An Epidemic Is Killing Thousands Of Coal Miners. Regulators Could Have Stopped It

Greg Kelly at home in Delphia, Ky. A former coal miner, Kelly has an advanced stage of black lung disease known as complicated black lung or progressive massive fibrosis.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
Greg Kelly’s grandson, Caden, scampers to the tree-shaded creek behind his grandfather’s house to catch crawdads, as Kelly shuffles along, trying to keep up. Kelly’s small day pack holds an oxygen tank with a clear tube clipped to his nose. He has chairs spaced out on the short route so he can stop every few minutes, sit down and catch his breath, until he has enough wind and strength to start out again for the creek.
“I just pray that the Lord give me as much time as I can with him,” Kelly said, his eyes welling with tears. “He just lightens my life. I want to be as fun with him as I can. And do as much as I can with him.”
Caden is 9 years old, and even at his age he knows what happened to his paw-paw at the Harlan County, Ky., coal mines where Kelly labored as a roof bolter for 31 years.
“That coal mine made your lungs dirty, didn’t it?'” Kelly recalled Caden asking. “Yeah it did. … And I can’t breathe and I have to have my backpack to breathe,” Kelly told him.

Former coal miner Danny Smith and his family used to ride their ATVs and go camping on this reclaimed strip mining site in Pike County, Ky. But Smith is no longer able to do such things because of his advanced black lung disease.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
It’s a familiar tale across Appalachia. Two hours north and east, beyond twisting mountain roads, Danny Smith revved up a lawn mower. He wore jeans, a T-shirt and a white face mask stretching from eyes to chin, and he pushed only about 15 feet before he suddenly shut off the mower, bent to his knees and started hacking uncontrollably.
“Oh God,” he gasped, as he spit up a crusty black substance with gray streaks, and then stared at the dead lung tissue staining the grass. Still coughing and breathing hard, Smith settled into a chair on his porch and clipped an oxygen tube to his nose.
After spending just 12 years underground, his lungs are so bad he faces what coal miners decades older and with decades more in mining have endured. His lung tissue is dying so fast, his respiratory therapist says, it just peels away.
“I’m terrified,” Smith said, as he remembered his father’s suffering when he was struggling with the same coal miner’s disease.
“I sure don’t want to go through what he went through. I seen a lot of guys that died of black lung and they all suffered like that.”

Kelly says he used to wrestle with his grandson before he was diagnosed with black lung disease. Fishing is one of the few activities he is still able to do.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
A multiyear investigation by NPR and the PBS program Frontline found that Smith and Kelly are part of a tragic and recently discovered outbreak of the advanced stage of black lung disease, known as complicated black lung or progressive massive fibrosis.
A federal monitoring program reported just 99 cases of advanced black lung disease nationwide from 2011-2016. But NPR identified more than 2,000 coal miners suffering from the disease in the same time frame, and in just five Appalachian states.
And now, an NPR/Frontline analysis of federal regulatory data — decades of information recorded by dust-collection monitors placed where coal miners work — has revealed a tragic failure to recognize and respond to clear signs of danger.
For decades, government regulators had evidence of excessive and toxic mine dust exposures, the kind that can cause PMF, as they were happening. They knew that miners like Kelly and Smith were likely to become sick and die. They were urged to take specific and direct action to stop it. But they didn’t.
“We failed,” said Celeste Monforton, a former mine safety regulator in the Clinton administration who reviewed the NPR/Frontline findings.

Kelly and his wife, Lisa, say grace before Sunday dinner.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
“Had we taken action at that time, I really believe that we would not be seeing the disease we’re seeing now,” said Monforton, now a workplace safety advocate who teaches at George Washington and Texas State universities.
“Having miners die at such young ages from exposures that happened 20 years ago … I mean this is such a gross and frank example of regulatory failure.”
It’s an “epidemic” and “clearly one of the worst industrial medicine disasters that’s ever been described,” said Scott Laney, an epidemiologist at the National Institute for Occupational Safety and Health.
“We’re counting thousands of cases,” he said. “Thousands and thousands and thousands of black lung cases. Thousands of cases of the most severe form of black lung. And we’re not done counting yet.”
“They’re essentially suffocating while alive”
This advanced stage of black lung leaves lungs crusty and useless, says Dr. Robert Cohen, a pulmonologist at the University of Illinois, Chicago who has spent decades studying black lung and PMF disease.
“You have a much harder time breathing so that you can’t exercise,” Cohen noted. “Then you can’t do some simple activities. Then you can barely breathe just sitting still. And then you require oxygen. And then even the oxygen isn’t enough. And so … they’re essentially suffocating while alive.”

“There’s a lot of memories here, some good, some bad,” says Smith, while reflecting on his years working at the now defunct Solid Energy mine in Pike County.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
The toxic mine dust that causes severe disease isn’t coal dust alone. It includes silica, which is generated when miners cut sandstone as they mine coal. Many coal seams in central Appalachia are embedded in sandstone that contains quartz. And when quartz is cut by mining machines, it creates fine and barbed particles of silica dust — fine enough to be easily inhaled and sharp enough to lodge in lungs forever.
In the past 30 years, the biggest coal seams were mined out in Appalachia, leaving thinner seams coursing through sandstone.
“All the good seams were gone because there were hardly no solid seams of coal left,” the 54-year-old Kelly remembered. “And there [was] more rock in the coal.”
The silica dust that resulted from cutting that rock was far more dangerous than coal dust alone.
Silica is “somewhere around 20 times more toxic and can cause disease much more rapidly,” said Laney.
The NPR/Frontline investigation found thousands of instances in which miners were exposed — not just to coal dust but to dangerous levels of toxic silica dust. The federal Mine Safety and Health Administration’s own data chronicle 21,000 instances of excessive exposure to silica since 1986.
At the same time, NPR identified black lung diagnoses involving miners in their 30s who also experienced rapid progression to the advanced stage of PMF. Smith says he was diagnosed with PMF at 39. NIOSH has confirmed this trend in its studies.
“We’ve got the bodies to prove it”
NPR/Frontline analyzed 30 years of data collected by federal regulators. They measure coal and silica dust where miners are working, and in 85 percent of the samples collected silica was at safe levels. But for that other 15 percent — which amounts to 21,000 dust samples — the data show that miners were exposed to excessive silica levels that violated federal health standards.
“That’s what causes disease, is the excessive exposure,” said Jim Weeks, an industrial hygienist and mine dust specialist at MSHA in the Obama administration and at the United Mine Workers union before that.
An NPR review of mine dust regulations also found that federal enforcement does not directly address silica dust. If regulators measure too much silica in mine air, they place coal mines on much tougher limits for coal dust. That’s supposed to lower the silica exposure because coal and silica dust are often mixed.
But our investigation found that this indirect approach to controlling silica dust didn’t always work. MSHA’s 30 years’ dust sampling data show dangerous levels of silica or quartz where miners were working close to 9,000 times, even after coal mines were required to meet reduced limits for coal mine dust.
“They didn’t pay sufficient attention,” Weeks concludes. “And …we’ve got the bodies to prove it. I mean these guys wouldn’t be dying if people had been paying attention to quartz. It’s that simple.”

A coal processing plant sits abandoned near Smith’s home in Pike County.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
We found another example of overexposure in MSHA’s data. Each time federal mine inspectors issued citations for too much silica, which they did only a fraction of the time, they included an estimate of how many miners were affected. A review of those data shows more than 9,000 workers were exposed to silica levels that the regulations considered dangerous.
This excessive exposure to silica almost certainly happens more often than the data suggest. That’s because the data show only what happens when regulators are checking. The inspectors don’t check most of the time miners are working. Dust sampling takes place during regular mine inspections, which are scheduled four times a year in underground mines and twice a year at surface operations.
And until recently, sampling did not take place every hour miners worked or while mines were at full production.
Another finding of the NPR/Frontline investigation: During some of the heaviest periods of exposure to silica, regulations allow miners to work without any monitoring for it at all.
A white rock dust
Smith drove us past a pair of adjacent coal mines near his home in Canada, Ky., where he and other miners cut nothing but rock for months.
He was reluctant to pull over at the Rockhouse Energy Mine, even though it is closed, because security guards were watching from a parking lot. So he slowly passed by, describing work shifts that lasted 16 hours a day, seven days a week, for months, while cutting through solid rock. They used drills and mining machines to dig from one coal seam to another underground.
“It wasn’t coal dust that you would see,” Smith said. “It was more of a white rock … dust.”
Smith and his coworkers were cutting what’s called a slope mine. It’s not really mining because there’s no coal involved. It’s all about cutting through mountainsides or blocks of rock to reach coal seams.
And because there’s no coal, it is considered development mining or construction. So sampling the air for toxic dust is not required, even though it is the most dangerous dust. Former MSHA officials told us some inspectors did it, but most did not.
Smith spent months cutting at least two slope mines in his career and believes that could explain his severe disease, even though he worked underground only 12 years.

An old photograph of Kelly taken when he was 19 captures him taking a break after working in the mines.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
“Very possible,” he said, as we passed the mine’s abandoned conveyor belts that stretch over the road. “Most of my mining career I run a continuous miner. I run a roof bolter also. And it’s very possible from all the hours we worked.”
Roof bolters operate a machine that pins roof supports into underground mines by drilling into solid rock. The machines have customized dust-control systems that suck away dust, but miners complain they get bursts of silica dust when they begin drilling and then later when they empty boxes that collect the dust that was sucked away during drilling.
The machine known as a continuous miner grinds up rock and coal. Dust is supposed to be controlled by massive ventilation fans that pump air through the mine, while heavy curtains channel that air to sweep away dust. Mining machines spray water as they cut, to tamp down dust.
NPR interviewed 34 coal miners, all diagnosed with PMF and with 12 to 40 years in mining in Pennsylvania, West Virginia, Virginia and Kentucky. Sometimes the dust controls worked, most told us, and sometimes they didn’t.
Federal law requires mining companies to offer dust masks or respirators to miners, but their use is not required. The law considers them a secondary and optional means of protection. Mines are required to provide air clear of dangerous dust, first and foremost.
Most of the sick and dying miners we interviewed who used dust masks said they often didn’t work.
“They would clog up with dust, sweat and spit,” said Edward Wayne Brown, who spent 21 years underground in Buchanan County, Va. “And then it feels like somebody just sitting there with their hand over your face.”
In fact, dozens of miners, including Smith, have filed product liability lawsuits against dust mask suppliers. Most cases are still pending but a few have resulted in multimillion-dollar verdicts for the miners.
“This is probably the oldest known occupational hazard,” said retired industrial hygienist Weeks, who has a collection of antique books to prove it — with references to mine dust hazards from Pliny the Elder in the first century and another dating to the 15th century.
“There’s nothing new about this,” Weeks added. “And you’d think by now we’d have figured out how to deal with it.”
Loading…
Don’t see the graphic above? Click here
Awareness of silica dust as a hazard in the United States goes back at least 100 years, with a series of studies and reports beginning in 1908. In the 1930s, hundreds of workers were sickened and killed by exposure to silica dust while tunneling through a mountain of solid rock in West Virginia.
In 1974, NIOSH first called for silica exposure limits twice as strict as those in place for coal miners and other workers. But it wasn’t until the 1990s that MSHA and others began to get serious about silica in coal mines.
NPR and Frontline obtained internal memos from the Clinton administration that showed alarm back then about clusters of advanced lung disease among coal miners as young as 40. MSHA sent out alerts to coal mining companies, warning about excessive exposure to silica dust and severe disease among miners. NIOSH again called for a silica exposure limit that would be twice as tough, plus separate regulation of silica, as did a Department of Labor advisory committee.
“We started a national campaign first to raise awareness,” recalled Davitt McAteer, the assistant secretary of labor for mine safety and health from 1994 to 2000.
“And it was that campaign that began to try to go after the silica requirements, raise the silica standard, and start on a separate path to control silica.”
McAteer proposed a major overhaul of the dust sampling system, which included other loopholes that permitted excessive exposures and inaccurate measurement of coal mine dust. But the effort encountered stiff opposition from the National Mining Association, the industry’s biggest lobbying group. The group sued over some elements of the plan and won.
“And then we ran out of time,” McAteer says. “And it’s something that’s unfortunate and put a lot of lives at risk.”
Mine dust loopholes
The regulation of silica dust wasn’t addressed during the administration of George W. Bush. During the Obama administration, mine safety advocate Joe Main was in charge of MSHA. Main was the longtime health and safety director at the mineworkers union and was on that Labor Department advisory committee that sought tougher regulation of silica back in 1996.
“It was very obvious that that whole scheme that had been in place, that has left so many people sick, had to be changed and had to be fixed,” Main said.
He was successful in closing major mine dust loopholes, and he deployed new technology — dust sampling devices that measured coal dust in real time and helped make sampling more immediate, honest and accurate.
Main also made the exposure limit for coal mine dust tougher. But not the exposure limit for silica. He didn’t include any specific action on silica in his plan.
“A high tide rises all boats, as the saying goes,” Main explained. “We were going to get a benefit out of reducing overall dust exposure by what we did. [That] would not only lower coal mine dust but all dust that was part of that, including silica.”
But as the NPR/Frontline data analysis shows, that formula failed thousands of times in the past. Lowering overall mine dust doesn’t necessarily reduce silica exposure to safe levels.

Smith worked mostly for Sidney Coal Co. during his 12 years as an underground miner. Sidney was owned by Massey Energy, a defunct coal giant with multiple mine disasters in its history and a CEO who went to federal prison for conspiracy to violate mine safety laws.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
Monforton wonders why MSHA missed or ignored that part of the dust sampling data.
“The fact that [NPR and Frontline] went back for 30 years and looked at that data, and that data was available to the agency to assess as well, why wasn’t that problem recognized and rectified?” Monforton asked.
Main and other former MSHA officials say they thought they were doing what they needed to do to control silica.
Another agency did act on silica during the Obama administration. The Occupational Safety and Health Administration concluded a 44-year review of silica exposure by enacting tougher regulation of silica dust.
So now, every industry in the country that cuts rock, every industry except mining, has separate regulation of silica and an exposure limit twice as tough — the limit first recommended by NIOSH in 1974.
Mining companies also knew they were cutting more quartz, creating more silica dust, and exposing miners to toxic dust. They were not only clearly warned by MSHA in the 1990s; they could see what was going on in their mines. Cutting rock slows mining machines and hurts production. And rock has to be removed from coal before it can be sold.
So NPR and Frontline wanted to know why mining companies didn’t act on their own to protect their workers.
“Sure they could have done that,” responded Bruce Watzman, the National Mining Association’s top lobbyist for more than 30 years. “But … I’m not going to speculate on why they did or didn’t do what they chose.”
“Our focus here is forward looking,” he said. “How do we prevent this in the future? I can’t answer for … what happened in the past.”
Watzman also asserted that the industry “is doing far better today than we did in the past, far better.”
That assessment is based on new data from MSHA following the new coal mine dust rules that began to take effect in 2014. Since then, mining companies have met exposure limits for coal and silica dust 99 percent of the time, the data show.
MSHA cited the same data in a written statement to NPR and Frontline.
“The dust rule … has greatly reduced miners’ exposure to respirable dust,” wrote MSHA spokeswoman Amy Louviere, who also noted a sharp drop in the past 10 years in the percentage of mine dust samples with excess silica. Her statement did not address the NPR/Frontline findings showing 30 years of excessive exposure to silica.
“MSHA continues to work diligently to protect coal miners’ health,” Louviere said.
But NIOSH epidemiologist Laney isn’t convinced the problem is solved.
“They’re sampled very infrequently so we don’t know what’s going on with these miners when they’re not being sampled,” Laney said. “Ninety-nine percent of the time we don’t have information on that.”
That’s also the conclusion of a recent review by the National Academies of Sciences, Engineering and Medicine. The new coal dust rules, the review committee said, “may not guarantee that exposures will be controlled adequately or that future disease rates will decline.”
It will also take 10 years or more to know whether the new dust rules result in fewer cases of disease. It takes that long for disease to develop.
“I said I suspect silica. I didn’t say it was”
MSHA declined multiple requests for interviews with top agency officials, including David Zatezalo, a former coal company executive and industry lobbyist who now heads the agency.
So we showed up at West Virginia University in September where Zatezalo was scheduled to make a rare public appearance.
“You hear the phrase in health circles of progressive massive fibrosis, these sorts of things,” Zatezalo told an audience of mining engineering students, agency employees and industry executives and lobbyists.
“To me, I believe those are all clearly silica problems,” Zatezalo continued. “Silica is something that has to be controlled.”
But immediately after his speech, when NPR and Frontline approached him, Zatezalo seemed suddenly uncertain about silica and PMF.
“I don’t think that the science of the causation is that well-defined,” Zatezalo said.
Asked about the direct link between silica and disease he described in his speech, Zatezalo became defensive.
“No, I said I suspect silica. I didn’t say it was. … I think until such time as you figure out what it is you don’t really know,” Zatezalo responded.
So far, under Zatezalo, MSHA has no plan to address a tougher limit for silica dust or separate regulation of silica in coal mines.
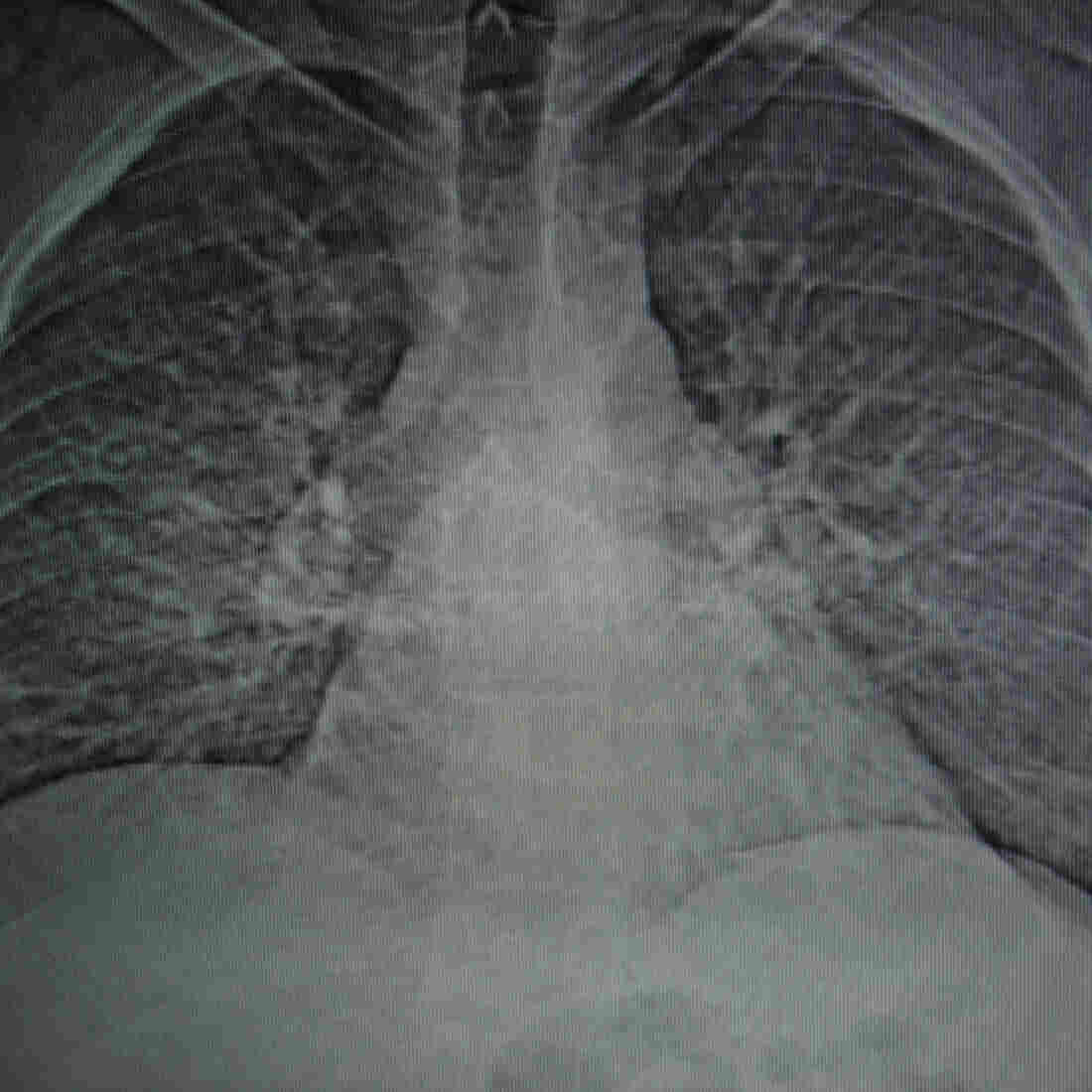
A CT scan shows the damage to Smith’s lungs caused by progressive massive fibrosis.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
In the meantime, the PMF epidemic continues. The biggest cluster of disease ever reported, according to NIOSH, continues to build at the Stone Mountain Health Services black lung clinics in Southwestern Virginia. The clinics continue to diagnose new cases at the rate of about a dozen a month.
“I’m not seeing any slowdown whatsoever,” says Ron Carson, who directed the Stone Mountain clinics for 28 years before retiring earlier this year.
“I think that America needs to know that these miners … have paid a price,” Carson added, his voice breaking. Carson cited the nation’s decades of dependence on coal for power and steel production.
“They paid a price so that we can have luxury and … so many have died. Thousands have died.”
“Every one of us is either crippled or dead”
Kelly has a long list of simple tasks he can no longer accomplish: walking up his driveway to the mailbox; climbing the few steps to his barn; riding horses; even just getting up to head to the bathroom. He has to stop and rest on the way, he says.
But what hurts the most are the things he can’t do with his grandson, Caden, especially playful wrestling on the floor.
“Now he has to wrestle a pillow while I call the match,” Kelly said, his voice halting and his eyes red. “It’s still fun, but …” and Kelly paused, his face tight and the tears flowing.
“I want to be that pillow.”

Incomplete projects are sprinkled around Kelly’s home. Kelly has a long list of simple tasks he can no longer accomplish; even just walking to the mailbox is difficult.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
Smith pulled up to another mine, which was also closed but had no guards in its weed-choked parking lot. This Solid Energy mine, along with the Rockhouse mine he drove by earlier, was operated by Massey Energy, now a defunct company with deadly mine disasters in its history and a CEO who went to prison for conspiracy to violate mine safety laws.
Smith got out and walked up to a rusted fence with a padlock. A ball cap shaded his face. Sunglasses hid his tears.
“It’s [been] eating at me for the last two years,” he said, “that I’m going to die over this. … Of all the things that could’ve killed me while I did work there, the rockfalls and all that stuff, I lived through all of that. And I find out years later I’m going to die over black lung. And it’s heartbreaking.”
Smith then mentioned his wife and two daughters and wondered what will happen to them when he’s gone. He wondered about the grandchildren he may never see. His voice breaking again, he talked about the excitement of being a young miner, about the hope and promise of good pay and good lives.
“We was all young and strong and stout and they took advantage of us. Every one of us is either crippled or dead. We was all young men,” he said, crying softly.

Smith has a plot picked out for himself in the family cemetery on his property, behind the gravestone of his parents.
Rich-Joseph Facun for NPR
hide caption
toggle caption
Rich-Joseph Facun for NPR
Back at his house in a narrow valley — a holler — in Canada, Ky., Smith pointed to a family cemetery on a knoll at the edge of the lawn he has so much difficulty mowing. It features a single gravestone with bright flowers and the names of his parents. Behind it, Smith told us, in the shade, is the burial plot he has picked out for himself. He’s 46 years old.
NPR’s Adelina Lancianese, Barbara Van Woerkom, Katie Lawrie and Cat Schuknecht; Benny Becker and Jeff Young of Ohio Valley ReSource; and Ellen Smith of Mine Safety and Health News contributed to this story.
VA Still Arbitrarily Cutting Caregivers From Program, Even As It Aims To Expand

Ret. Sgt. Christopher Kurtz and his wife Heather Kurtz pose for a portrait on the couch in their living room on Dec. 10, 2018.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
Chris Kurtz is trying to keep his sense of humor. Even after the VA told him last summer that he no longer needs a caregiver.
“Apparently my legs grew back, I dunno,” he says with a laugh, and sinks into his couch in Clarksville, Tenn. And then he mentions that he probably can’t get out of the couch without help from his wife.

Caretaker Ashlee Williams helps her husband, Former Staff Sgt. J.D. Williams, begin the process of putting on a prosethic leg.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
In December 2010, a bomb blast ended his Army deployment to Afghanistan. He lost both legs above the knee and half of his left hand. Heather, then his fiancée, joined him at Walter Reed Army Medical Center and the VA suggested she apply for their new caregiver program.
The program was set up to support family members of Iraq and Afghanistan veterans. They’re mostly wives and mothers who receive a VA stipend to provide home health care that would otherwise cost the VA millions of dollars.
When it started in 2011, vets signed up in huge numbers, quickly overwhelming the VA staff assigned to the program.
In recent years many VAs have drastically cut their rolls — often with little explanation to the caregivers.

Top, Ret. Sgt. Christopher Kurtz waits for his chair after arriving home. Bottom left, Kurtz wheels himself up to his front door as his wife and caretaker Heather Kurtz follows behind. Bottom right, Kurtz rests his hand, which is missing fingers from his injury.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
The cuts come at a time the program is supposed to be growing. Congress approved a major expansion of the program in May, though implementation could take years.
Congressional sources confirmed that the VA has missed its first deadline in October to implement new IT for the caregiver expansion — raising serious concerns of further delay. VA says the department will not deploy the new system until it is ready and has been tested thoroughly.
But VA also recently blew through a deadline to fix the IT for a new GI bill rule, and did so without initially telling Congress about the delay.

Jillyan Motter holds her younger brother Gabriel Kurtz.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
Chris and Heather Kurtz had been getting the highest level of support — Tier 3. That meant a stipend, health care for Heather and quarterly visits from a nurse. But earlier this year, Heather Kurtz was told her standing in the program was being evaluated. And without anyone from the VA even coming to see them, the Kurtzes got dropped in July.
Not reduced to a lower tier, but simply told that Chris no longer needs any help from Heather.
“He’s all better now, all better,” she said sarcastically as Chris laughed. “So he doesn’t need a caregiver for anything.”
“It was part of my identity. And then to have a letter tell me, ‘Well you’re no longer on the caregiver program,’ it hurt like a punch in the gut. Because I didn’t stop caregiving. I’ve always been a caregiver and I always will be,” she says.

The home of Ret. Sgt. Christopher Kurtz and Heather Kurtz on base at Fort Campbell.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
The Kurtzes are not alone. Just across the border near Bowling Green, Ky., Ashlee and J.D. Williams also got bad news, around Thanksgiving.
J.D., a former Army sniper, lost three limbs in a bomb attack in Kandahar. He’s fiercely independent, and he still finds ways to bow-hunt and target shoot. But he can’t do basic things like put on his prosthetic legs without help from Ashlee.
“It’s a 24/7 job,” she says. “If he wants to put his legs on he needs assistance. He wants a shower, he needs assistance. It’s not my choice. I worked full time before, at a job I enjoyed. [I had] to walk away from that.”
The Williams were demoted to Tier 1 of the program — but once their story got negative media attention, they were quickly restored to a higher tier. Still, Ashlee Williams says the way the decision was so easily changed makes her nervous.

Former Staff Sgt. J.D. Williams poses for a portrait with his wife and caretaker Ashlee Williams.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
“We’re in the clear right now — but for how long? It could be next month and they reassess us again,” she says.
An NPR report this year found that some VAs across the country have cut their rolls drastically. The VA says it’s part of standardizing the program and removing some vets who never should have qualified.
But a VA inspector general report in August found that about half the time, the VA wasn’t adequately monitoring the veteran’s health when it dropped them.
“So many caregivers are having issues,” says Williams, “and there’s no one to look at their case.”
That’s certainly true for the Tennessee Valley VA. From 510 caregivers on its rolls early last year, there are now only 104 — a drop of 80 percent.
It’s not only Tennessee. A VA spokesman said nationally the total number on the program has decreased slightly as facilities more accurately and consistently identify veterans who meet eligibility criteria for the program.

Caretaker Ashlee Williams helps her husband, Former Staff Sgt. J.D. Williams, put on one of his prosethic legs.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
But it doesn’t feel more accurate to Sherman Gillums — he’s a paralyzed former Marine who uses the VA in Washington, D.C. His wife is his caregiver.
“I was also told that in order to stay on the program, that I needed to have gotten treatment in the VA within the last year,” he says, “or else I’ll be removed from the program.”
Gillums says he had been to the VA for treatment. He thinks either the administrator who contacted him didn’t seem to have complete access to his health records, or it was something worse.
“You could take that as just informing me of the policy or it seems like a veiled threat — that’s just how I took it,” he says.
Gillums is also a senior official with one of the country’s largest veterans organizations, AMVETs. And he’s the vice chairman of the VA’s own caregiver advisory committee. He thinks there’s an effort to shrink the program.
“I characterize it this way — beginning a purge,” Gillums says.

Old wheelchairs and prosthetic legs sit in a corner of Former Staff Sgt. J.D. Williams’ home.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
He says getting the program fixed is crucial — because it’s about to grow five or six times bigger.
Congress passed a law in May, the VA Mission Act, which begins expanding the program to caregivers for veterans who served before 9/11, starting with vets from World War II, Korea and the Vietnam era.
VA Secretary Robert Wilkie told NPR last month that improvements in the program are underway.
“I think we are close to fixing that. What was the Mission Act has done [is] provided us with more resources to go out into the community and find those families that we have not been supporting, from the Vietnam era in particular,” Wilkie said.
Families like Paula and Chris Minger in Temecula, Calif. Chris suffered an abdominal wound in 1973, and complications led the VA to rate him 100 percent disabled. Paula has been taking care of him — without any VA stipend — for over 30 years. He’s in and out of the hospital, and now he’s often bedridden at home.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Former Staff Sgt. J.D. Williams practices shooting with his bow in his backyard on Dec. 11, 2018. Williams uses his love of hunting not only as therapy for himself but for other disabled combat veterans.
Erica Brechtelsbauer for NPR
hide caption
toggle caption
Erica Brechtelsbauer for NPR
“He’s probably just the most amazing guy I’ve ever known in my life. His mind is so good. He’s an avid reader. He does everything he can to make himself better,” she says.
But now he’s 68 and she’s 67, and she’d love some help, so the caregiver expansion was great news.
“I’m thrilled by it — I can’t wait,” Minger says.
She’ll have to wait, though. The timeline isn’t clear for when the expansion will start.
Bipartisan sponsors in Congress said they wanted to make sure to get the program right before rolling it out — particularly an update to the IT system. Congressional sources said it could be one to three years before Vietnam vets get in – but that hasn’t been communicated to caregivers like Paula Minger, who thought she might be able to apply this spring.
“I’m speechless,” she said upon hearing the one to three year estimate. “Think how many will die before then.”
Kentucky Attorney General Vows To Protect The Affordable Care Act

NPR’s Ailsa Chang talks with Kentucky Attorney General Andy Beshear about the court ruling out of Texas last Friday that struck down the Affordable Care Act.
What You Need To Know About The Affordable Care Act After Texas Ruling

{kind=link}
The Affordable Care Act that protects people with pre-existing conditions is at risk after a federal judge in Texas ruled it unconstitutional.
Rick Bowmer/AP
hide caption
toggle caption
Rick Bowmer/AP
The Affordable Care Act faces a new legal challenge after a federal judge in Texas ruled the law unconstitutional on Friday. The decision risks throwing the nation’s health care system into turmoil should it be upheld on appeal. But little will be different in the meantime.
“Nothing changes for now,” says Julie Rovner, chief Washington correspondent of Kaiser Health News.
“If you need to sign up for health insurance you should,” Rovner tells NPR’s Michel Martin. “If you’re in one of the several states where it’s extended where you can sign up through January, you have time to do that too.”
Below are some questions and answers about the ACA.
1. What was the Texas ruling?
U.S. District Judge Reed O’Connor ruled that the Affordable Care Act was not constitutional. O’Connor made his decision after 18 Republican state attorneys general and two GOP governors brought their case, Rovner reports. They claimed that the Supreme Court upheld the ACA in 2012 because it included an individual mandate — or a tax penalty for Americans who did not buy health insurance. After Congress repealed the individual mandate in 2017, O’Connor said the rest of the law fell apart.
2. Who might this ruling affect?
The Affordable Care Act runs for more than 1,000 pages and includes many provisions — the exchanges for individuals that are frequently political footballs — and a long list of other measures and protections designed to expand insurance coverage.
NPR’s Alison Kodjak reports that the ACA expanded Medicaid, which has allowed more than 10 million people to get coverage in states that chose to expand the program. The law also protects people with pre-existing conditions and allows people up to age 26 to be covered under their parents’ insurance; requires calorie counts at restaurants and gives protections to lactating mothers. The ACA also secured more money for Native American health care and made significant changes to allow for generic drugs and to provide funding for Medicare.
Rovner says people should act as if the ACA is still in place, but the ruling opens a possibility for “an enormous disruption.”
“It would really plunge the nation’s health care system into chaos,” Rovner says. “The federal government wouldn’t be able to pay for Medicare because all the Medicare payments have been structured because of the Affordable Care Act.”
3. What next?
Judge O’Connor did not rule the law has to be enjoined immediately. Saturday was the last day of open enrollment for the ACA in most states. NPR’s Kodjak reports people can still enroll in health plans in states with extended deadlines. She says even the newest ACA insurance policies will go into effect until more legal action plays out in courts. The federal site for insurance, Healthcare.gov, is running a banner that reads, “Court’s decision does not affect 2019 enrollment coverage.”
NPR’s Kodjak says the state of California has already said it will appeal the ruling. Other states will likely join California in the fight to preserve the law, Kodjak reports. Rovner says the case will probably reach the Supreme Court, though lower courts may reject O’Conner’s ruling first.
4. What are the political stakes in this decision?
The political stakes are great. Voters saw health care as an important issue in November’s midterm elections. Kodjak notes Congress voted multiple times in 2017 to repeal the ACA but did not succeed.
“Lots of Republicans were running ads during the midterms saying they were the ones who were going to protect people’s health care, and specifically protect people with pre-existing conditions,” Kodjak says.
The challenge to the ACA brought by Republican attorneys general is aimed at eliminating protections for pre-existing conditions, Kodjak says.
“So now you have Republicans trying to play both sides, which is going to be difficult,” she says.
News Brief: Trump's Personnel Changes, Obamacare, Weinstein Case
The White House makes more personnel moves as a government shutdown looms. A federal judge’s ruling threatens Obamacare. The latest in the sexual harassment case against movie mogul Harvey Weinstein.
What Now? Judge Rules Affordable Care Act Is Unconstitutional
Steve Inskeep talks to Ezekiel Emanuel, an architect of Obamacare, about a federal district judge’s ruling Friday that the law is unconstitutional because of a recent change in federal tax law.
STEVE INSKEEP, HOST:
Here is the reasoning behind a federal judge’s ruling against the Affordable Care Act. Obamacare includes a mandate to buy health insurance. There used to be a tax penalty if you didn’t. Courts found that legal because Congress has the power to tax. But last year’s tax bill eliminated the penalty. Now the judge in Texas says there’s no authority for the mandate. Therefore, the entire law must go. What does that mean? Well, Zeke Emanuel is in our studios again. He worked on the Affordable Care Act under President Obama. Welcome back.
EZEKIEL EMANUEL: Good to be here.
INSKEEP: Is the law in serious danger?
EMANUEL: I don’t think so. It’s a kind of silly ruling. Even conservative legal scholars think it’s a silly ruling. The mandate had, as you mentioned, no teeth because there was no tax penalty. And so it turns out it’s not essential to the law. And if it’s not essential to the law, you can’t invalidate the whole Affordable Care Act just because the mandate might not be operative anymore.
INSKEEP: Although the judge is saying in his ruling, that may make sense, but I’ve got to go on the actual wording of the law. And the law is not severable, as they say. And this part doesn’t work. Therefore, none of it works.
EMANUEL: Well, that was true maybe in the 2010 version but not the post-December 2017, when the tax law changed the Affordable Care Act. One of the things I like to emphasize, certainly, to my students at the University of Pennsylvania is the ACA is over 900 pages long. The coverage sections are 225 pages. And those covered sections include not just the exchanges where the mandate is important but Medicaid. So it’s a small part of the law. There’s many other things in the law where the mandate has no effect, like changes to how we pay doctors, changes to try to incentivize – improve quality, penalties to hospitals that have too many hospital-acquired infections and other problems. Those things have nothing to do with the mandate. So the judge here is just way overstepping in his decision.
INSKEEP: So you are not worried at all that this would be upheld on appeal?
EMANUEL: I lost no sleep last night or on Friday night.
INSKEEP: (Laughter) OK, that’s fine. Let me ask about the law itself because we have just gotten through the end of open enrollment. Is this law working, in your judgment?
EMANUEL: Oh, it’s working hugely and better than anyone thought. I mean, we saw last week that health care inflation was down at 3.2 percent in the country, which is remarkably low. You also see that the law is actually popular. The insurance companies came out against this judge. The hospitals came out against this judge. The American Medical Association came out against this judge. The ACA is the framework for health care going forward. It’s incentivizing more efficiency. It’s actually led to lower costs for the last seven years. So it’s actually working pretty well.
INSKEEP: I want to ask about costs because you alluded to health care inflation being down, some lower costs being down. It is true that in 2018 – we’ve reported this – some people are paying lower health insurance premiums than they would’ve been – a few percentage points down. Yet we have also noted that is after huge increases the several years before. Health insurance costs are still really, really high, aren’t they?
EMANUEL: Oh, yes. They are very high. A family of four getting employer-sponsored insurance is over $19,000 – way high. But the growth rate, as we like to say, has actually come down. And that come-down, that decline in the growth rate has a lot to do with the fact that the Affordable Care Act changed how people think about health care. We’re now thinking more in the health care system about eliminating unnecessary care, reducing inefficiencies in the system. And we see that in the numbers. Actually, the utilization of services is going down because doctors are not ordering as many unnecessary tests. The big problem now is prices, high prices in the health care field – you know, $2,500 for an MRI and things like that.
INSKEEP: And there are still a lot of incentives built into the system for doctors and hospitals to just charge for things and see if they get paid.
EMANUEL: Right. And also drugs. Drugs are a big portion of those price differences. And that’s where you’re going to see focus over the next five years – in bringing those prices down and the exorbitant prices in many areas down. And I think private insurance companies are going to do that. You’re going to see some action on that on the part of Medicare. And I think that’s probably going to bring health care costs down. I’ve predicted a long period of relatively low health care inflation. And I do think we’re getting there.
INSKEEP: Zeke Emanuel, thanks for coming by. Always a pleasure talking with you.
EMANUEL: It’s my pleasure to be at NPR.
INSKEEP: He served under President Obama, worked on the Affordable Care Act.
Copyright © 2018 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by Verb8tm, Inc., an NPR contractor, and produced using a proprietary transcription process developed with NPR. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
Medical Detectives: The Last Hope For Families Coping With Rare Diseases

{kind=link}
Seven-year-old Carson Miller (left), and his brother, 5-year-old Chase Miller (right), both have a degenerative brain disease called MEPAN syndrome. There are only 13 people in the world who have it.
Courtesy of Andrew Ross-Perry
hide caption
toggle caption
Courtesy of Andrew Ross-Perry
All over the country, specialized teams of doctors are giving hope to families who are desperately searching for a diagnosis.
The medical sleuths, scattered across 12 clinics nationwide, form the Undiagnosed Disease Network. Since the program began in 2014, they’ve identified 31 previously unknown syndromes and they’ve cracked more than a third of their cases, according to a recent paper in the New England Journal of Medicine.
“It was like Sherlock Holmes,” says Euan Ashley, a professor of medicine at Stanford University.” Patients would come with mystery diseases and we would try to solve them.”
Although rare diseases are individually very uncommon, collectively they are surprisingly pervasive. In fact, if grouped together into a single category, they afflict between 25 to 30 million Americans.
For people coping with mystery conditions, finally getting a diagnosis can be life-saving or life-changing. Take the perplexing case of the two Miller boys from Marin County.
A Four-Year Diagnostic Odyssey
Five-year-old Chase and 7-year-old Carson have alert minds and radiant smiles but very uncooperative bodies. The blond, blue-eyed brothers are not able to sit, stand, speak, or feed themselves. They’ve spent their lives in wheelchairs.
Even though they attend a mainstream elementary school and are cognitively functioning on par with their peers, they are both still in diapers. The boys require constant care at home and attentive individual aides in the classroom.

When Carson was about a year old, he was misdiagnosed with cerebral palsy.
Courtesy of Andrew Ross-Perry
hide caption
toggle caption
Courtesy of Andrew Ross-Perry
The boy’s parents, Nikki and Danny Miller, first noticed a problem seven years ago when their first son wasn’t reaching typical milestones like rolling over or crawling. Instead, they witnessed spastic movements and tiny hands repeatedly balling into fists. Babbling never turned into words.
When Carson was about a year old, he was misdiagnosed with cerebral palsy. Then when the same developmental delays emerged in the Millers’ second-born, the parents started asking more questions, which led to a four-year diagnostic odyssey with countless inconclusive lab tests. One after another, specialists shrugged their shoulders.
“It’s really tough because as a parent you blame yourself,” says Danny. “What did I do wrong? Is there something wrong with my genes?”
Cracking the Case
Finally, two years ago Danny applied to the clinic at the Stanford Center for Undiagnosed Diseases. After reviewing the boys’ medical history, researchers ordered full genome sequencing for all four family members. Until recently this type of extensive testing was prohibitively expensive.
“We’re rapidly moving to the point where it makes more sense to go straight to the genome rather than measuring one gene, then another, then another,” says Ashley as he pulls out his laptop to point out the clue within the family’s genetics.
The screen is divided into several rows and columns with long strings of letters that represent the human DNA code. Ashley points to a section in the MECR gene, which, when disrupted, alters the part of the brain that controls movement.
“You can see in the colored section the same gene was hit by by two variants one from mom and one from dad,” he says. There is an incorrect letter in the boys’ genetic code. “One letter of 6 billion can cause these incredibly devastating diseases,” Ashley says.

Chase Miller plays at the park with his mom and older brother.
Courtesy of Andrew Ross-Perry
hide caption
toggle caption
Courtesy of Andrew Ross-Perry
Neither of the boys’ two copies of the gene works properly, which is why Carson and Chase have a brain disease called MEPAN syndrome. Only 13 people in the world are currently known to have it, and there is only one published scientific paper on it, says Ashley.
“Currently, there is no treatment for MEPAN, but Danny and Nikki are hoping a heavy cocktail of vitamins and supplements will slow down the disease from progressing and further limiting the boy’s ability to move. The parents also take the boys to physical, occupational, and speech therapy to strengthen their muscles and teach them life skills. The boys communicate with computers attached to their wheelchairs.
Discovering what was wrong was only a single step on the family’s journey, though a crucial one. A diagnosis is key to refining treatment and potentially attracting more scientific interest, which may someday lead to a cure.
Father Danny Miller’s voice cracks as he contemplates the road ahead.
“Recently at school Carson built a sentence that said, ‘I hate my wheelchair,’ ” recalls Danny. “Because I know that he wants to be up running around, playing tag, and hide and seek with the other kids. That may not be the way things work out. But I’m going to do everything in my power to try and make sure that does happen.”
'Bleed Out' Shows How Medical Errors Can Have Life-Changing Consequences

{kind=link}
In Bleed Out, filmmaker and comedian Steve Burrows documents the 10-year odyssey of trying to figure out what went wrong when his mom went in for a hip replacement surgery and came out with brain damage and mobility issues after a weeks-long coma.
Noam Galai/Getty Images for HBO
hide caption
toggle caption
Noam Galai/Getty Images for HBO
In 2009, Steve Burrows’ mom, Judie, went in for hip replacement surgery. She came out with brain damage and mobility issues after a weeks-long coma that would change her and her family’s life.
In the new HBO documentary Bleed Out — Burrows, a filmmaker and comedian, tracks his 10-year odyssey to find out what happened to his mother and who is to blame. It’s a deep dark dive into the heart of America’s health care system.
What happened to Judie is complicated, but it essentially began with massive blood loss.
“In the end, that’s really how this whole thing started,” Burrows says in an interview with NPR’s Lulu Garcia-Navarro. “She lost over half the blood in her body.”
After her surgery, she was put into recovery and left alone with that’s called an electronic intensive care unit, or eICU.
With a series of monitoring tools that usually include microphones, video cameras and alarms, eICUs are meant to provide the 24-hour monitoring that many patients require after a major medical emergency.
“This [eICU] didn’t notice my mom was in a coma for at least a day and a half and I wanted to talk to the ICU doctor who was there that night,” Burrows says. “We were told there was no doctor there. I said ‘Well that’s insane, what do you mean?’ “
He says there were doctors monitoring the cameras out by the airport in Milwaukee and they were supposed to be the safety net for his mother.
Burrows says that when he asked whether the camera was on, the head of the ICU told him it wasn’t because of patient privacy issues.
As Burrows dug into his mother’s case and the failure of the eICU to recognize her coma, he came across a staggering statistic. According to a study by researchers at Johns Hopkins University, the third leading cause of death in the United States is medical errors.
YouTube
And those errors, Burrows says, can leave patients one step away from financial ruin.
“That’s the hard lesson we learned,” Burrows says. “My mom, certainly. She was a single mom, she raised my sister and I. She did everything right. She was set. And this happened and two and half years later, she’s broke. She’s on Medicaid … and now we, all the American taxpayers, are paying for her.”
Burrows says that before her surgery, Judie was a vibrant, independent and adventurous woman. These days, her health care has become increasingly more complicated, and in the past two months, she has started long-term hospice care.
“She is very compromised,” Burrows says. “She lost her speech several years ago and that was really the thing that really hurt her the most because she was so articulate and so full of life. I know that the loss of her speech is really the thing that is really killing her the most.”
Throughout the 10 years that Burrows documented his mother’s struggles, he recorded many conversations — both openly and secretly. One of those conversations was with the doctor who conducted his mom’s hip replacement surgery. At the time, the doctor didn’t know he was being recorded.
Steve: If you were in my shoes, right now, what would be …
Doctor: I’d like an accounting, just like you, for why in the hell no doctor was there. Their intensive care unit, where this problem occurred, we still don’t know what happened. We don’t have accountability.
Steve: I mean, do you think they’ll ever tell the truth?
Doctor: No. I don’t.
Up until this point, Burrows had been asking basic questions to the doctors and caregivers involved in his mom’s situation and their stories were always changing, he says. When he finally heard what he thought was the truth by the doctor, Burrows says it was shocking.
He started filming his mother’s pain and suffering after consulting with attorneys about trying to pursue justice for her. She was at her most vulnerable. It was painful and uncomfortable, but he knew he had to do it.
At the time, he didn’t want to make a documentary, but he eventually decided others needed to know what happened.
“When I started to find out about this universal thing, about the third leading cause of death, and then the eICUs, I thought I really have to tell people about what I just found out,” Burrows says. “Because I’m a pretty informed guy and I didn’t know about any of this stuff.”
Although he’s done his best to make sure his mother is comfortable, Burrows says he hasn’t been able to give her what she really wanted, which was to get her life back.
“I had a great mom and I really tried hard to give her everything she wanted and I couldn’t give her any of that,” he says. “She wanted to go home. She wanted to drive. She wanted her life back.”
Burrows says he hopes that as people watch the film, they realize they need to ask thoughtful questions when it comes to their health care, and he stressed the importance of having a patient advocate in case things like this happen.
“You need to shop for doctors and hospitals like you’d shop for a car,” he says. “You know, shop like your life depends on it because we found out that it does.”
NPR’s Sarah Handel and Cindy Johnston produced and edited the audio for the story. Wynne Davis adapted it for Web.
Affordable Care Act Court Challenge
A federal judge in Texas struck down the entire ACA on Friday, but the law will stay in place pending appeals. NPR’s Michel Martin talks with Julie Rovner of Kaiser Health News about the implications.
Federal Judge Issues Ruling Declaring The Affordable Care Act Unconstitutional
A federal judge in Texas issued a ruling Friday declaring the Affordable Care Act unconstitutional, apparently setting the stage for another hearing on the health care law by the U.S. Supreme Court.