performance.
Richard Harris/NPR
hide caption
toggle caption
Richard Harris/NPR
Joyner says there are certainly appropriate places to use this technology, and he doesn’t dispute the individual stories of success his colleagues tout. But he believes the best way to address the health concerns facing the nation is by studying — and treating — whole people, not by breaking the problems down to billions of genetic bits and pieces.
He practices what he preaches in both his personal life — his thorough exercise routine includes commuting by bicycle — and in his physiology lab.
On the day I visited at the end of August, volunteer Greg Ruegsegger was outfitted with monitors, a catheter threaded into a vein and a mask to capture his breath. He would exercise to the point of exhaustion while scientists studied him. This is far more informative than any genetic test, Joyner says.
“People have looked at 3,000 elite endurance athletes — these are people who compete in the Tour de France and win Olympic medals in cross-country skiing and distance running — and [scientists] have been unable to find any genetic marker for superior performance.”
And when it comes to the health of ordinary people, Joyner talks about real-world studies, which show that walking or biking to work has four- or fivefold more influence on a person’s body mass index than that person’s genetic profile.
Joyner is focused on how the body’s systems work together during exercise, but the same interconnectedness applies to many diseases. That’s why cancer drugs that target one biological pathway generally don’t last long. Tumor cells simply find workarounds, exploiting the redundancies deeply embedded in biology. And that’s why Joyner has so little faith in science that keeps trying to focus down on smaller and smaller details.
“One of the things we have to ask ourselves when we get these big initiatives is, ‘What’s the definition of success?’ ” he says.
Scientific discoveries alone don’t do it for him. Doctors need to build effective treatments — and patients need to follow along. This is the promise of precision medicine in the long run, but Joyner has published articles (like this one) skeptical of the drive to collect vast piles of information, hoping to make sense of it later.
“Is this just going to be a biological Tower of Babel,” he asks, or will this information also lead to discoveries that translate beyond the laboratory and actually change public health for the better?
He doesn’t doubt that DNA sequencing and other tools of precision medicine are useful in specific instances, such as for diagnosing rare diseases. There are a few uses in cancer treatment, but so far there has been just one randomized study of patients assigned to treatments based on their tumor’s DNA profile, and it showed no advantage over traditional medical judgment.
This isn’t a popular point of view elsewhere at the Mayo Clinic, which is sinking hundreds of millions of dollars a year into precision medicine. The shiny new labs across campus seem a world apart from Joyner’s physiology lab.
After my conversation with Joyner, Mayo public affairs officers eagerly led me to a series of scientists there who disagree with him. One stop was at the Medical Genome Facility.
This room is chock-full of machines that cost many hundreds of thousands of dollars apiece. They can analyze DNA from a person, a tumor or even a single human cell. They can read out an entire genome, or just a subset, which is called the exome.
“I really do believe that understanding our genome is fundamental,” says Julie Cunningham, one of the facility’s three co-directors. Like other scientists at Mayo, she has had swaths of her own exome sequenced.
“I learned that by and large I’m really lucky, but I learned that I have two [genetic] variants that affect how I respond to particular drugs that are out there.” She had actually known that before for one of those drugs, “but now I know exactly why I have it and it’s potentially serious. That has to be good. There’s nothing wrong with that.”
Bad drug reactions are a serious medical problem, so in principle, a genome profile should help reduce that risk. The reality, though, is that the vast majority of genomic tests for drug sensitivity give ambiguous answers.
One of the most carefully studied examples involves the blood thinner warfarin. Four separate studies show that people who got genomic testing for this susceptibility did no better — or only marginally better — than patients whose dosages were determined by traditional strategies.
This lack of strong data is a problem for many areas of precision medicine.
“Although we think conceptually this is going to be of high value, and it will ultimately improve health care with better quality and lower cost, we have to prove that,” says Keith Stewart, a hematologist who directs Mayo’s Center for Individualized Medicine. “If it doesn’t all pan out the way we expect that’s OK, but I think there will be plenty of unexpected areas that we haven’t conceptualized yet, so I think it’s a very worthwhile investment on the taxpayers point of view.”
Whether precision medicine is going to be a boom or a bust, “right now it’s just speculation on both sides,” he says.
“It is somewhat inevitable that every person in this country will have their genome sequenced.” he adds.
Gianrico Farrugia, a gastroenterologist who is chief executive officer of the Mayo Clinic in Florida, agrees.
“What we’re beginning to see is that technology is invading and replacing traditional testing,” says Farrugia. For example, it is already used to determine treatments for lung cancer and diagnose rare diseases.
And, in any event,he says medicine is already moving aggressively into this new territory and there’s no going back. “That’s not only wrong,” he says, “it’s impossible.”
With the momentum now built up behind this enterprise, precision medicine will be judged like much of modern medicine: in hindsight, after it becomes entrenched in clinical practice.
You can contact Richard Harris via email.
Why Some Teen Moms Can't Get The Pain Relief They Choose In Childbirth

Throughout the U.S., minors are generally required to have permission from a parent or legal guardian before they can receive most medical treatment. However, each state has established a number of exceptions.
PhotoAttractive/Getty Images
hide caption
toggle caption
PhotoAttractive/Getty Images
In 2011, before she became a nurse practitioner, Maureen Sweeney was working as a registered nurse in labor and delivery at a Cleveland-area hospital. She helped hundreds of women deliver their children, many of whom were minors in their early teens.
That’s because, in Ohio, the rate of teenage pregnancy is slightly higher than the national average. This year, about 23 in 1,000 teenage girls will become pregnant.
One patient in particular from those nursing school days sticks out in Sweeney’s mind.
“It was a 15-year-old woman who was coming in, in labor, to the emergency room,” Sweeney remembers.
The teen was scared. She didn’t talk much and didn’t trust any of the doctors. She told Sweeney she had no family and that she was a runaway.
“She was by herself and she was living on the streets or between friends’ houses,” Sweeney says.
In that moment, Sweeney became the young woman’s only support system to help her through the delivery of her baby.
“So as it progressed and it got more and more painful, she did request an epidural,” Sweeney says.
An epidural is a common type of regional anesthesia that eases the pain of labor. As she had done many times before, Sweeney followed hospital protocol and called the anesthesia department. But to her shock, they told her they could not help her young patient.
“They said that without parental consent, … she would not be able to sign for her own epidural,” Sweeney says.
In Ohio, people under 18 who are in labor cannot consent to their own health care. They can receive emergency services, but nothing considered to be elective. For the many Ohio minors who become pregnant, it’s a painful gap in coverage.
It’s also complicated by the fact that in Ohio, there is no legal process for emancipation: A minor’s parents must be deceased, or the minor must be married or enlisted in the armed forces to be granted independent legal status.
Ohio lawmakers are considering legislation that would allow minors to determine their own care during pregnancy. Colorado and North Dakota passed similar laws in recent years.
Abigail English, director of the Center for Adolescent Health and the Law, studies consent laws that govern minors. She says most states do allow pregnant teens to consent to their own care. One by one, it seems holdout states are moving in that direction, too, she says — once someone advocates for the change.
Delivery room doctors and nurses are often the ones pushing for that change.
When the hospital wouldn’t authorize an epidural for the 15-year-old Sweeney was caring for in 2011, Sweeney called the office of Cuyahoga County Children and Family Services; oftentimes an agent from children’s services can sign for medical consent in these cases. But it was 3 a.m. The young woman was in active labor and an agent couldn’t make it to the hospital until 9 a.m.
Sweeney remembers how hard to was to tell her patient the news.
“I had to go in, sit down with her and talk about the fact that she wasn’t going to be able to get an epidural, and she was going to have to do this naturally,” Sweeney says.
That’s when the young woman broke down, Sweeney says, and folded in on herself in tears.
Throughout the U.S., minors are generally required to have permission from their parents or legal guardian before they can receive most medical treatment that’s not considered emergency care. However, each state has established a number of exceptions.
According to the Guttmacher Institute, 26 states allow minors 12 and older to get prescription methods of contraception without a parent’s or guardian’s consent, and just two allow minors to consent, on their own, to an abortion. Ohio is one of more than a dozen states with no explicit policy allowing a minor to consent to prenatal and pregnancy-related care.
Diana Thu-Thao Rhodes directs public policy for Advocates for Youth, an advocacy organization that focuses on, among other things, the rights of minors to get access to health care. She says in the last few years, minor-consent laws in some places around the country have become increasingly restrictive.
“We can legislate minors’ decision-making much easier because of the fact that they are minors,” says Thu-Thao Rhodes.
Dr. Michael Cackovic, an obstetrician at The Ohio State University Wexner Medical Center, says every couple of months he sees a teenage mom who, under Ohio law, is unable to receive elective treatment, like an epidural. He says it’s frustrating to see patients in unnecessary pain.
“First of all, from a labor and delivery standpoint, you don’t like to see anybody uncomfortable,” Cackovic says.
Both Cackovic and Sweeney report that, just as frequently, they’ve had cases where the mothers intentionally denied their teenage daughters an epidural – as a sort of punishment for getting pregnant.
All Cackovic can do is try to talk them out of it.
“To take the mom aside,” he says, “and say, ‘You know, this isn’t some life lesson here. This is basically pain — and there’s no reason for somebody to go through that.’ “
This gap in Ohio law bars a young mother from choosing a C-section. And she can’t consent for a procedure to test for chromosomal abnormalities in the fetus.
Cackovic says he thinks that’s pretty backward: After she gives birth, the teenage mother can consent to the care of her baby, but she can’t consent to the prenatal procedure that would help pinpoint a diagnosis.
There is no way to know for sure how many teens across the country are denied these elective procedures. Thu-Thao Rhodes says in states like Ohio these young patients have been overlooked by lawmakers because they’re not in a position to advocate for themselves.
“The priority for a lot of these young people is to just get the basic health care and services they need,” Thu-Thao Rhodes says, “not spending unnecessary, and often unavailable, time and resources navigating complicated healthcare and legal systems.”
This story was produced in partnership with WOSU and Side Effects Public Media, a reporting collaborative focused on public health. A web-only version originally ran in Shots in September; listen to the audio above to hear from an Ohio woman, Shani Rucke, who couldn’t get the epidural pain relief she wanted during childbirth because she was 15 years old at the time, and her mom said no.
For Children, A Good Booger Joke Helps The Medicine Go Down

Where are we? In the sinuses, with some dancing green mucus.
Rodale Kids
hide caption
toggle caption
Rodale Kids
Dr. Howard Bennett creates elaborate Lego sculptures, juggles squishy balls during office visits and transforms exam gloves into water balloons, but it’s his booger and fart jokes that crack up even his grumpiest pediatric patients.
“Kids of any age are curious about their bodies,” the pediatrician writes in his latest book, The Fantastic Body: What Makes You Tick & How You Get Sick, “especially if what they’re learning about is gross! That’s why kids laugh hysterically if someone tells a booger joke or lets out a big, juicy fart in class.”
Bennett, who practices in Washington, D.C., has been writing about children’s health for years, in books and in a column for The Washington Post. The Fantastic Body includes fun facts about lice, pimples, warts and other nasty stuff, but he also explains to children how muscles work, how you digest food, what’s going on inside your brain and heart, how to treat common ailments and how to avoid getting sick in the first place. This interview has been edited for length and clarity.
How did you discover that telling gross jokes could help children feel more comfortable?
Adults are typically scared about what’s wrong with them. Children are scared about what you’re gonna do to them, but in both cases, patients need to know that you’re interested in why they’re there, interested in them as people, that you care about them. There’s lots of different ways to do that. You don’t have to talk about pee and poop. You can talk about the weather, politics, and you can be kind and very serious and still get it across.
It just so happens that part of me never grew up, so pee and poop and that kind of stuff, my patients’ parents see that their kids like this, and so they let me go with it because they realize it makes the kids feel more comfortable.
In the adult world, research has shown that if you come into my office, and I spend just a minute talking to you about something unrelated to why you’re there, you’ll be more satisfied with the visit, and you’ll be more likely to do what I’m suggesting you do, so it improves patient compliance. It’s not just touchy-feely stuff. It actually has an impact on health care.
Do your strategies work even with very sick kids?
One time when I was in the ER, this child was very scared, and somebody called me over to see if I could do something ’cause I guess I had a little bit of a reputation for being childlike, if not childish. He was in his bed wearing Ernie pajamas and Ernie slippers, and I pulled out my Ernie puppet. I swear I could have put a tube in the child’s throat, and he would have said ‘Thank you.’ He was mesmerized. By taking out Ernie, I showed him that I liked kids, and I liked toys, and if I liked toys, maybe I’m not a jerk.
Do your jokes ever backfire?
At one visit, I was ranting about potty humor, and the mom said, “Dr. Bennett, we don’t use potty humor in our house.” For the next 20 years, I never used potty jokes with them. Another mom wrote me a letter explaining that my humor is inappropriate and offered to take me out to lunch to teach me how to interact with children. I declined.

The Fantastic Body shows kids how their bodies work, including what’s going on in the nose and mouth.
Rodale Kids
hide caption
toggle caption
Rodale Kids
I went into the room once with this girl who got hit on the head with a lacrosse ball, and the first thing she said is, “My head really hurts; I don’t want any jokes,” so I didn’t do any. You get a feel for it, but still, anybody can mess up. If people know that your intentions are good, I think it’s OK.
When did you start writing books, and how did you decide to write The Fantastic Body?
The first book I did was The Best of Medical Humor in 1991. Then I did Waking Up Dry: A Guide to Help Children Overcome Bedwetting in 2005, and I saw there was a perfect way to put together my writing for kids and my working with kids. You know that standard line about write what you know? It finally sort of came together. The Fantastic Body grew out of my KidsPost columns. There are a lot of gross books out there, but this was the first time anybody put the body, physiology, medical facts and gross stuff all together.
What’s your favorite gross fact in the new book?
One of my favorites is a sidebar in the skeleton chapter. When lobsters molt, and they’re just these things crawling around with no shell, people in the lobster industry refer to them as turds, so this is perfect. I’ve got a medical fact, and I’ve got a gross fact all wrapped into one.
Lauren Kafka is a freelance writer, editor and English tutor and founder of Kafka Consulting in Bethesda, Md. Her twins have been Dr. Bennett’s patients for 19 years. She’s on Twitter: @LaurenKafka

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A side view of the eye shows how he iris works — and a sad little tear.
Rodale Kids
hide caption
toggle caption
Rodale Kids
Radio Replay: Don't Panic!

{kind=link}
After a long history of civil war and corruption, many Liberians didn’t trust their government’s attempts to control Ebola.
John Moore/Getty Images
hide caption
toggle caption
John Moore/Getty Images
It may sound like the plot of a movie: police find a young man dead with stab wounds. Tests quickly show he’d had Ebola.
Officials realize the suspects in the case, men in a local gang, may have picked up and spread Ebola across the slum. These men are reluctant to quarantine themselves and some – including a man nicknamed “Time Bomb” – cannot even be found.
This scenario actually unfolded in the West African country of Liberia in 2015. And what followed was a truly unconventional effort by epidemiologists to stop a new Ebola outbreak.
On today’s Radio Replay, we hear how those epidemiologists built trust to prevent an epidemic. Then, we talk with author Tim Harford about the surprising benefits of messiness and chaos in our everyday lives.
Hidden Brain is hosted by Shankar Vedantam and produced by Maggie Penman, Jennifer Schmidt, Rhaina Cohen, Parth Shah and Renee Klahr. Our supervising producer is Tara Boyle. You can also follow us on Twitter @hiddenbrain, and listen for Hidden Brain stories each week on your local public radio station.
Robust Health Insurance Sign-Ups Surprise Supporters And Opponents

{kind=link}
Kelley Mui helps a client sign up for health insurance through the Affordable Care Act on Dec. 15 at the Midwest Asian Health Association in Chicago.
Scott Olson/Getty Images
hide caption
toggle caption
Scott Olson/Getty Images
A day after President Trump said the Affordable Care Act “has been repealed,” officials reported that 8.8 million Americans have signed up for coverage on the federal insurance exchange for 2018 — nearly reaching the 2017 number in half the sign-up time.
That total is far from complete. Enrollment is still open in parts of seven states, including Florida and Texas, that use the federal HealthCare.gov exchange but were affected by hurricanes earlier this year.
The numbers released Thursday by the Department of Health and Human Services also did not include those who signed up between midnight Dec. 15 and 3 a.m. ET on Dec. 16, the final deadline for 2018 coverage, as well as those who could not finish enrolling before the deadline and left their phone number for a callback.
And enrollment has not closed in 11 states, including California and New York, as well as Washington, D.C., that run their own insurance exchanges. Those states are expected to add several million more enrollees.
The robust numbers for sign-ups on the federal exchange — 96 percent of last year’s 9.2 million total — surprised both supporters and opponents of the health law, who almost universally thought the numbers would be lower. Not only was the sign-up period reduced by half, but the Trump administration also dramatically cut funding for advertising and enrollment aid. Republicans in Congress spent much of the year trying to repeal and replace the law, while Trump repeatedly declared the health law dead, leading to widespread confusion.
On the other hand, a Trump decision aimed at hurting the exchanges may have backfired. When he canceled federal subsidies to help insurers offer discounts to their lowest-income customers, it produced some surprising bargains for those who qualify for federal premium help. That may have boosted enrollment.
“Enrollment defied expectations and the Trump administration’s efforts to undermine it,” says Lori Lodes, a former Obama administration health official who joined with other Obama alumni to try to promote enrollment in the absence of federal outreach efforts. “The demand for affordable coverage speaks volumes — proving yet again the staying power of the marketplaces.”
“The ACA is not repealed and not going away,” tweeted Andy Slavitt, who oversaw the ACA under President Barack Obama.
The tax bill passed by Congress this week repeals the fines for those who fail to obtain health coverage, but those fines do not go away until 2019. Still, that has added to the confusion surrounding 2018 coverage.
And it remains unclear whether Congress will make another attempt to repeal the law in 2018.
“I think we’ll probably move on to other issues,” Senate Majority Leader Mitch McConnell, R-Ky., said in an interview Thursday with NPR.
Kaiser Health News is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation.
FDA Commissioner: Are The Incentives Right For Orphan Drugs?

{kind=link}
Dr. Scott Gottlieb, Food and Drug Administration commissioner, told Kaiser Health News the incentives intended to spur development of drugs for rare diseases deserve a fresh look.
J. Scott Applewhite/AP
hide caption
toggle caption
J. Scott Applewhite/AP
Food and Drug Administration Commissioner Scott Gottlieb is questioning whether the law that encourages drugmakers to develop medicines for rare diseases is working the way it should.
In an interview this week, Gottlieb said the Orphan Drug Act of 1983 has provided “an enormous amount of public health value” over the years. But the “market has changed,” he said, and it’s time to ask: “Do we have the right incentives in place?”
The nearly 35-year-old law created incentives for companies to develop “orphan drugs” considered not financially viable because they treat rare diseases affecting fewer than 200,000 people. Those incentives include a waiver on millions of dollars in fees, seven years of market exclusivity and a tax break for research and development expenses.
The law proved successful. In the decade before it passed, only 10 industry-supported rare-disease drugs had been brought to market, according to the FDA. Since then, more than 450 individualorphan drugs have been approved.
Today, the medicines often carry six-figure price tags and pharmaceutical companies eagerly develop them. In 2016, 41 percent of the new drugs approved by the FDA were orphans. And 2017 is on track to be a record year.
“Clearly, [the Orphan Drug Act] has delivered,” said Bernard Munos, a former corporate strategy adviser at drug giant Eli Lilly who is now a senior fellow at FasterCures. “In that same vein, I think a problem that we didn’t anticipate some 30 years ago is the pricing crisis.”
In the past year, the high prices of rare-disease drugs sparked controversy. Examples include Marathon Pharmaceuticals, which priced its drug for Duchenne muscular dystrophy at $89,000 drug a year, and Strongbridge Biopharma, which relaunched a glaucoma drug dating back to the 1950s as an orphan drug to treat a rare neuromuscular condition. The drug’s annual price tag is now at least $109,500.
The top 100 orphan drugs in the U.S. cost an average of $140,442 per patient last year, according to EvaluatePharma.
Gottlieb’s comments come after a year of scrutiny for orphan drugs.
An investigation by Kaiser Health News that NPR published and aired in January found that many drugs with orphan status weren’t entirely new when approved. Of about 450 drugs that have won orphan approval since 1983, more than 70 were drugs first greenlighted by the FDA for mass-market uses. Those include the cholesterol blockbuster Crestor, Abilify for psychiatric disorders, and the rheumatoid arthritis drug Humira, the world’s best-selling drug.
More than 80 other orphan drugs won FDA approval for more than one rare disease, and in some cases, multiple rare diseases. For each approval, the drugmaker qualified for a fresh batch of incentives. Altogether, KHN’s investigation found that about a third of drugs given the FDA’s orphan status have either been repurposed mass-market drugs or drugs that received multiple orphan approvals.
Gottlieb and other industry analysts have said that repurposing common drugs to treat rare diseases is scientifically sound and good for patients. But Gottlieb has also said high drug prices are a public health concern, and in the phone interview Wednesday he questioned whether the financial incentives should be different for drugs that receive “secondary approvals.”
“It could very well be that you need to think differently about how you would create a framework around the secondary indication and the primary indication,” Gottlieb said, adding that he doesn’t have an answer but the agency has been asking the question.
At the same time, he pointed to rare diseases without treatments, even under the current incentive system: “You have to ask why various uses of drugs aren’t getting studied.”
Paul Melmeyer, director of federal policy at the National Organization for Rare Disorders, said there is a lot of unmet need since nearly 7,000 diseases lack treatments for an estimated 30 million Americans.
While Gottlieb can change agency guidelines, any change to the Orphan Drug Act’s incentives would require congressional action. There may be an appetite for such a change.
Gottlieb became commissioner in May, a few months after three key Republican senators called for a federal investigation into potential abuses of the Orphan Drug Act. The Government Accountability Office began an investigation in November.
Congress included changes to orphan drug incentives in its sweeping tax legislation, reducing the orphan drug tax credit from 50 percent of research and development coststo 25 percent — a move that will save the government $32.5 billion from 2018 to 2027. Earlier versions of the bill included transparency requirements and an elimination of credits for repurposed drugs — both of which were struck from the final version.
Gottlieb, though, has not waited for the GAO or Congress before doing what he can to revamp the program. In late June, he announced a modernization plan that included closing a loophole that allows manufacturers to skip pediatric testing requirements when developing a mass-market drug for treating rare diseases in children.
When asked about the coming year, Gottlieb said: “We are going to look for other ways to make sure the program is achieving its public health goals.”
Sydney Lupkin contributed to this report. KHN’s coverage of prescription drug development, costs and pricing is supported in part by theLaura and John Arnold Foundation.
Kaiser Health Newsis a nonprofit news service covering health issues. It is an editorially independent program of theKaiser Family Foundationthat is not affiliated with Kaiser Permanente.