Patriots Taking Antonio Brown’s Status ‘One Day At A Time’ Following Rape Accusation

Wide receiver Antonio Brown was sued in federal court by his former trainer who claims Brown sexually assaulted and raped her. As the NFL investigates, the Patriots say they are standing by Brown.
Jeff Chiu/AP
hide caption
toggle caption
Jeff Chiu/AP
Embattled Patriots wide receiver Antonio Brown is expected to practice with the team on Wednesday, a day after Brown’s former trainer accused him of rape in a federal lawsuit.
In a combative press conference, Patriots coach Bill Belichick said the accusations “are what they are” and that “I won’t be entering into a discussion about that right now,” adding that the team is taking the latest controversy involving Brown “one day at a time.”
Brown’s future was thrown further into question on Wednesday after news reports that the NFL is considering whether to place the star wide-receiver on leave in light of the lawsuit. The Washington Post first reported that the NFL is giving “serious condition” to making Brown ineligible to play.
Brown has not been charged with any crime.
His lawyer, Darren Heitner, released a statement denying the accusations against his client. “Mr. Brown denies each and every allegation in the lawsuit. He will pursue all legal remedies to not only clear his name, but to also protect other professional athletes against false accusations,” Heitner said.
On Tuesday, a former trainer accused Brown of sexual assault and rape in a federal lawsuit filed in the U.S. District Court for the Southern District of Florida, where Brown resides.
In the suit, Britney Taylor, 28, says she met Brown when they both attended Central Michigan University and were bible study partners. Brown transferred to Louisiana State University, but the two kept in communication.
According to the suit, Brown messaged Taylor, who runs a gymnastics training center in Memphis, on Facebook and asked her to assist him with “improving flexibility and strength in his ankles and fast twist muscles,” and that she agreed to help.
In June 2017, when the two were in one of Brown’s houses in the Pittsburgh area, Brown exposed himself to Taylor and then forcibly kissed her, according to the lawsuit. Taylor “willed herself to brush off the episode,” her lawyers say in the complaint.
The suit describes a subsequent episode when the two were streaming a church service at Brown’s home in Miami and the all-star wide receiver allegedly masturbated behind Taylor without her knowing. The suit contains degrading messages allegedly sent by Brown bragging about the incident.
The suit says Taylor ended contact with Brown but that he reached out months later, apologizing for his actions and asking her to train him again during off-season weekends. She agreed under the conditions that he not make advances on her and that he provide her with a private hotel room.
In May 2018, the lawsuit says, Brown invited her to a club in Miami with friends. Afterward, Taylor drove Brown and a friend back to Brown’s house and went to use the restroom. Brown allegedly then pulled her into his bedroom and raped her. The suit says Taylor pleaded with him to stop, saying “no” and “stop,” but that Brown refused.
Taylor talked about the alleged rape and the two other incidents with her mother, Brown’s chef and a member of her church, according to the lawsuit.
“Brown preyed on Ms. Taylor’s kindness and her religious devotion, casting himself as a person equally dedicated to his religious faith and someone she could trust. In reality, he used manipulation and false promises to lure her into his world, and once there, he sexually assaulted and raped her,” wrote Taylor’s lawyer, David Haas.
Brown said through his attorney that the relationship with Taylor was consensual.
“Mr. Brown, whose hard work and dedication to his craft has allowed him to rise to the top of his profession, refuses to be the victim of what he believes to be a money grab,” Heitner says.
Heitner says that prior to the alleged rape, Taylor reached out to Brown about a $1.6 million investment in a business project and that Brown turned it down.
A spokesman for the NFL declined to comment on the lawsuit. The Patriots said in a statement Wednesday that the team takes the allegations “very seriously,” saying the NFL has told them league officials will be investigating.
Brown is no stranger to controversy. He clashed with the NFL over regulations that would not allow him to use his preferred helmet.
Just last week, when he was with the Oakland Raiders, Brown recorded a conversation with coach Jon Gruden and posted it on YouTube. On Saturday, the Raiders voided a multimillion-dollar contract with the wide receiver and released him.
He was snapped up by the New England Patriots days later. He has yet to play a game with the Patriots.
California Could Radically Alter Amateur Rules In College Sports

The California State Assembly is on the verge of passing a law that would make it possible for the state’s college athletes to be paid for the use of their images to market products.
How To Teach Future Doctors About Pain In The Midst Of The Opioid Crisis

Tracy Lee for NPR
The next generation of doctors will start their careers at a time when physicians are feeling pressure to limit prescriptions for opioid painkillers.
Yet every day, they’ll face patients who are hurting from injuries, surgical procedures, or disease. Around 20% of adults in the U.S. live with chronic pain.
That’s why some medical students felt a little apprehensive as they gathered recently for a mandatory, four-day course at Johns Hopkins University in Baltimore — home to one of the top medical schools in the country.
The subject of the course? Pain.
“I initially was a bit scared and I guess a bit wary coming into this course because of the opioid crisis,” says medical student Annie Cho. “That seems like that’s the only thing that people have been talking about nowadays.”
She wasn’t the only one aware of how fraught pain can be right now. Student Jenny Franke says she’s been shadowing doctors in a clinic, and has already seen new patients come in with pain.
“And it seems that the therapy that they are on hasn’t been working, and a lot of the time their past primary care providers just keep prescribing the same thing over and over,” Franke says. “Sometimes those patients will ask for opioids, and then it turns into kind of an awkward conversation.”
Even though doctors see a lot of pain, medical schools traditionally haven’t dedicated much time to teaching future physicians about it, says Shravani Durbhakula, a pain management specialist at Johns Hopkins Hospital and director of the pain course this year.
“Most medical schools get about nine hours of formalized pain education,” says Durbhakula. “If I was to think back to my training, it probably is somewhere about that much time.”
While she remembers some classes on certain painkillers, she says, “I don’t remember a lot of formal pain education, certainly not any kind of course that was given to me. It was just something you kind of learned as you went along.”
“There are very few medical schools that have a course like ours,” agrees Jennifer Haythornthwaite, a professor in the Department of Psychiatry & Behavioral Sciences at Johns Hopkins University School of Medicine.
Most schools have integrated pain management throughout their curriculum, says Alison Whelan, chief medical education officer at the Association of American Medical Colleges, which represents hundreds of medical schools and teaching hospitals.
A couple of years ago, her group did a telephone survey of its members to see what they were teaching about pain. They asked about four important categories: what pain is, how you identify it and assess the severity, how you treat it, and how you deal with cultural and social issues related to pain management.
While 87% of medical schools reported teaching all of those pain-related subjects, there’s great interest in medical schools in coming up with new ways to bolster teaching about the management of pain.
And a recent review of a key medical licensing exam showed that most of the questions it asked about pain focused on assessment, rather than on safe and effective pain management.
Barbara Del Duke, a spokesperson for the National Board of Medical Examiners, says that every year, hundreds of volunteers gather to write new questions for this test. “The opioid epidemic is definitely on the minds of these volunteers,” she says. “We see evidence of this through the test items they write.”
All of this is a big change. About a decade ago, as the opioid crisis was taking off in the U.S., a Johns Hopkins neurologist and pain specialist named Beth Hogans looked to see what medical schools were teaching about these drugs.
“U.S. medical students were getting less than one hour, on average, of opioid- related instruction in medical school,” Hogans says. “That’s not enough.”
She helped create the four-day course at Hopkins, with the idea of giving all students a solid foundation for thinking about pain and pain management at the start of their medical education.
Here, the students learn that pain is a physical and an emotional experience, and that doctors tend to underestimate pain. They learn how it can be affected by people’s moods, cultural expectations or individual sensitivity. They discuss problems with the usual way of asking patients to rate their pain on a scale of 1 to 10, and learn to instead ask if and how pain limits people’s daily activities.
And, of course, they talk about opioids. A doctor named Ryan Graddy asks the students to pull out their cellphones. He says they should text him a few words in response to this question: “What comes to mind when I say ‘chronic opioid therapy?’ “
Their answers start to appear on a big screen behind him. The first word is BAD. Other words pop up, including ADDICTION and DRUG ABUSE. The lecture hall fills with nervous laughter.
“So, interesting, right, a lot of negative connotations that people have with chronic opioid therapy,” says Graddy, who goes on to describe some of the challenges his patients face and why some have been on opioid pain medications long-term.
Overall, students get taught that opioids are just one tool in the toolbox — though one they will have to learn to use thoughtfully and carefully.
“You wouldn’t really use a chainsaw to cut a piece of paper. But you also wouldn’t use a pair of scissors to cut down a tree,” Cho says.
Over and over, speakers stress the need to build a relationship with patients rather than just write a prescription.
“We can’t just focus on that single moment of writing a script,” says bioethicist Travis Rieder, who shared a harrowing account of how he was prescribed opioids by about a dozen different caregivers after having an accident and then surgery. When he became physically dependent and wanted to stop taking opioids, he couldn’t find a doctor willing to help him get through his agonizing withdrawal.
Rieder’s experiences surprised medical student David Botros. “I really didn’t expect that to even be … I don’t want to say possible, but even a factor in the health care world, I guess,” Botros says.
Botros and the other students heard about other possible medications, beyond opioids. And they learned that pain control goes way beyond just prescribing drugs. Patients could benefit from physical therapy, cognitive behavioral psychotherapy and all kinds of exercise, like yoga.
“You really need to address the whole person,” says Traci Speed, assistant professor of psychiatry and behavioral sciences at Johns Hopkins. She notes that co-occurring depression or substance use can increase the severity of pain. “It’s the chicken and the egg, which one do you treat first? And sometimes, you have to treat both to really get patients to improve.”
Graddy thinks the medical profession overall has been doing a disservice to patients when it comes to chronic pain. “I see that certainly in my own practice — a lot of patients who have bounced around from place to place and not been treated with the respect or dignity or empathy that they deserve,” he says.
That’s why this hospital invited patients and their families to this lecture hall, to movingly convey how pain impacts their entire lives. And these medical students definitely get the message.
“I felt like I learned a lot and it was very helpful,” Franke says. “One thing I learned was to really get into the patients’ perspectives and their values, and figuring out what their pain goals are. One important thing we learned is that it’s rare that you will get a chronic pain level to a zero.”
Tony Wang took this course two years ago and is just finishing his third year of medical school.
“The takeaway message that I distinctly remember leaving with was that pain management is extremely complicated,” Wang says. “It’s not just, give this medication and they’ll feel better.”
NFL Season Kicks Off With Refuges For Fans With Sensory Needs To Take A Timeout

Sheletta and Shawn Brundidge, alongside their four children, were the first fans to use the sensory room at the Minnesota Vikings’ U.S. Bank Stadium. Opened during the August pre-season, the space comes with trained therapists and provides fans, including those with autism, a break from the excitement of the game.
Tami Hedrick/Minnesota Vikings
hide caption
toggle caption
Tami Hedrick/Minnesota Vikings
The roar of the crowd, the boom of the sound system, the flash of fireworks — all part of the thrill for many fans who flock to NFL games, but for others, including those on the autism spectrum with sensory issues, the experience can be too much.
Now a growing number of teams are including “sensory inclusive spaces” within their arenas to accommodate them.
The Philadelphia Eagles, the Seattle Seahawks and the Minnesota Vikings have all opened rooms that provide a refuge for those who need to step away from the clamor. The spaces come equipped with dim lighting, sound-protected walls and sensory activities, including toys and games, with the goal of providing a reset.
And Julian Maha, co-founder of KultureCity, the nonprofit that worked with the Vikings and the Eagles to design the rooms, told NPR that there are many people who may need that reset.
“One in six people in the U.S. have a sensory need,” said Maha, who is also a medical doctor. That can include individuals not only with autism, but also Down syndrome, post-traumatic stress disorder and dementia; all challenges that Maha said may not be visibly apparent but come with “a freedom barrier.”
“The lights, the noises, the crowd can be not only overwhelming from a sensory aspect but also physically painful to them,” he said.
Valerie Paradiz, vice president of services and supports at Autism Speaks, who was diagnosed with autism as an adult, told NPR that for people on the autism spectrum, public sports events can be especially difficult to process. “By creating a calm space, these NFL stadiums encourage inclusion and enable people with autism, their families and friends to attend events together,” she said in an email.
Tami Hedrick, the Vikings’ director of women’s initiatives, worked to create the sensory inclusive space at U.S. Bank Stadium in Minneapolis.
She told NPR that the Brundidge family — whose three out of four children have been diagnosed with autism-spectrum disorders — were the first people to use the room when it opened during the August preseason. Hedrick said the room was a game changer for the family, as they would have been unable to attend without it.
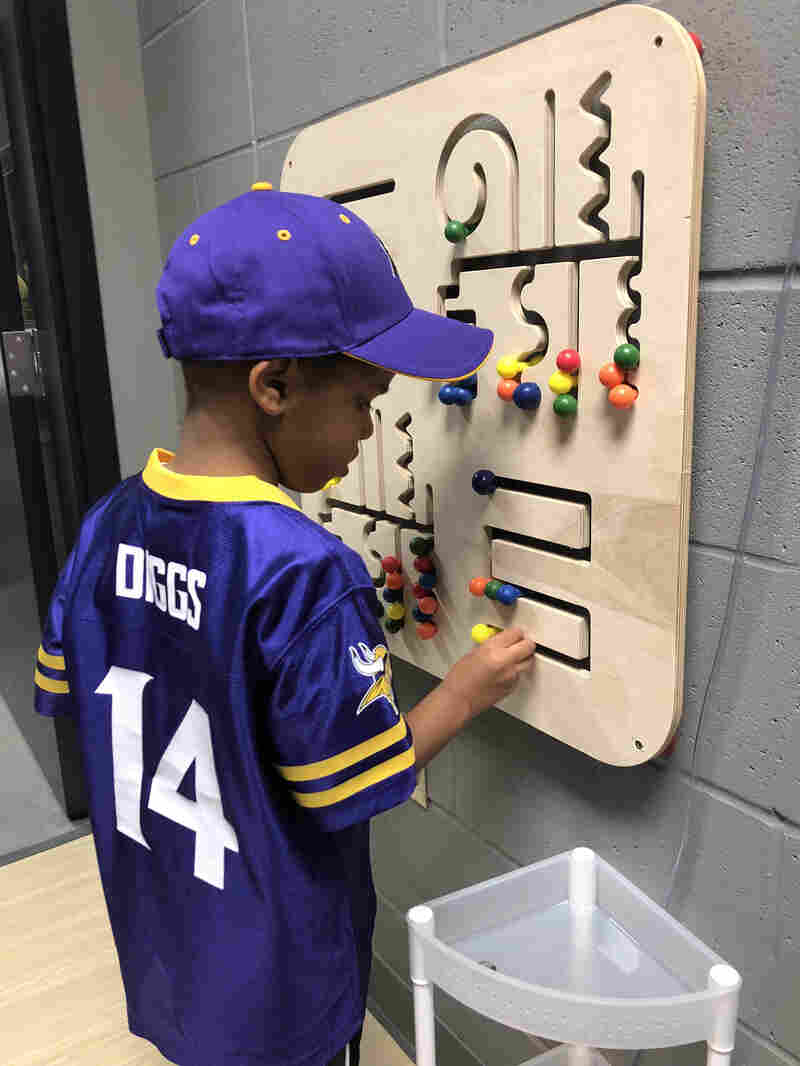
A child enjoys the sensory inclusive space at U.S. Bank Stadium during the Minnesota Vikings’ August pre-season.
Tami Hedrick/Minnesota Vikings
hide caption
toggle caption
Tami Hedrick/Minnesota Vikings
The room comes with two trained therapists and has so far averaged around 15 people per game, Hedrick said. Attendance is capped at four people at a time, and they are asked to stay for no longer than twenty minutes, although accommodations could be made as needed.
“We want to be able to have that privacy and to have that quiet,” he said. “All of them were only in there for about five minutes. They didn’t really need a lot more time.”
Several arenas, including the Denver Broncos’ Mile High Stadium, the New York Giants and Jets’ MetLife Stadium and the Pittsburgh Steelers’ Heinz Field, are also accommodating fans with special needs by offering tool kits with noise-cancelling headphones and sensory toys — known as fidget tools.
The kits come with a badge letting staff know that a fan can leave the arena and come back in.
KultureCity works with franchises to train staff to recognize what sensory needs look like. The training, Maha said, includes “the awareness and freedom you’re giving to this population to come into your facility without fear of judgement.”
Maha knows the feeling. His 11-year-old son was diagnosed with autism and is non-speaking.
He also adores basketball.
At one time, the family only got to enjoy a few minutes of an Atlanta Hawks’ game before having to leave. Now several NBA teams have added sensory rooms to their arenas, including the Hawks. Now, Maha said, his son can stick it out for an entire game, occasionally using the sensory room — and the kit — to decompress.
“It’s been transformative,” Maha said. “At the core, it gives families and individuals the freedom to re-engage with communities again.”
Looking Back At The Best Of This Year’s U.S. Open
NPR’s Ailsa Chang talks with Jon Wertheim of Sports Illustrated about the amazing play seen at the U.S. Open this year.
Telepsychiatry Helps Recruitment And Patient Care In Rural Areas

Doctors Say Federal Rules On Discussing Abortions Inhibit Relationships With Patients

Unlike Planned Parenthood which pulled out of Title X family planning funding, many clinics still take the funding and must comply with new rules on discussing abortion. Doctors worry it will affect their relationships with patients.
SDI Productions/Getty Images
hide caption
toggle caption
SDI Productions/Getty Images
Clinics that take federal Title X family planning funding are adjusting to a new set of rules that limit what health care providers can say to their patients about abortion.
Though Planned Parenthood pulled out of the program in August rather than comply with the rules, thousands of other clinics continue to use grants from the federal program for family planning and sexual health services. These clinics are now under pressure to make sure their staff comply.
The new regulations prohibit doctors in Title X-funded primary care clinics from referring pregnant patients for abortions, and also state that health care providers cannot “perform, promote, or support abortion as a method of family planning.”
Though the Department of Health and Human Services issued guidance that the regulations are not a “gag rule” and that doctors are still allowed to provide information about abortion, organizations that represent physicians are concerned that the ambiguity of the language in the rules will leave some doctors forgoing conversations about abortion entirely.
And some physicians worry the rules set a precedent that the federal government can regulate doctors’ speech in the exam room — a precedent that may erode the doctor-patient relationship.
“By restricting providers from delivering accurate information to their patients, including abortion referrals, the new Title X rule represents an inappropriate intrusion in the patient-physician relationship,” American College of Obstetricians and Gynecologists president Ted Anderson said in a statement.
Family physician Elliot Goodenough works at a community health center in Philadelphia that doesn’t provide abortions but uses funding from Title X to help pay for family planning services like birth control and HIV testing. He sees almost entirely low-income children and adults.
His job, he says, is to help them sort through their care choices and provide them with accurate medical information. Now Goodenough worries that he won’t be able to speak as freely.
“The role of the doctor is under question here,” Goodenough says. “Medical professionals are generally esteemed providers of information. That’s our main job.”
The provision about referrals is particularly perplexing to some physicians working in Title X-funded clinics, since referral from a primary care doctor is not typically required for abortion. Women can usually walk in to a clinic that provides abortions without seeing another physician first.
When patients come in with an unexpectedly positive pregnancy test, Goodenough says he tries to listen to their concerns and help them sort through their options. This can include giving them information about what to expect during an abortion and information about local clinics that provide abortions, he says.
While that’s not a referral in his mind, he says, he worries some of the counseling he used to provide would no longer be legal.
“I think I’ll have to figure it out as conversations come up,” Goodenough says.
According to David Cohen, a law professor at Drexel University who studies abortion, a government restriction on what doctors are allowed to discuss with their patients is a departure from the way medicine has typically been regulated in the U.S.
“Generally the law requires some basic things of physicians, in terms of compliance with regulation and informed consent, and then lets them practice medicine,” he says.
The American Medical Association joined Planned Parenthood and other organizations in a lawsuit challenging the rules in March, arguing in part that they “would force doctors to violate their obligation to give honest and informed advice.” That case is still making its way through the courts.
There have been a few other examples of American laws that attempt to restrict doctors’ speech, according to sociologist Carole Joffe, but most have been struck down by the courts for violating the First Amendment.
Joffe, a professor at University of California, San Francisco who studies abortion, points to a 2011 Florida law that attempted to prevent doctors from asking their patients about whether they own guns.
The 11th U.S. Circuit Court of Appeals struck down that law because of concerns about freedom of speech, stating in its majority opinion, “Florida does not have carte blanche to restrict the speech of doctors and medical professionals.”
The Title X restrictions are likely to be treated differently in court, Joffe says. Many states require abortion providers to counsel their patients about topics like adoption resources or a contentious procedure known as abortion pill “reversal,” even if some of the talking points aren’t backed by medical research. This type of mandated counseling unique to abortion has largely stood up in court, she adds.
Still, Joffe says she’s troubled by the reach of the Title X rules, beyond clinics that provide abortions and into general primary care.
“The idea that we’re going to regulate what a doctor can say to a patient is abhorrent,” Joffe says. “This relationship … should be, in some ways, so sacred. The patient is entrusting the doctor with the most important issues in his or her life.”
For some physicians who are opposed to abortion, however, the rules are a welcome opportunity to ensure that doctors’ counseling about pregnancy includes multiple options.
The rules don’t prevent doctors from talking about abortion when patients ask about it, notes Ingrid Skop, an obstetrician-gynecologist in Texas and the president elect of the American Association of Pro-Life Obstetricians and Gynecologists. She sees the rule as preventing doctors from pushing their patients towards abortions they may not want.
“It’s not gagging you,” Skop says. “It’s just saying, ‘Don’t make it a one-sided conversation, the way that informed consent should be.’ … This allows women to know what their options are but not to be directed in a particular direction.”
Before the Trump Administration change to Title X, clinicians working in Title X-funded clinics were required to provide “non-directive” counseling to pregnant patients, meaning that doctors were previously obligated to tell their patients about prenatal care, abortion services, and adoption. Under the new rules, doctors are allowed to withhold information about abortion services.
But for many clinics choosing to no longer participate in the Title X program, doctors’ concerns were significant enough that clinic leaders were willing to forgo millions of dollars in federal grants.
“We just felt like we couldn’t abide by these rules in good faith [and also] abide by our responsibilities to our patients,” says Ken Gordon, the CEO of Coos County Family Health Services, a network of community health centers in northern New Hampshire.
His clinics have never provided abortions, but his organization recently withdrew from using Title X funding due to concerns about how the new regulations would affect the doctor-patient relationship.
Coos County Family Health services is one of hundreds of clinics around the country — including many that provide abortions and many that do not — that announced it would no longer use Title X money. A Kaiser Family Foundation report found that over 900 clinics plan to withdraw from the Title X program, just under a quarter of all Title X-subsidized clinics.
“Physicians were concerned about the ethical and moral implications of withholding information from someone who was their patient,” Gordon adds.
Meanwhile, Joffe, the sociologist at UCSF, says she wonders if the move signals a decline in how much society trusts doctors to regulate their own profession.
“Are we seeing the declining authority of medicine?” she says. Historically, she says, “only doctors can regulate other doctors, only they understand the medical issues … I don’t really have a good handle on if [regulation like this] could spread to other areas of medicine. I could see arguments that it could.”
Mara Gordon is a family physician in Camden, N.J., and a contributor to NPR. You can follow her on Twitter: @MaraGordonMD.
Philly Teens ‘Work To Ride’ And Change The Face Of Polo

Schyler Smith, far left, Marc Harris and Shane Woodson are some of the younger members of Work to Ride in Philadelphia’s Fairmount Park.
Courtesy of Lezlie Hiner
hide caption
toggle caption
Courtesy of Lezlie Hiner
It started with a wrong turn while driving in Philadelphia’s Fairmount Park.
That was how 8-year-old Shariah Harris and her mother found the stables of an equestrian program called “Work to Ride.” Growing up in a West Philadelphia neighborhood where crime rates are high and graduation rates are low, Harris never dreamed of playing polo.
“Polo wasn’t something that was in the cards for me,” she says. “I couldn’t afford riding lessons, or a horse for that matter. I never even thought about riding horses until I got lost in the park that day,” she says.
But after finding the barn, Harris was hooked. Within days she was mucking stalls and grooming horses. By the age of 12, she was competing against some of the most elite polo teams. Being the only players of color on the field was tough at first.
“I was only around black people as a kid and then traveling out to games we were the only black people, so it was weird, we were kind of sticking out,” says Harris, who became the first black woman to play top-tier polo at the age of 19. The team eventually gained acceptance she says, especially when they started winning.

Shariah Harris (right) is one of the captains of the Cornell University polo team.
Courtesy of Lezlie Hiner
hide caption
toggle caption
Courtesy of Lezlie Hiner
But earning the privilege to ride takes work. Each morning the players wake up at dawn and get to work cleaning the barn, bathing, grooming and exercising the horses. If they show up late, they don’t play, says Lezlie Hiner, founder and coach of Work to Ride.
“It’s a progression with the kids,” Hiner says. “I’m very funky about being on time. That’s one of my big things in life, so I battle with the kids about that all of the time and if they really want to do something their behinds will be here.”

Lezlie Hiner is the founder and coach of Work to Ride. In 1994, she got frustrated with her desk job and quit to figure out a way to combine her two passions: her deep love for horses and helping at-risk youth.
Windsor Johnston/NPR
hide caption
toggle caption
Windsor Johnston/NPR
In 1994, she got frustrated with her desk job and quit to figure out a way to combine her two passions: her deep love for horses and helping at-risk youth. What she came up with was a program that gives low-income, inner city kids the chance to play polo for free in exchange for taking care of the ponies.
To stay on the team the players must maintain at least a C average in school. If they don’t, they’re demoted to barn chores until they get their grades up. That was the case for 14-year-old Mosiah Gravesande, who was sidelined last year for a bad report card.
“I felt bad because I was missing out on a lot and I just wanted to play, but I couldn’t because I was playing around and not paying attention to my school work,” Gravesande says.
In communities where the high school dropout rates are high, Hiner says she’s not surprised that some kids don’t make it.
“My main goal is to make sure that the kids graduate high school. Sometimes we have to provide them with tutors or interface with their schools, especially if there is no parental involvement,” she says.
Many of the players are raised in single-parent households that often lack structure and discipline. Lyzette Rosser enrolled her two sons in the program when they were in elementary school, and says Hiner has been a lifesaver over the years.
“She kept my kids from off the streets, I struggled to raise them and I couldn’t have done it without Miss Lez,” Rosser says.
Her son Kareem captained the Work to Ride team in 2011 when it became the first all-black squad to win the National Interscholastic Polo championship.

Shariah Harris competed in the Amateur Cup tournament in Tully, N.Y., this past August.
Courtesy of Lezlie Hiner
hide caption
toggle caption
Courtesy of Lezlie Hiner
“It was a time that we made history,” says Kareem, who went on to graduate from Roger Williams University in Rhode Island. Now at 26, he works as a financial analyst in Philadelphia. “It took us so long to get to that point, there was a lot of falling, broken mallets and tears, but just over the years being a resilient group we finally accomplished a long-term goal of ours.”
Clinching that title was also the moment when the polo establishment started to take notice.
“She’s changing lives,” says John Gobin, former captain of the U.S. polo team. “What she has done in Philly, people are trying to duplicate around the country and she’s raised those guys as gentlemen and fantastic polo players,”
Gobin says Hiner’s tough-love approach has gone a long way in helping the kids stay on track.
“Working with the horses teaches these kids to get out of bed in the morning. They have a lot of responsibility to get to the barn in the morning, feed the horses and make sure they have water, exercise, brush them. And they can’t get into trouble because they are in the barn 12 hours a day,” Gobin says.
But Work to Ride hasn’t been able to help all of the kids. Sometimes the players drop out of school or get into trouble with the law, a few have ended up in prison. Other times they’re lost to more tragic circumstances. In 2003, one of the team’s most promising players was murdered in her West Philadelphia home in a drug deal gone bad. Hiner thinks back to the last time she saw 14-year-old Mecca Harris.
“Mecca was our only female player at the time. We had just dropped her off that night after practice and then we got the call the next morning,” Hiner says.
Mecca’s picture now hangs above the door in the tack-room of Work to Ride.
For the last 25 years, Hiner has worked tirelessly to teach the kids life skills and responsibility, but education remains her top priority. She estimates that about 65 percent of those who sign up for Work to Ride will graduate from the program. She says it’s a good number, but not good enough.
But for the most part, the program has succeeded in keeping the kids off the streets, in school and on the polo field.

Mosiah Gravesande also competed in the Amateur Cup tournament in Tully, N.Y. He was sidelined last year for a bad report card.
Windsor Johnston/NPR
hide caption
toggle caption
Windsor Johnston/NPR
On a recent day, Shariah Harris and the Work to Ride team are in Central New York preparing to compete in the Amateur Cup, one of the biggest polo matchups of the summer.
On the sidelines of the Preble Valley Polo Club, Harris fastens a yellow do-rag around her head and tightens the reins on Easy Ed, a shiny, black thoroughbred. She says at first, the former racing horse had no interest in playing polo.
“He was a problem child at first,” Harris says. “He would bite me and some of the other horses, but over time we got used to each other and now he’s OK, he’s easier.”
Harris says learning how to establish a relationship with a horse was one of the biggest challenges she faced while learning to ride.
The horn blows signaling the last 30 seconds of the game and the team is down 7 to 1. Harris looks disappointed as she walks Easy Ed back to his trailer.
“I hate to lose more than I love to win. But losing helps you become a better player and you can’t learn if you always win,” she says.
The 21-year-old captains the polo team at Cornell University and will graduate next year with a degree in animal science. She’s also helping to expand Work to Ride by raising funds for an indoor arena – which is set to open in 2021.
But for now, Harris shakes off today’s loss and walks off the field wearing a bright, pink t-shirt that reads, “Polo: the sport of millionaires, royalty and homeboys.”
Rafael Nadal Claims His 19th Grand Slam Title With U.S. Open Triumph

Rafael Nadal brandishes the spoils of his U.S. Open final victory over Russian Daniil Medvedev on Sunday. The Spaniard’s win in New York City — his fourth U.S. Open title — gives him 19 career individual grand slam wins, just one shy of rival Roger Federer’s record.
Johannes Eisele/AFP/Getty Images
hide caption
toggle caption
Johannes Eisele/AFP/Getty Images
Rafael Nadal enjoys a well-earned reputation as tennis’ long-reigning king of clay — but on Sunday, Nadal reminded the world he’s anything but a one-surface wonder. The 33-year-old Spaniard reasserted his mastery of the hard court, as well, claiming his fourth career U.S. Open title over an opponent roughly a decade his junior.
Nadal defeated Daniil Medvedev in a five-set humdinger in New York City, 7-5, 6-3, 5-7, 4-6, 6-4. To do it, he had to fend off a furious rally by the 23-year-old Russian, who, after ceding the first two sets to Nadal, stormed back to push his celebrated opponent to the brink — and extend the marathon match’s final running time to nearly five hours.
But Nadal ultimately steadied his course, breaking Medvedev’s serve twice in the final to seal the victory and buttress his position in the record books. The win makes for his second Grand Slam title of the year, after he won the French Open — yet again — in June. It also gives him his 19th career Grand Slam, placing him just one title behind arch-rival Roger Federer, who currently owns the men’s singles record.
After the match, Nadal wept as the stadium in Flushing Meadows played a string of highlights from his career. He called it “one of the most emotional nights of my tennis career.”
Not a dry eye in the house after this match!
?: @usopen | @RafaelNadal | #USOpen pic.twitter.com/Iuv0kuthxg
— ATP Tour (@ATP_Tour) September 9, 2019
“The last three hours of the match have been very, very intense, no?” Nadal said. “Very tough mentally and physically, too.”
No kidding.
For all the history Nadal brought to Sunday’s match, and all the edge in experience he had over Medvedev — a newcomer to the U.S. Open final — Nadal’s win did not come easily. Despite clinching the first two sets, the Spaniard saw the next two slip away on broken serves. What looked early on like a possible cruise to triumph ended up taking about 4 hours, 50 minutes, in what became one of the longest matches of Nadal’s considerable career.

Rafael Nadal splays across the court after fending off a furious comeback attempt by Daniil Medvedev on Sunday. Nadal won the marathon match, but it took him five sets in New York City to do it: 7-5, 6-3, 5-7, 4-6, 6-4.
Timothy A. Clary/AFP/Getty Images
hide caption
toggle caption
Timothy A. Clary/AFP/Getty Images
“The way that he was able to fight, to change the rhythm of the match, was just incredible,” Nadal acknowledged afterward.
Medvedev, for his part, made clear that the respect was mutual.
“What you’ve done for tennis in general,” he told Nadal at the trophy ceremony, calling his career Grand Slam total simply “outrageous.” “I mean, I think 100 million kids watching you play want to play tennis, and it’s amazing for our sport.”
They Dress From The Bottom Up: Sneakerheads Converge In D.C.

The line of attendees waiting to get in stretched down the hall, up the stairs, and outside the building. Sneaker Con organizers expect more than 10,000 people to show up to the event this weekend.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
A line stretches down the hall, up the stairs, and out the door at the Walter E. Washington Convention Center in Washington, D.C. The voice of an event organizer echoes throughout space: “No fakes! We catch you selling fakes, you’re getting kicked out!” he warns. “Embarrassment!”
It’s Sneaker Con. Organizers say they are expecting about 10,000 people to converge at the convention center over the weekend for this stop of the global tour.
Sneaker Con is exactly what it sounds like.
“Everybody’s out here buying sneakers, trading sneakers. Every sneaker you can imagine,” describes Tamika Jeter.
She’s a stylish Baltimore native wearing a pair of black and white checkered Commes Des Garcon x Nike Cortez Platform sneakers that retail for $390.
It’s her first time at Sneaker Con but, a self-proclaimed sneakerhead, Jeter’s excited by what she sees. “Exclusives, some [sneakers] that you haven’t seen in years,” she says. “Everything’s here. For the sneaker fan, this is the place to be.” She has her eyes out for a good deal on some Yeezy 700s, a collaboration between Adidas and Kanye West.

Tamika Jeter poses for a photo at Sneaker Con. A self-proclaimed Sneakerhead, she says she has always liked sneakers but they became part of her lifestyle after she broke her toe. She’s pictured wearing the Commes Des Garcon x Nike Cortez Platform Sneaker which retails for $390.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
People come from all over the country to buy, sell, and trade sneakers, at this event. Organizers say that it’s one of the few places where people can still physically gather together to talk sneakers. These days more and more people RSVP for new shoes online and wait for a digital drop rather than waiting in lines wrapped around a Footlocker for hours.
The event started in 2009 in New York to celebrate sneaker culture, and has since evolved to include a digital marketplace, an app, and has even developed an authentication process that includes tagging shoes with microchips to indicate that they’re real. It helps keep fake shoes out of the marketplace.

Attendees bring their shoes to have them tested and authenticated to make sure they’re real.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
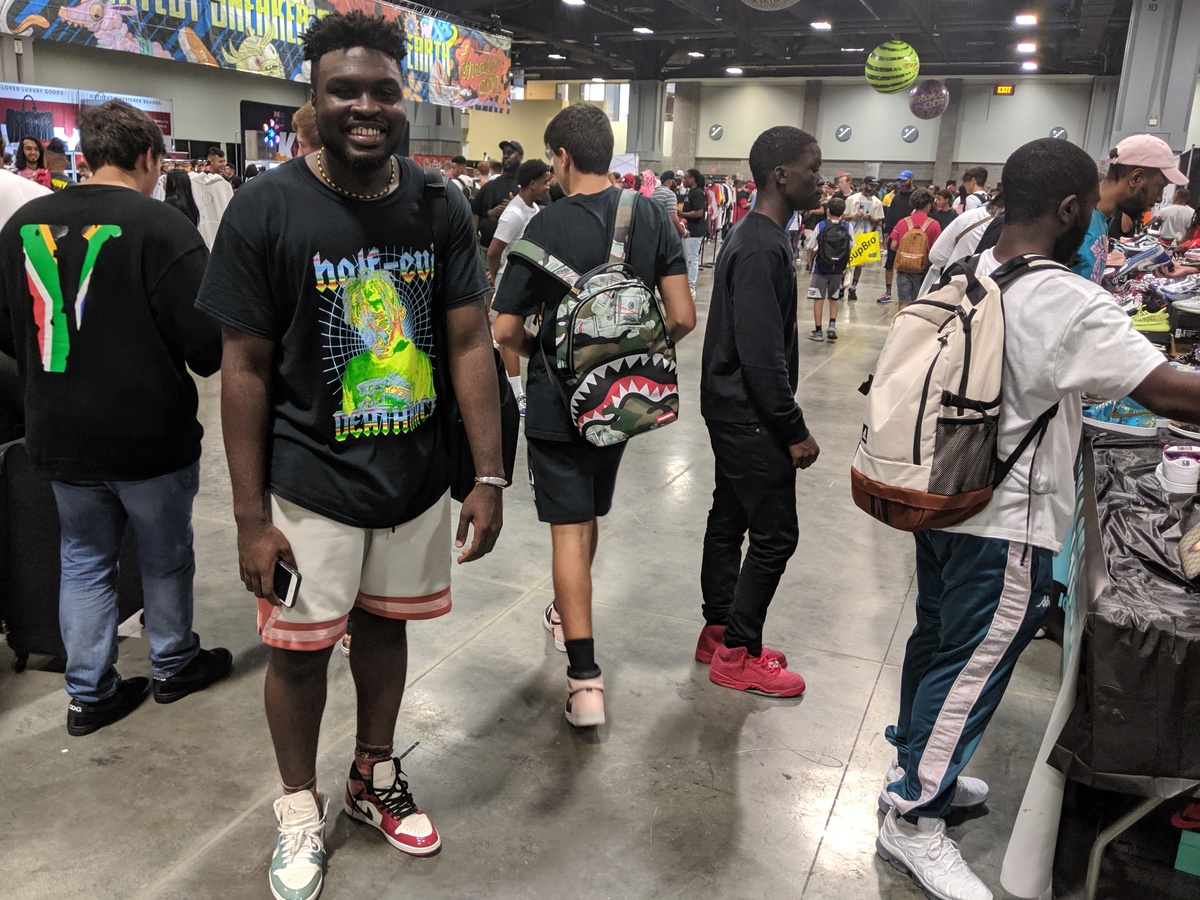
Fakes can create problems in a peer-to-peer marketplace like this. Organizers say that’s just part of what happens when an item is popular or valuable. But, attendees like 20-year-old Yusuf Lewis, say the biggest issue is an over saturation of resellers.
Lewis flew to D.C. for Sneaker Con from Atlanta, Ga. He’s the first person in line at the event and even though he says he loves sneakers, that’s not really what the event is about for him anymore. “It’s becoming more of a resellers playground instead of a person who’s passionate about sneakers,” he says. “It’s not their playground anymore.”
For many people, reselling shoes makes them a lot of money. And Lewis has done pretty well for himself too. He says he travels to almost every Sneaker Con using the money he makes from buying and selling shoes. But for many other attendees the prevalence of resellers makes it hard to participate in the sneaker culture.
Comte Momo of Washington, D.C., says he doesn’t like all of the reselling and it’s hard for him as someone who actually wants to wear the shoes to find the ones he wants at a reasonable price. “It just hurts when I watch somebody buy a size 12 in the new ones that dropped. And I just know that they’re gonna go resell instead of a person like me loving and cherishing the shoe” he says. “But, get your bread. I can’t be mad.”

Comte Momo poses for a photo. He was on the hunt for a pair of Zoom Kevin Durant 4 All Star Galaxy shoes. He had a pair in his collection that he sold to help pay for rent but now it’s hard to find a pair to fit his size 12 feet. He’s pictured in the Jordan 1 Retro Chicago Bulls Patent on his left foot and the Jordan 1 Retro UNC on his left foot.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
Yuming Wu, one of the co-founders of Sneaker Con says he isn’t worried about the balance between resellers and buyers.
“This show is not about buying, selling and trading,” he explains. “Obviously, there is a lot of commerce happening here. But for us, we’re really about putting together a great vibe for for people who are interested in this subject to hang out with other people.”
There are plenty of other things to do at the convention like a watch a basketball game of 1-on-1 knockout, or interact with artists creating shoe- related artwork and doing customizations, or attend panels featuring people in the shoe industry.
Wu says, as the convention moves into its tenth year, he wants to incorporate much more programming and turn the convention into more a festival.

People watching isn’t nearly as fun as sneaker watching at Sneaker Con. Many come to make a fashion statement as much as they come to buy, sell, or trade shoes. Sneakerheads get dressed from the bottom up.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
Buying, selling, and trading may not be entirely what the show is about, but it is the central activity at Sneaker Con. At least here in Washington, D.C.
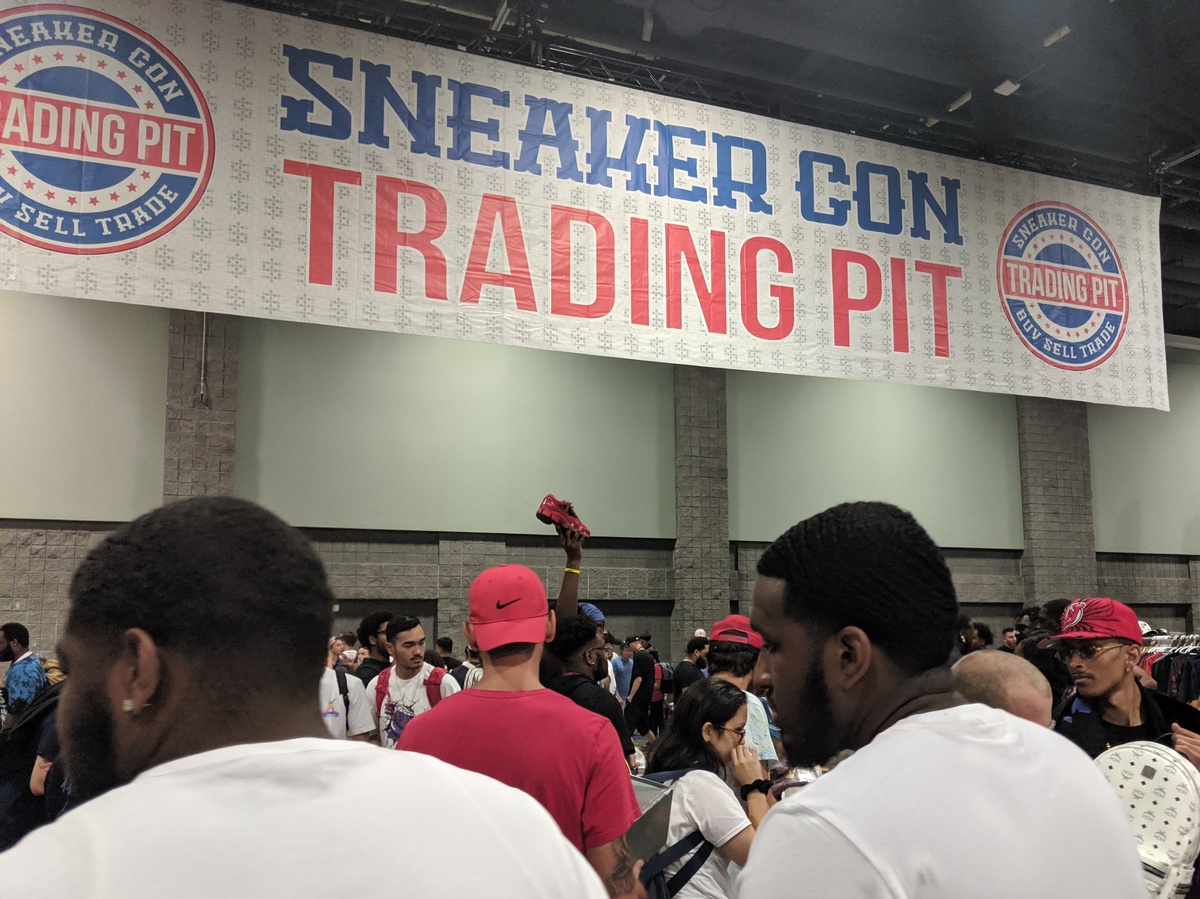
Much of the space is taken up by more than 200 vendors who have set up tables and brought hundreds of pairs of shoes to try and sell. Some people just walk around with a couple pairs in hand looking to trade or sell to a willing buyer. But most of the action, the bargaining, haggling, and trading, is happening in the trading pit.
Anyone who wants to, can bring as many shoes as they like and create a space for themselves on the floor.

It helps to have long arms in the trading pit. People who choose not to purchase a vending table can bring as many shoes as they can carry to trade amongst everyone else. Without display tables or much space, most simply advertise their shoes by holding them up in the air.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
That’s where 18-year-old Lateef Amdali is set up.
“A goal for me is to definitely go home with a couple of sneakers that I’ve been wanting for a while,” he says. “And definitely sell some things I’m trying to get rid of in my collection to make a profit off of it.”
He says he started buying and reselling shoes when he was around 13 years old.
“I was asking my mom and dad to buy me sneakers [and] sometimes they’ll say ‘no,’ so I had to find a way to get them myself,” he says. When he figured out that he could resell his shoes for a profit, then buy more shoes, and resell those, he quickly turned his hobby into a business.
“I just got really into it and learning [that] I can make money from this I didn’t have to have a job necessarily,” he says as he sells pair of shoes for $280 dollars cash.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lateef Amdali, 18, stands with his collection of shoes. Amdali starting buying and selling shoes by the time he was 13 years old. He says his most memorable flip to date netted him over $1,000 in profit off of just one shoe.
Mayowa Aina/Mayowa Aina
hide caption
toggle caption
Mayowa Aina/Mayowa Aina
Children as young as 10 years old like Theo Galpert of Chevy Chase, Md., were in the trading pit too getting in on the action. He says he learned about buying and reselling from his older brother 13-year-old Bennett. Their father, Josh Galpert, says that he’s impressed by what his sons are doing. “I think it teaches a lot about how to build a business and what goes into building a business,” he says. “And that’s been fascinating to watch how they price things, how they negotiate, how they keep track of their inventory, which is a challenging thing to do when you’re you know, 13, 10, and 7.”
Co-founder Wu says it’s a mixture of everything; the commerce, the artistry, the fashion, that makes sneaker culture attractive around the world.
“A sneakerhead in Melbourne, Australia, they’re as interested in Nikes, Jordans, [and] Yeezys as much as the kid in in Phoenix, Arizona.” Or here in Washington D.C.
Meantime, back in the trading pit, Amdali says even though his goal is to make a profit, it’s not just about money. “I definitely have my own sneaker collection. My [Jordan] ones collection goes crazy — 18 pairs right now,” he says. “I love the game.”
For Amdali, and Sneaker Con, the games continues year-round.