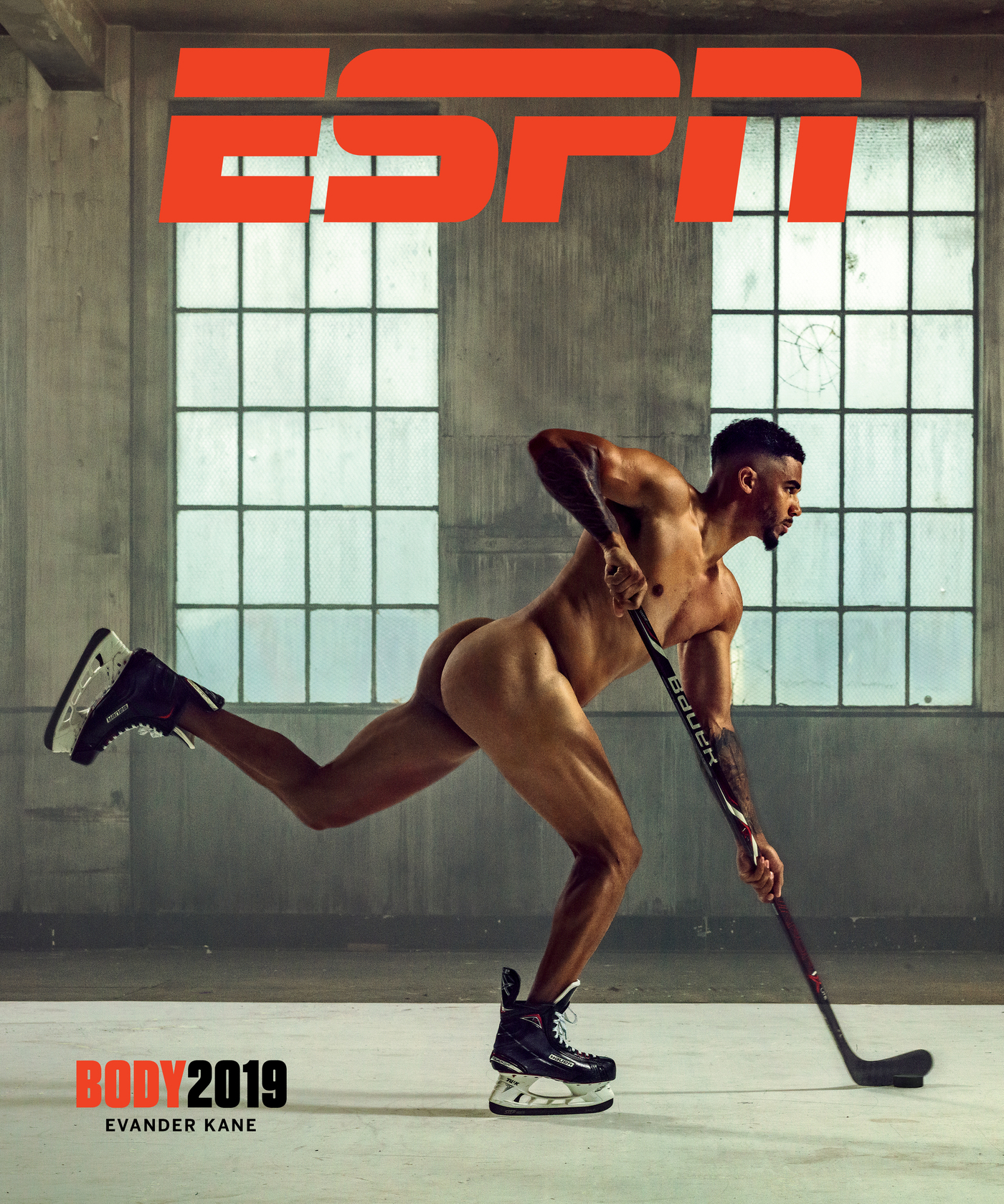
ESPN Celebrates Variation Of Athletic Bodies In Final Print Edition Of Its Magazine

When ESPN The Magazine set out to create its Body Issue, the idea was to celebrate how varied athletic bodies really are. The last print edition of the annual issue, which is also the last print edition of the magazine, is being released this week.
Marcus Eriksson for ESPN
hide caption
toggle caption
Marcus Eriksson for ESPN
Athletes’ bodies are on display constantly. Whether they’re running, climbing, jumping, throwing, skating, hitting or engaging in any other motion, we’re watching them. But how often do we stop to think about how varied those bodies are?
That is exactly what ESPN The Magazine set out to do with its Body Issue. The annual issue is meant to celebrate athletes from across the sporting world and across gender, from the superfamous to the less well-known, in carefully composed nude photographs.
Athletes including Serena Williams, Hope Solo, Prince Fielder, Gus Kenworthy, the U.S. women’s national hockey team, the Philadelphia Eagles’ offensive line and many other fan favorites have graced the multiple covers that each issue features. Along with the images showcasing all different types of athleticism, the magazine has included interviews with athletes talking about body image, discussing their struggles with it and portraying that many body types are capable of athletic feats.
This special feature has been a highlight for the past decade, but last week ESPN published its final print edition of the magazine after 21 years. ESPN announced in April that the September issue of the magazine would be its last. In a statement, the company said the work and features by journalists for the magazine would not end, but that based on consumer trends, the content would move entirely to the digital platform.
The company is expected to launch ESPN Cover Story this fall, bringing many of the “high-concept franchises born in ESPN The Magazine“ to a monthly digital presentation that showcases features on athletes.
To mark the moment and get a sense of how the idea for The Body Issue came to creation, NPR’s Michel Martin spoke with the magazine’s editor in chief, Alison Overholt, on All Things Considered.
This interview has been edited for length and clarity.
Interview Highlights
On where the idea for The Body Issue came from
There were some conversations that came actually out of the action sports and X Games world, where some of the athletes had done an art project where they took nude photos. And they are actually very beautiful. I mean, you started to get a sense that body types were very different depending on the sport.
Then there was sort of perpetual conversation around training and fitness. And, you know, body has never actually gone so explicitly into that space. But this felt like a way for us to begin to talk about what do athletes do in order to make their bodies into the machines that they are?
On getting athletes to sign on at the beginning
My first year was crazy. We openly had conversation about how this might be completely impossible. We also knew that it would hinge on one or two influential people saying yes and that making other people feel safe. And it actually hinged on Serena Williams. Our editor in chief at the time approached her on the red carpet at the ESPYs and asked her if she would do this and had an elevator pitch ready and explained to her what he thought it could accomplish. She was a star, of course, but she was building her public image and her reach with fans beyond tennis.
She looked at him and, you know, asked him a couple of questions and then said, “Would you put me on the cover?” And he said yes. And she said, “I’m in.” She was our first Body cover. For her to do that made other athletes say, “You know, all right. This is something.”
On sensitivity and working conditions during photo shoots
We take a lot of special steps. One of the earliest conversations that we had specifically about Body was the need to bring it, you know, into focus around a mission statement that we developed that’s very simply “Everybody has a story.”
So every single piece that we did, every time we approached an athlete, we wanted to know, first, what’s your body story? You know, what is the story that they want to tell? Then we work with them to figure out what would be the creative expression visually of that story. And based on that, we’re pairing people with photographers who can bring that vision to life.
We’re talking to them about, you know, do you feel more comfortable with an open set or a closed set? Do you want to bring people with you who are going to make you feel more comfortable? They’re looking at images on-screen as they’re coming through, which is something that, you know, we don’t do at every single shoot. But for something like this, you need to be comfortable with the material.

When Scout Bassett, a Paralympic track and field athlete, decided she wanted to do The Body Issue, she told ESPN she wanted to make sure people could see her scars.
Richard Phibbs for ESPN
hide caption
toggle caption
Richard Phibbs for ESPN
On a special story in the last issue
There’s a young woman in the issue named Scout Bassett. And she is a Paralympic track and field athlete. She was born in China, and she was abandoned and an orphan and was actually caught in a terrible house fire at a very, very young age. As a result, she lost her leg. She wasn’t adopted by her American family until she was, you know, probably middle elementary school and didn’t begin running until she was into her teens. And she became an incredibly accomplished track and field athlete. She now competes at UCLA.
When she decided she wanted to do The Body Issue, she was very specific with us and said, “I want to make sure people can see my scars because I want them to understand that scars are part of what makes you who you are. And, you can have strength and beauty and power even after overcoming an experience like what I went through.”
NPR’s Robert Baldwin III and William Troop produced and edited this interview for broadcast. Wynne Davis produced it for Digital.
How A Prenatal ‘Bootcamp’ For New Dads Helps The Whole Family

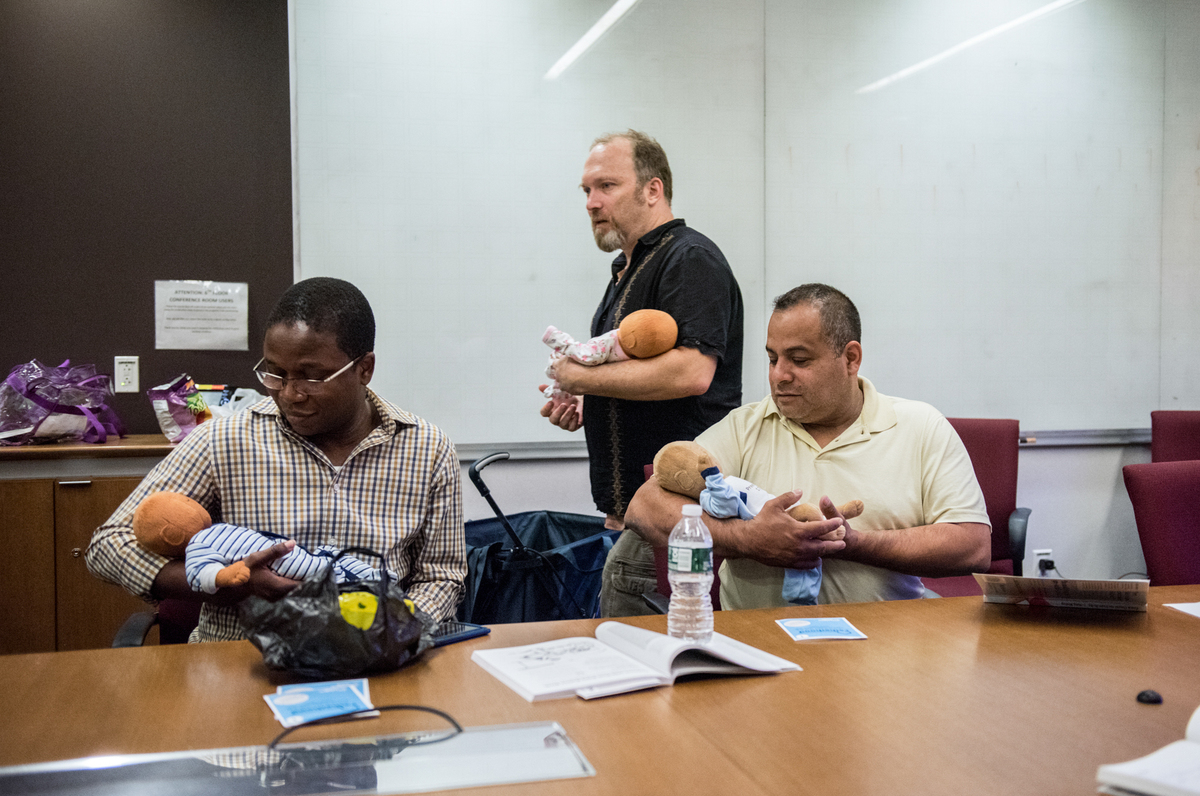
Joe Bay (center), coach of a New York City “Bootcamp for New Dads,” instructs Adewale Oshodi (left) and George Pasco in how to cradle an infant for best soothing.
Jason LeCras for NPR
hide caption
toggle caption
Jason LeCras for NPR
“Before I became a dad, the thought of struggling to soothe my crying baby terrified me,” says Yaka Oyo, 37, a new father who lives in New York City. Like many first-time parents, Oyo worried he would misread his newborn baby’s cues.
“I pictured myself pleading with my baby saying, ‘What do you want?’ “
Oyo’s anxieties are common to many first-time mothers and fathers. One reason parents-to-be sign up for prenatal classes, is to have their questions, such as ‘What’s the toughest part of parenting?’ and ‘How do I care for my newborn baby?’ answered by childcare experts.
However, though prenatal classes show both parents how to swaddle, soothe, and comfort their infants, they are usually aimed mostly at the mom — discussing her shifting role and how to cope with the bundle of emotions motherhood brings.
With that focus, “Dad’s parenting questions can fall to the wayside,” says Dr. Craig Garfield, an associate professor at Northwestern University’s Feinberg School of Medicine and an attending physician at Lurie Children’s Hospital in Chicago. And the lack of attention to a new father’s needs can have ripple effects that impact the whole family — in the short-run and later, Garfield says.
Around the U.S., a number of health care providers, such as Garfield in Chicago and the non-profit ‘Bootcamp for New Dads’ in New York City, have begun trying to change their approach to such classes. Some go so far as to hold single-sex prenatal classes specifically for men.
“Because each parent holds a separate role in their child’s life, expectant mothers and fathers may seek different answers to their parenting questions,” Garfield explains.
Indeed, raising children is nothing new, but parenting culture has shifted in the U.S., over time. For instance, compared to parents of the 1960s, today’s mothers and fathers tend to focus more of their time and money on their children, a recent study suggests, adopting what sociologists call an “intensive parenting” style.
Parental worries about their kids’ academic success and future financial stability may drive this parenting philosophy, researchers say.
These mounting responsibilities can stress the family, which is why mothers and fathers may feel eager to define their parenting roles. While a new mother’s role in modern society is often directed by her baby’s needs to breastfeed, cuddle and sleep; a new father’s role isn’t always spelled out.
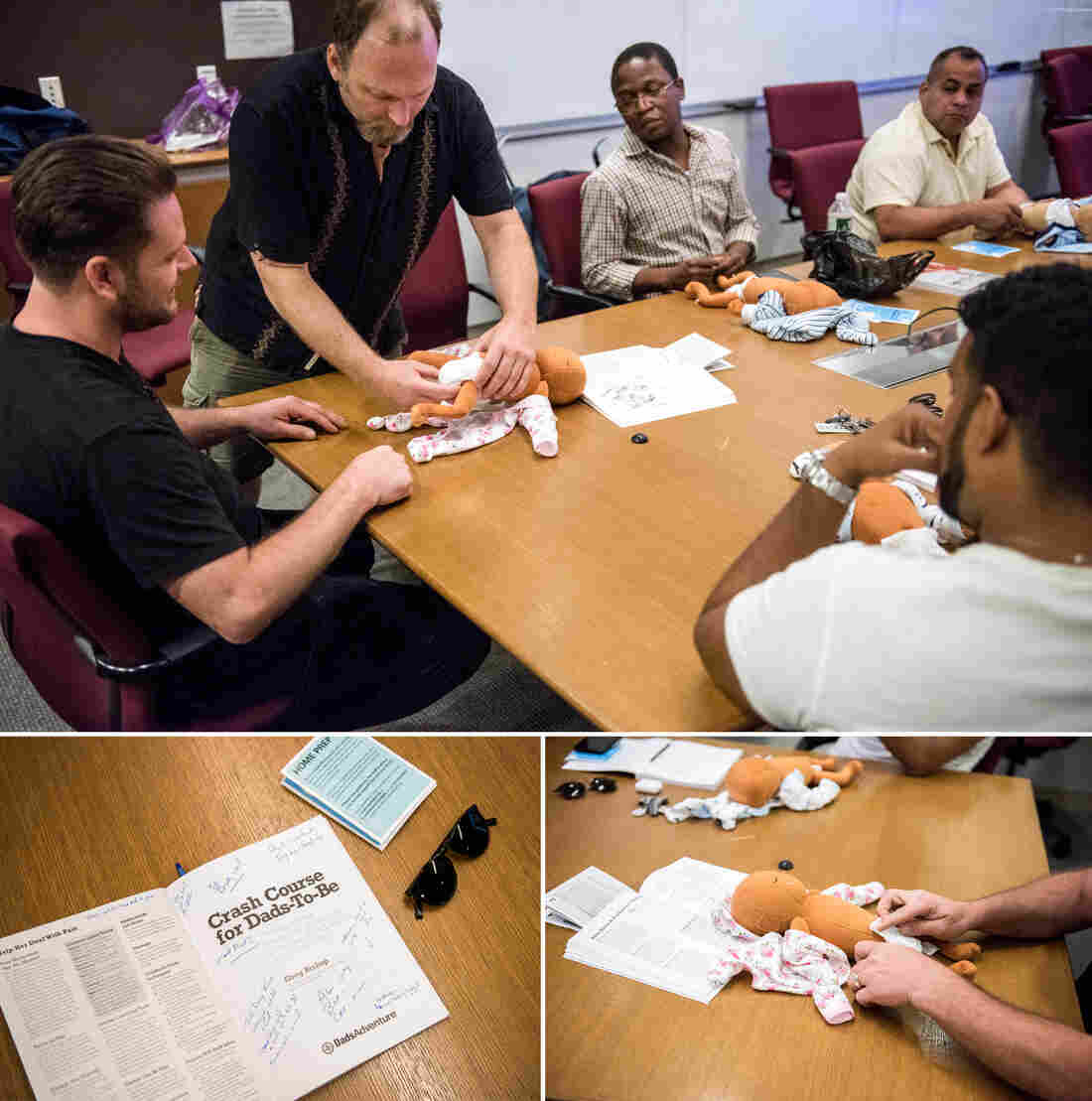
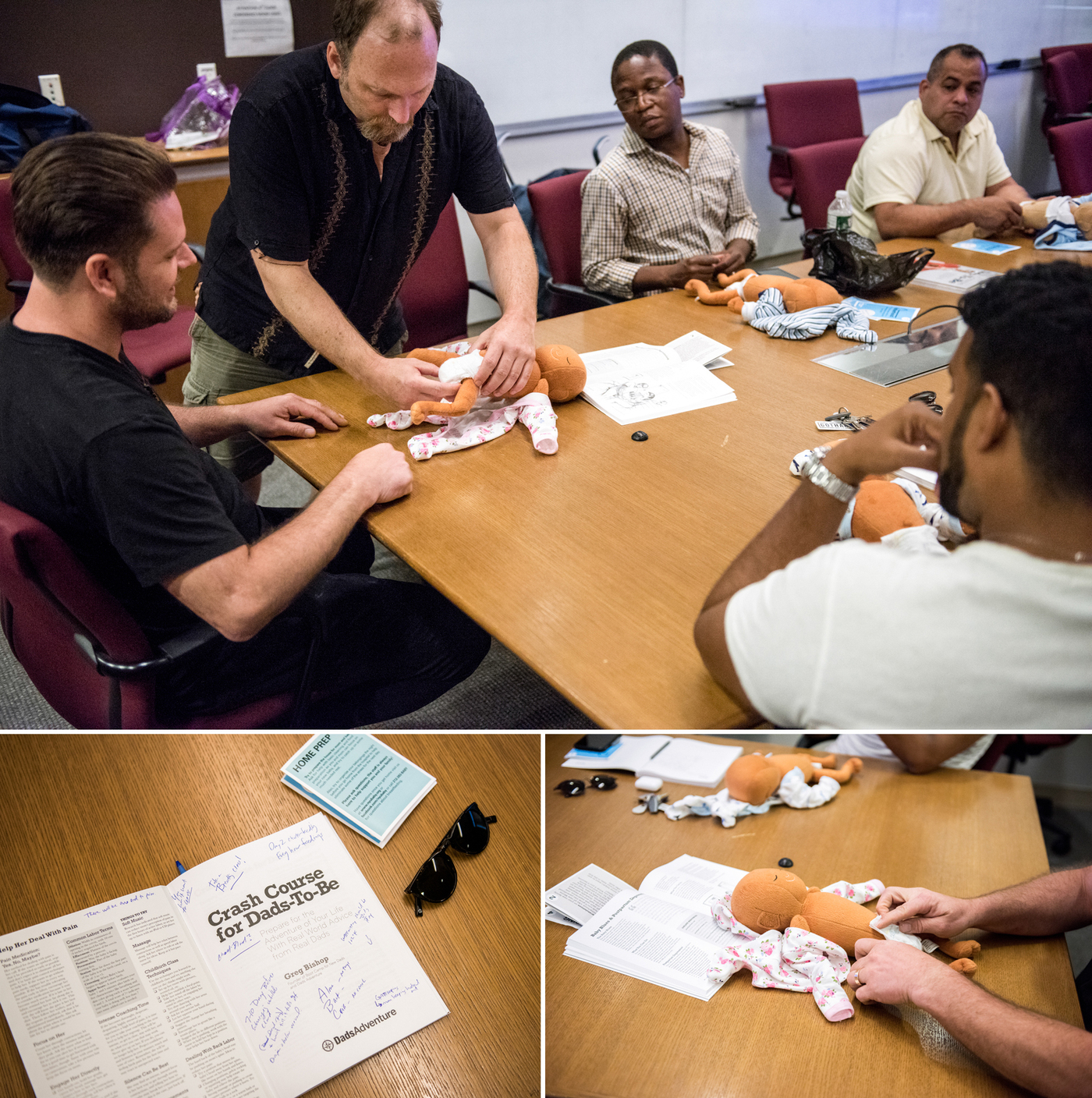
Dads-to-be learn how to change diapers in the workshop for and by men, at the New York Langone Medical Center. Participants say they appreciate the combination of concrete skills and candid advice from other fathers.
Jason LeCras for NPR
hide caption
toggle caption
Jason LeCras for NPR
“Even though fathers are far from secondary in their children’s lives, they may feel uncertain about their place in the family,” says Julian Redwood, a psychotherapist in San Francisco who counsels dads.
In fact, Garfield says, as they await their baby’s arrival, men, like women, often worry about the hands-on tasks of childcare, how to raise well-adjusted kids, and about how to cope with sleep deprivation, especially after they return to work.
Addressing those concerns early helps dads get involved with parenting from the outset, and that bolsters the whole family’s health — maybe especially the baby’s — according to research by pediatricians and child psychologists. For example, a 2017 study found that the amount of hands-on, sensitive engagement dads were observed to have with babies at age 4 months and 24 months correlated positively with the baby’s cognitive development at age 2.
Early father involvement also benefits the health of the child by fostering sturdier father-child bonds and psychological resilience, researchers say.
Oyo says the three-hour-long, Sunday Bootcamp for New Dads session he attended at NYU Langone Medical center, helped ease his early fears. At the peer-led workshop, “I learned babies communicate through crying,” he says, “and that they usually cry for four reasons — which made infant care seem less scary.”
Joe Bay, a 44-year-old father who lives in Clifton, N.J., was the session’s coach. Calling the course a “bootcamp” acknowledges the ambivalent relationship dads may feel between childcare duties and societal views of masculinity, Bay says. It also speaks to the practicality of what the men can expect to learn — how to hold a tiny baby, for example, or how to soothe a crying infant.
Participants also learn how parenthood can rock their partner’s well-being — and upend their own emotional health, as it rattles their sense of identity.
Future fathers get a chance in the course to question Bootcamp grads. Bay says he finds many fathers-to-be more willing to open up when their partners are absent. Oyo concurs.
“I met a dad who seemed like a ‘pro’ with his infant son, which was reassuring,” Oyo says. Learning from that man how to change a diaper and how to swaddle a baby, he says, helped him stay calm later, when facing his own wailing daughter. In the class he’d learned how to “read her cues.”
As the dads get more secure in their parenting skills, the moms usually become less anxious, too. And that’s crucial in making sure a behavioral tendency family scientists call “maternal gatekeeping” doesn’t derail the family system.
“Maternal gatekeeping encompasses a set of behaviors that mothers may use — consciously or unknowingly — that limit the father’s involvement with their children,” explains Anna Olsavsky, a doctoral candidate in human development and family science at The Ohio State University, and lead author of a 2019 study of how such “gatekeeping” influences a budding family.
Gatekeeping behaviors can be small but powerful: micromanaging dad’s interaction with the baby, for example, or criticizing how he holds or feeds the child.
Though fathers have always been somewhat involved in their children’s care, Olsavsky says, society still deems mothers “childcare experts.”
“That portrayal can lead dads to be socialized into supportive parenting roles” she adds — in other words, they take a step back.
In their most recent study, Olsavsky and her colleagues found that men who felt welcomed by their partners to participate in child rearing felt more connected to their partners, and were more likely to identify as equally involved and responsible co-parents.

Guests of the class Jesse Applegate (center) and his son, Jacob, field questions from Saxon Eldridge (left), and Chris De Souza (right) about what to expect after the baby’s born.
Jason LeCras for NPR
hide caption
toggle caption
Jason LeCras for NPR
Oyo, whose daughter is now nine-months-old, says the bootcamp helped him take an active lead in parenting. It was also a relief to his pregnant wife, he says, to see that he was studying up for fatherhood.
After the course,” Oyo says, “I shared everything I had learned, and once the baby was born, I became the trusted source for swaddling.”
Garfield tells prospective fathers that the art of proper swaddling, a method of wrapping babies that soothes them in the first couple of months, can be one of ‘dads secret parenting weapons.’ Additional tools include using a low voice to talk or sing to the baby, Garfield adds, or playing with the newborn during diaper changing time.
Learning these parenting techniques and the dynamics that develop when one new parent feels sidelined can be just as useful for adoptive parents and same-sex couples, Bay notes.
For all parents, raising children can feel a bit like being thrust into an ocean without knowing how to swim. But having an outlet where each caregiver can connect and learn from their peers helps make parenting less lonely. And it dismantles the myth of the ‘perfect parent.’
Greater parental harmony can help decrease spousal friction, which tends to rise when sleep deprivation and a lack of control are at an all-time high.
Reducing parental bickering pays off for the baby, too: Research suggests constant arguments can have an impact on a child’s brain development, disrupt healthy attachment, and raise a child’s risk of becoming anxious and depressed later in life.
Many mothers and fathers enter the wild ride of parenting hoping to be ‘expert parents.’ That’s a big mistake, Bay tells participants in his Bootcamp workshops.
“I always tell dads the goal isn’t to be ‘perfect,’ ” he says, “but ‘good enough.’ “
Juli Fraga is a psychologist and writer in San Francisco. You can find her on Twitter @dr_fraga.
Bianca Andreescu Snatches Historic Victory From Serena Williams, Wins 1st Grand Slam

Bianca Andreescu reacts after defeating Serena Williams in the women’s singles final of the U.S. Open.
Adam Hunger/AP
hide caption
toggle caption
Adam Hunger/AP
Canadian Bianca Andreescu beat Serena Williams (6-3, 7-5) at the U.S. Open on Saturday, becoming the first Canadian to win a Grand Slam singles title.
Her victory at Arthur Ashe Stadium — the site of Williams’ first Grand Slam win in 1999 — kept Williams from tying Australia’s Margaret Court’s all-time record of 24 Grand Slam titles.
For the 19-year-old Andreescu — born the year after Williams won her first major title at the U.S. Open — the victory capped an impressive run at this year’s tournament. She became the first Canadian to reach a Grand Slam finals. And despite setbacks from a shoulder injury, the Romanian Canadian’s play helped her rise to 15th in the Women’s Tennis Association rankings entering her match against Williams. She was ranked 208 last summer.
The match represented another difficult loss for the 37-year-old Williams since her return to tennis last year after the birth of her daughter in 2017. Since her return, she has tried unsuccessfully four times to match the record for most Grand Slam wins.
The only other match-up between Williams and Andreescu was cut short when Williams suffered a back injury in the Rogers Cup final in Toronto last month. Andreescu took home that title. Impressed by her rival’s sportsmanship after the match, Williams called Andreescu an “old soul.”
Both attribute their success to a strong mental game as much as a physical one. Andreescu has spoken about her pre-game meditation ritual.
As for Williams, she says the stress of contending with other tennis superstars might be less taxing than motherhood.
“I think being on the court is almost a little bit more relaxing than hanging out with a two-year-old that’s dragging you everywhere,” Williams told USA today after a commanding semifinals performance against Ukraine’s Elina Svitolina on Thursday. “I think that’s kind of been a little helpful.”
Barbershop: NFL’s 100th Season

To mark the NFL’s 100th anniversary, NPR’s Michel Martin talks football with The Nation’s Dave Zirin, Jason Reid of ESPN’s The Undefeated, and journalism professor Kevin Blackistone.
Saturday Sports: U.S. Open, NFL
The U.S. Open is well underway and Serena Williams is, unsurprisingly, in the finals. The NFL’s opening night was underwhelming. And more girls than ever are signed up to play high school football.
SCOTT SIMON, HOST:
How nice it is to find time for sports.
(SOUNDBITE OF MUSIC)
SIMON: Serena Williams on the verge of history again. The regular NFL season has begun with a long, dull splat. And are more young women interested in getting their heads rattled too? We’re joined now, as always, by NPR’s Tom Goldman. Tom, thanks so much for being with us.
TOM GOLDMAN, BYLINE: Thank you, Scott.
SIMON: U.S. Open – Serena Williams going for what would be a record-tying 24th Grand Slam win. But there’s a 19-year-old on the other side of the net. How do you see today’s match?
GOLDMAN: I see victory. I see the great…
SIMON: For one of the players, yes. But yes, yeah.
GOLDMAN: (Laughter) Oh, OK, for Serena Williams.
SIMON: Yeah.
GOLDMAN: I see Serena reversing recent history. You know, since her return to tennis after becoming a mother, she’s been in three Grand Slam finals and lost all three. And she has looked rattled. Each of those losses was preceded by a strong showing in the semifinal match.
Now, the U.S. Open has followed that pattern. She’s looked really good coming into this final against 19-year-old, Canadian Bianca Andreescu. So why do I see victory, Scott?
SIMON: Why do you see victory, Tom Goldman?
GOLDMAN: Thank you for asking. Because both Williams and her coach say she is finally healthy. She’s battled injuries this year. Now they say she’s physically ready, and that helps her mental approach. In her words, she says she has been way more chill than in the past. And, Scott, I believe her.
SIMON: Yeah, well, she knows. Rafael Nadal is the last of the big three standing on the men’s side. What do you see there?
GOLDMAN: Well, we’ve seen the big three teeter this tournament. Novak Djokovic pulled out with an injury. Roger Federer lost in the quarterfinals, largely because he was hurt, although he refused to blame that. You know, there’s all this speculation – is the big three reign over? I mean, someday it will be, someday soon. But Federer, the oldest of them at 38, he has been playing great, and no reason he can’t still at 39 if the body holds up. For now, though, as you say, Nadal is left. He plays in tomorrow’s final. And he has a chance to win his 19th major title, putting him one behind the leader, Federer.
SIMON: Yeah. NFL season opened – Green Bay Packers versus the Chicago Bears…
GOLDMAN: (Imitating snoring noises).
SIMON: …With their headliner Eddie Goldman, the fabulous Eddie Goldman. This is the oldest rivalry in football – all the makings of a classic, except the game. You watched all three hours. If you had to put a highlight reel together, how many seconds would be in there?
GOLDMAN: Not many. Can I get those three hours back? I don’t think I can. It was a 10-3 snore-fest, although NFL aficionados – and there are many – will say that shows my ignorance because it was a defensive masterpiece.
SIMON: Right, yes.
GOLDMAN: Well, there was a lot – there were a lot of penalties and bad offense, too. Scott, I love a great defensive play now and then, but give me touchdowns, long touchdowns.
SIMON: At least one, I think there was one. Yeah, yeah.
GOLDMAN: Lots of – lots of them. Come on, guys. And hopefully, the offenses will start waking up tomorrow.
SIMON: I want to ask you about a development in high school football, and I have divided thoughts about it. Recent numbers show that more girls, young women, than ever are participating in tackle football at the high school level. I have a hard time cheering the fact that young women athletes now stand – want an equal chance to suffer head trauma.
GOLDMAN: Yeah, well, it’s a good point. And some will agree with you. We will note this interesting development, however. The National Federation of State High School Associations says last season, more than 2,400 girls played 11-man, or shall we say 11-person, tackle football on high school boys’ teams. Now, that’s only 0.2% of the total, but it’s an increase for the fourth straight year, and this at a time when participation by boys has been declining. California leads the way with 593 girls who played. New Jersey, Texas, Colorado also had more than 100, so an interesting development.
SIMON: NPR’s Tom Goldman. Thanks so much.
GOLDMAN: You’re welcome.
Copyright © 2019 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Trump Administration Is In Court To Block Nation’s First Supervised Injection Site

Supporters of safe injection sites in Philadelphia rallied outside this week’s federal hearing. The judge’s ultimate ruling will determine if the proposed “Safehouse” facility to prevent deaths from opioid overdose would violate the federal Controlled Substances Act.
Kimberly Paynter/WHYY
hide caption
toggle caption
Kimberly Paynter/WHYY
Philadelphia could become the first U.S. city to offer opioid users a place to inject drugs under medical supervision. But lawyers for the Trump administration are trying to block the effort, citing a 1980s-era law known as “the crack house statute.”
Justice Department lawyers argued in federal court Thursday against Safehouse, the nonprofit organization that wants to open the site.
U.S. Attorney William McSwain, in a rare move, argued the case himself. He says Safehouse’s intended activities would clearly violate a portion of the federal Controlled Substances Act that makes it illegal to manage any place for the purpose of unlawfully using a controlled substance. The statute was added to the broader legislation in the mid-1980s at the height of the crack cocaine epidemic in American cities.
Safehouse argues the law does not apply because the nonprofit’s main purpose is saving lives, not providing illegal drugs. Its board members say that the “crack house statute” was not designed to be applied in the face of a public health emergency.
“Do you think that Congress would want to send volunteer nurses and doctors to prison?” asked former Philadelphia Mayor and Pennsylvania Governor Ed Rendell, who is on Safehouse’s board, after the hearing. “Do you think that’s a legitimate result of this statute? Of course not. No one could have ever contemplated that, ever!”
Safehouse earned the backing of Philadelphia’s mayor, health department, and district attorney, who announced they would support a supervised injection site in January 2018 as another tool to combat the city’s dire overdose crisis.
More than 1,100 people died of overdoses in Philadelphia in 2018 — an average of three people a day. That’s triple the city’s homicide rate.
In response, public health advocates and medical professionals teamed up with the operators of the city’s only syringe exchange to found Safehouse. They created a plan for its operations, and began scouting a location.
But the Trump Administration sued the nonprofit in February to block the supervised injection site from opening.
In June, the Justice Department filed a motion for judgment on the pleadings– essentially asking the judge to rule on the case based on the arguments that had already been submitted. Since then, a range of parties have filed amicus briefs in support of or in opposition to the site. Attorneys general, mayors, and governors from across the country filed briefs backing Safehouse, while several neighborhood associations in Kensington and the police union filed against it.
U.S. District Judge Gerald McHugh requested an evidentiary hearing to learn more about the nuts and bolts of how the facility would work, were it to open. At that hearing, in August, Safehouse’s legal team, led by Ilana H. Eisenstein, explained that Safehouse would not provide drugs, but that people could bring their own to inject while medical professionals stood by with naloxone, the overdose reversal drug. They said Safehouse would also be an opportunity for people to get access to treatment, if they were ready to commit to that.
Safehouse vice president Ronda Goldfein said the only difference between what Safehouse would do — and what’s already happening at federally sanctioned needle exchanges and the city’s emergency departments — is permit drug injection to happen in a safe, comfortable place.
“If the law allows for the provision of clean equipment, and the law allows for the provision of naloxone to save your life, does the law really not allow you to provide support in that thin sliver in between those federal[ly] permissible activities?” she said.
McSwain contends operating in that “sliver” is exactly what makes Safehouse illegal.
Much of the debate at Thursday’s hearing revolved around interpreting the word “purpose.” The statute in the Controlled Substances Act makes it illegal for anyone to “knowingly open … use or maintain any place … for the purpose of … using any controlled substance.”
The federal government says it’s simple: Safehouse’s purpose is for people to use drugs. McSwain conceded the facility will also provide access to treatment, but so does Prevention Point, the city’s only syringe exchange. Effectively, he argued, the only difference between Safehouse and what’s already going on elsewhere would be that people could inject drugs at Safehouse, which is prohibited by the statute.
“If this opens up, the whole point of it existing is for addicts to come and use drugs,” McSwain said.
Safehouse said its purpose is to keep people at risk of overdose from dying.
“I dispute the idea that we’re inviting people for drug use,” Eisenstein argued.
“We’re inviting people to stay to be proximal to medical support.”
McSwain conceded that if Safehouse were to offer the medical support without opening up a space specifically for people to use drugs, the statute would not apply.

Philadelphia Mayor Jim Kenney spoke Thursday in support of the Safehouse injection site to reduce the number of deadly overdoses in Philadelphia. More than 1,100 people died of overdoses in the city in 2018 — an average of three people a day.
Kimberly Paynter/WHYY
hide caption
toggle caption
Kimberly Paynter/WHYY
“If Safehouse pulled an emergency truck up to the park where people are shooting up, I don’t think [the statute] would reach that. If they had people come into the unit, that would be different,” he said. Mobile units and tents in parks are supervised injection models that other cities like Montreal and Vancouver have implemented.
Safehouse has also said it hasn’t ruled out the idea that it might incorporate a supervised injection site into another medical facility or community center, which would indisputably have other purposes, as well.
McSwain ultimately argued that Safehouse had come to the “steps of the wrong institution,” and that if it wanted to change the law, it should appeal to Congress. He accused Safehouse’s board of hubris, pointing to Safehouse president Jose Benitez‘s testimony at the August hearing, where he acknowledged that they hadn’t tried to open a site until now because they feared the federal government would think it was illegal and might shut it down.
“What’s changed?” asked McSwain. “Safehouse just got to the point where they thought they knew better.”
“Either that, or it’s the death toll,” Judge McHugh replied.
Supervised injection sites are used widely in Canada and Europe, and studies have shown that they can reduce overdose deaths and instances of injection-related diseases like HIV and hepatitis C. San Francisco, Seattle, New York City, Ithaca, N.Y., and Pittsburgh, Pa., among other U.S. cities, have expressed interest in opening a similar site, and are watching the Philadelphia case closely. In 2016, a nonprofit in Boston opened a room where people can go after injecting drugs, to ride out their high. The room has nurses equipped with naloxone standing by.
The Justice Department’s motion for the judge to rule on the pleadings is still pending. McHugh could decide he now has enough information to issue a ruling, or he might request more hearings, arguments or a full fledged trial.
Safehouse’s legal team said this week that if the judge rules in its favor, it might request a preliminary injunction in the form of relief — to allow the facility to open early.
“We recognize there’s a crisis here,” said Safehouse’s Goldfien. “The goal would be to open as soon as possible.”
This story is part of NPR‘s reporting partnership with WHYY and Kaiser Health News.
This story is part of NPR’s reporting partnership with WHYY and Kaiser Health News.
The Thistle & Shamrock: Debuts

Beth Malcolm
Courtesy of the artist
hide caption
toggle caption
Courtesy of the artist
Hear musicians from both sides of the Atlantic making their first appearances on our show. Artists include Beth Malcolm, a new duo for Tony McManus and a welcomed return from a band last aired in the days of vinyl.
The Thistle & Shamrock: The Lost Songs Of St. Kilda

Barrule
Phil Kneen/Courtesy of the artist
hide caption
toggle caption
Phil Kneen/Courtesy of the artist
Hear the haunting melodies from St. Kilda that offer a last link to the “island on the edge of the world,” with Julie Fowlis and Barrule.
For Health Workers Struggling With Addiction, Why Are Treatment Options Limited?

Dr. Peter Grinspoon was a practicing physician when he became addicted to opioids. When he got caught, Grinspoon wasn’t allowed access to what’s now the standard treatment for addiction — buprenorphine or methadone (in addition to counseling) — precisely because he was a doctor.
/Tony Luong for NPR
hide caption
toggle caption
/Tony Luong for NPR
Peter Grinspoon got addicted to Vicodin in medical school, and still had an opioid addiction five years into practice as a primary care physician.
Then, in February 2005, he got caught.
“In my addicted mindframe, I was writing prescriptions for a nanny who had since returned back to another country,” he says. “It didn’t take the pharmacist long to figure out that I was not a 19-year-old nanny from New Zealand.”
One day, during lunch, the state police and the DEA showed up at his medical office in Boston.
“I start going all, ‘I’m glad you’re here. How can I help you?’ ” he says. “And they’re like, ‘Doc, cut the crap. We know you’re writing bad scripts.’ “
He was fingerprinted the next day and charged with three felony counts of fraudulently obtaining a controlled substance.
He also was immediately referred to a Physician Health Program, one of the state-run specialty treatment programs developed in the 1970s by physicians to help fellow physicians beat addiction. Known to doctors as PHPs, these programs now cover other sorts of health providers, too.
The programs work with state medical licensing boards — if you follow the treatment and monitoring plan they set up for you, they’ll recommend to the board that you get your medical license back, Grinspoon explains. It’s a significant incentive.
“The PHPs basically say, ‘Do whatever we say or we won’t give you a letter that will help you get back to work,’ ” Grinspoon says. “They put a gun to your head.”
But the problem, he and other critics say, is that, for various reasons, most PHPs don’t allow medical professionals access to the same evidence-based, “gold standard” treatment that addiction specialists today recommend for most patients addicted to opioids: medication-assisted treatment.
Grinspoon was told that to avoid a criminal record he would need to spend 90-days at an inpatient center in Virginia; there, he was not allowed access to the most common MAT prescription of counseling plus buprenorphine or methadone. These drugs are particular members of the opioid family that have been shown to suppress cravings for heroin, fentanyl and other frequently abused opioids. (Another drug, naltrexone, works by blocking opioids’ action, and is also sometimes prescribed as a component of medication-assisted treatment.)
“Why would you send this Jewish atheist to a religious, Christian rehab place in Virginia?” Grinspoon says. “It didn’t make any sense. I was just sitting there listening to people recite the Lord’s Prayer and hold hands. And I’m not against the Lord’s Prayer, but it just didn’t help me.”
At the same time, Grinspoon was forced off all the drugs he’d been taking “cold turkey,” without the medical support that would have eased withdrawal pangs and cravings. “It was completely insane,” he says.
“Why on earth,” Grinspoon adds, “would you deny physicians — who are under so much stress and who have a higher access and a higher addiction rate — why would you deny them the one lifesaving treatment for this deadly disease that’s killing more people in this country every year than died in the entire Vietnam War? There’s no reason for it.”
Grinspoon eventually recovered, but only, he says, after going through several “awful” rehab experiences. “I recovered despite going to rehab not because I went to rehab,” he says.
Today, he is a licensed primary care doctor and teaches at Harvard Medical School. He has also written a book about his experience with addiction called Free Refills.
Addiction specialists call for an end to the medication ‘ban’
While there is some variation in the particular rules and policies that each state’s physician health program follows, Dr. Sarah Wakeman of Harvard and the Massachusetts General Hospital Substance Use Disorder Initiative, says most PHPs don’t refer patients to addiction programs that include medication as part of their treatment. And that’s a problem, she says.
“I think the underlying issue is stigma and a misunderstanding of the role of medication,” Wakeman says, “and this idea that a non-medication-based approach is somehow better than someone taking the medication to control their illness.”
She co-authored a recent opinion piece in the New England Journal of Medicine titled “Practicing What We Preach — Ending Physician Health Program Bans on Opioid-Agonist Therapy,” along with collaborators Leo Beletsky and Dr. Kevin Fiscella.
“Systematically denying clinicians access to effective therapy is bad medicine, bad policy and discriminatory,” they write in NEJM. “We call on the health care sector to practice what it preaches, by discarding this antiquated norm.”
“It’s the peak of hypocrisy and absurdity,” Beletsky, a professor of law at Northeastern University tells NPR.
“I work with a lot of folks who are health professionals themselves, who are on the front lines advocating and fighting against stigma, trying to get policies and practices to align more closely with the science,” he says. “If those very same people were themselves struggling with addiction they would not have access to those medications.”
The strict policies of PHPs might have a chilling effect on health professionals who have opioid use disorder and need help, Beletsky and Wakeman believe.
A proven record, and reasons for caution
So what do the institutions getting blamed here — Physician Health Programs — have to say about all this?
Dr. Christopher Bundy is the executive medical director of Washington state’s PHP and the president-elect of the Federation of State Physician Health Programs.
He wants to make clear, first of all, that there is no systematic ban against the use of medication-assisted treatment, and no health care provider should avoid seeking help.
“There are doctors today across the country who are being monitored on buprenorphine,” he says. “And not just physicians. Nurses and other health professionals — certainly nurses in our state are able to work on buprenorphine.”
Bundy acknowledges, though, that those cases are not the norm.
There are “rational and understandable reasons,” he says, why such medications are often not used in rehab programs aimed at health professionals.
For example, he cites concerns that medications like buprenorphine can affect cognition. PHPs also get pressure from other stakeholders, such as regulators and licensing boards not to use medication. And, he points out, the in-patient, non-medication treatment model has been proven to work with many health professionals across several decades, and he worries that changing it could open PHPs up to unnecessary risk.
“Our tendency is to err on the side of caution,” Bundy says, “especially when implementing therapies that have the potential to impair somebody’s ability to practice safely. Despite the fact that there are many who would like us all to believe that the jury is in [on medications like buprenorphine], more remains unknown than known, especially when it comes to how to appropriately use these medications in safety-sensitive professionals.” That includes some other professions, such as pilots, he says — not just health workers.
Bundy notes that the public trusts PHPs to help health workers get healthy enough to be able to work with patients again — and that trust is fragile.
“We only need to have a case of one physician who is on buprenorphine where there’s a bad patient outcome,” he says, “to potentially have a whole other source of criticism being levied against the PHP for putting that physician back to work on a medication that may have played a role in that bad outcome.”
An overwhelming process
Bill Kinkle, a nurse in recovery from opioid use disorder, is right now going through the laborious process of getting his nursing license back. He lives outside of Philadelphia and is very public about his past drug use — he even has a podcast called “Health Professionals in Recovery.”
He’s working through an extensive treatment and monitoring program to get his nursing license back. Kinkle hopes to complete his third year of documented sobriety next fall; if so, he’ll then be eligible to practice nursing again.
When he was in the throes of his addiction and desperate to get into recovery, Kinkle says he was scared to do anything that might jeopardize his chance to get his career back.
Independence Blue Cross Foundation
YouTube
“In the nursing community, there is a ton of fear about the PHPs,” he says. “Everybody always told me, ‘You can’t be on Suboxone [a form of buprenorphine] — you can’t be on anything.'”
But he wanted to check for himself. So he called his state’s PHP to ask what their policy actually was.
” ‘The Board of Nursing will send you for some type of extensive cognitive testing,’ ” he says he was told. ” ‘Number one, the testing is very expensive. And it’s very difficult to find someone that will do the testing that we require.’ “
Daunted by that response, Kinkle says he instead “white knuckled it.” He went to abstinence-based programs — over and over again, and over and over. Many, many times, as soon as the rehab ended, Kinkle would relapse and turn to opioids again.
“A lot of those, I overdosed,” he says. “And had my wife not found me on the floor and been able to take care of me, I very well may have died.”
Kinkle believes “all that possibly could have been mitigated, had I gotten the gold standard of treatment, which is either buprenorphine or methadone.”
He doesn’t fault PHPs or licensing boards for their problematic policies, even though he thinks those policies put his life at risk. He says the stigma associated with addiction is ingrained in our culture; there’s no single institution to blame.
Both sides of the table
Peter Grinspoon was monitored in his recovery from opioid dependence by a PHP for seven years; and then later went to work for that very program.
“I’ve seen this issue from both sides,” he says. “I actually sat at the same table — in 2005 looking like something the cat dragged in, and then from 2013 to 2015 as a physician in recovery, helping other doctors.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Grinspoon eventually wrote a book about his experiences and now works as a doctor at Mass General Hospital in Boston.
/Tony Luong for NPR
hide caption
toggle caption
/Tony Luong for NPR
Grinspoon says in his experience, there was a de facto ban on medication-assisted treatment. In his state the ban was based, he says, on the assumption that the licensing board would reject any doctor-applicant who was taking a medication like buprenorphine. He says the feeling among staff at the PHP was “why bother to set someone up for failure?”
He believes such a policy needs to change, and that any cited concerns about cognitive impairment associated with medication-assisted treatment are unproven — and hypocritical.
“Why do they make medical students, interns and residents work 28-hour shifts then?” he points out. “I’d rather have someone on Suboxone [treat me] than someone who’s been up all night. And doctors are allowed to drink the night before [they go to work] — they’re allowed to take Ambien for sleep. That totally impairs you the next day.”
“This is pure stigma,” Grinspoon says. “It’s harming doctors. They need to reevaluate this completely.”
Women’s Soccer Stars Concerned About Trauma From Repetitive Head Impact

As research into head injuries expands to include women’s soccer, some of the sport’s former stars are calling attention to the health fallout from heading the ball multiple times.