
Tim Green, former NFL player and a former NPR commentator, has ALS, also known as Lou Gehrig’s disease. Green believes football gave him the disease.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
Tim Green first noticed the symptoms about five years ago.
The former NFL player, whose strength was a job requirement, suddenly found his hands weren’t strong enough to use a nail clipper. His words didn’t come out as fast as he was thinking them.
“I’m a strange guy,” Tim says. “I get something in my head and I can just run with it. I was really afraid I had ALS. But there was enough doubt that I said ‘alright, I don’t. Let’s not talk about it. Let’s not do anything.'”
Denying pain and injury had been a survival strategy in football.
“I was well trained in that verse,” he says.
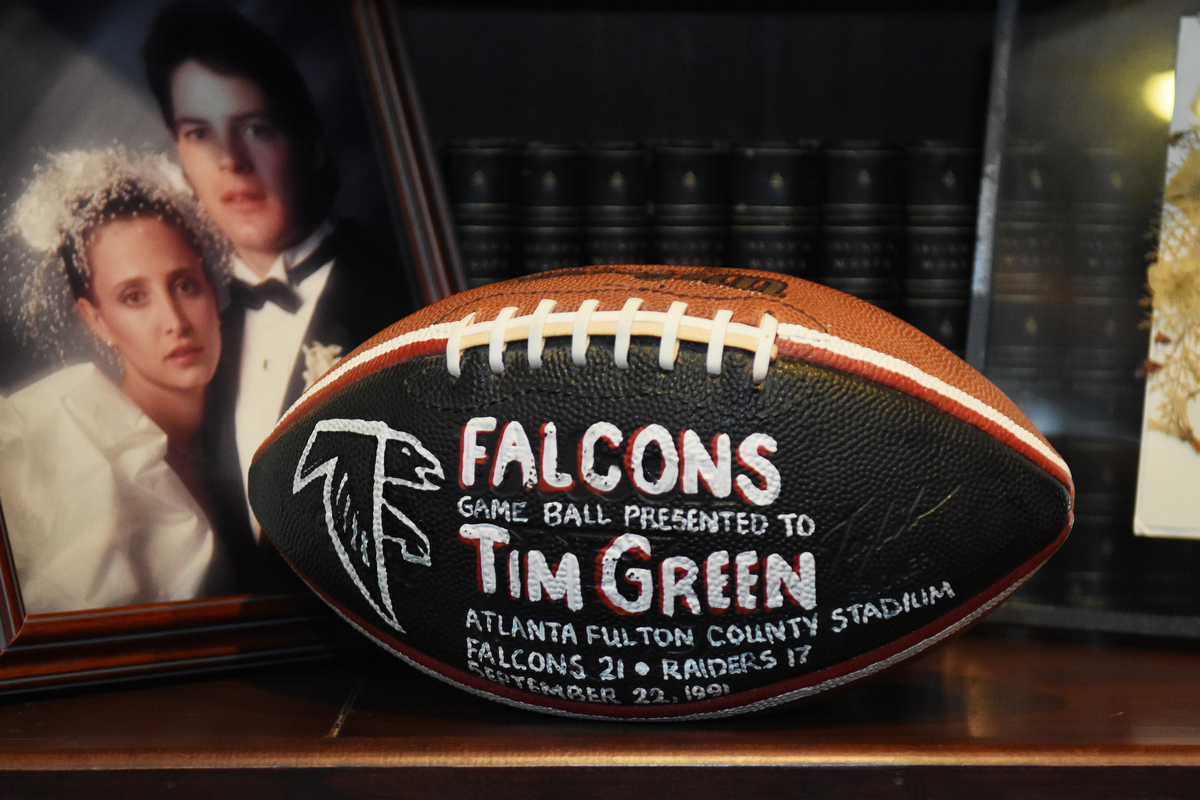
A Falcons game ball that was presented to Green in 1991.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
But a diagnosis in 2016 made denial impossible. Doctors confirmed that Tim, also a former NPR commentator, had ALS, known as Lou Gehrig’s disease. The degenerative illness attacks the body’s motor nerve cells, weakening muscles in the arms and legs, and the muscles that control speech, swallowing and breathing.
Tim tried to keep it private — he didn’t want people feeling sorry for him.
But he says, “I got to a point where I couldn’t hide it anymore.”
So Tim went on 60 Minutes and revealed his illness.
“What we said is, you either write your own history or someone’s going to write it for you,” says 24-year-old Troy Green.
When one isn’t enough
I was one of Tim Green’s producers for his Morning Edition commentaries back in the 1990s. We went to dinner once when he was in Washington, D.C. for a game — his Atlanta Falcons were playing Washington. Tim had a huge plate of pasta and when we finished, the waiter came over and asked “anything else?” Tim pointed to his clean plate and said, “yeah. Let’s do it again.”
That was him. One entrée wasn’t enough. One high-profile career wasn’t enough – he’s also a prolific author, has a law degree and works for two firms.
And ultimately, it wasn’t enough for Tim to deal with ALS in silence. Last month, in conjunction with his 60 Minutes appearance, Tim helped launch a fund-raising website, Tackle ALS.
Writing his own story
I recently visited Tim at his lakeside home in upstate New York, in the village of Skaneateles.
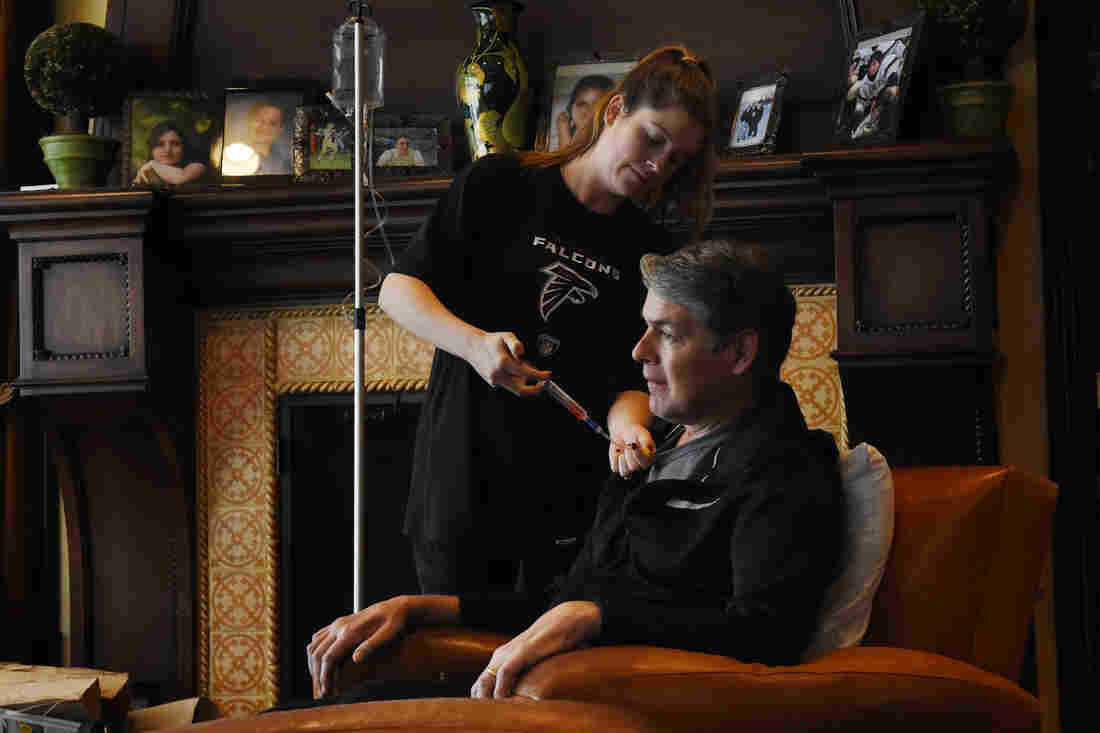
We sat down in a room with a huge picture window that normally offers a gorgeous view of Skaneateles Lake. On the day I visited, all you could see was driving snow. Troy Green sat next to his dad — Tim’s speech is slow and raspy and sometimes Troy helps repeat or reinforce Tim’s words. During our talk, a tube connected to a port in Tim’s chest provided an infusion of Radicava. Last year, the FDA approved the new drug, which has been shown to slow the progress of what’s currently a fatal disease.
Green’s daughter-in-law, Jessica Green, gives him an infusion of Radicava. Last year, the FDA approved the new drug, which has been shown to slow the progress of what’s currently a fatal disease.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
The history Troy encouraged Tim to write is positive and hopeful. They stress that ALS can be cured, it’s just underfunded.
The history certainly includes family. Tim and his wife Illyssa have been married for 29 years. They have five kids — all with first names starting with “T” — that’s Illyssa’s doing, Tim says. And the family is incredibly close. Literally.
“My brother lives on the same lane as us. I’m their neighbor,” Troy says, adding, “my little sister’s at school, my little brother lives here and then my older sister lives the furthest away. She’s about a three minute drive.”
“We’re going to reel her in,” Tim laughs.
Football, a complicated love
Of course, any Tim Green history has to include football.
For better and worse.
Tim believes football gave him the disease. His eight years in the NFL in the 1980s and 90s, as a defensive lineman and linebacker, were before protective rule changes and concussion protocols.
There were “countless” head collisions, Tim says. I mention that he had decades of those collisions, from an early age through the NFL.
“But in the NFL,” he says, “the violence and the impacts are extraordinary. Every day.”
Troy adds, “when [Tim] played, practices were worse than the games. Because in the game, you typically would see 45 to 65 plays. In practice, you could run 100, 200 by the time you’re done with drills.”
Researchers say repetitive head blows may play a part in causing ALS. The recent NFL Concussion Settlement acknowledged a link by including payouts to former players with the disease, including Tim.
His Morning Edition commentaries regularly took listeners inside the violent game. In 1992, Tim wrote one about about a teammate, former Atlanta defensive end Rick Bryan, who’d had enough of the physical toll and was retiring.
The piece ended with this:
“Back at the locker room, I checked my protective neck padding and pumped some extra air into the padding of my helmet. Like a gypsy gazing into a crystal ball, I looked at my own distorted reflection in the glossy black surface of my helmet. The smile let me know I was glad to be there, but there was nothing I could see that told me how long it would last.”
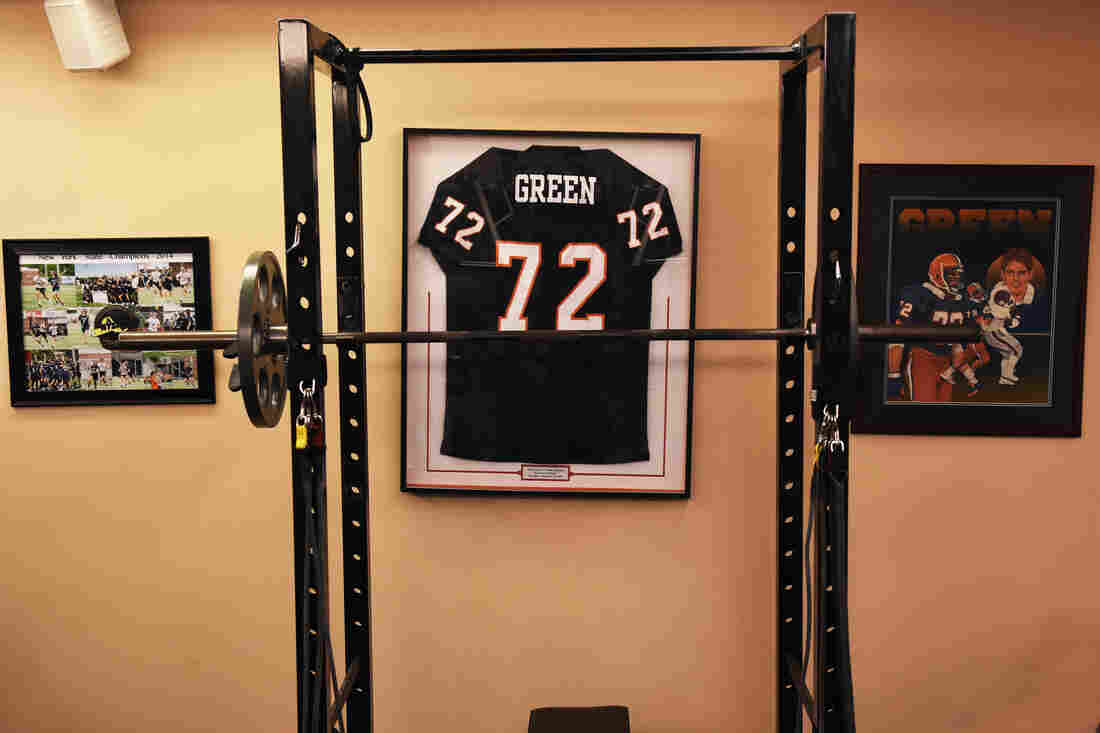
Old uniforms and posters adorn the walls at Green’s home gym.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
Tim could articulate what many players couldn’t. Why, I asked him, with his insights, would he play a sport that had the potential to do permanent damage?
Tim says as a kid, he had two passions. Writing and football. From the earliest age, he says, he worked incredibly hard to succeed at both, and he did.
“I was just impassioned,” he says. “That’s what I wanted, and that’s what I got.”
“If [this disease] is part of the bargain, I don’t know,” he continues. But back then, he says, he had “no idea” of the potential long-term damage of football. “So the temporary pain and discomfort, I knew that was worth it. Some pain in the future with my back, neck, knees, I knew that was worth it.”
“Can I say getting ALS was worth it? I don’t know. I don’t know.”
His ambivalence illustrates Tim’s profound and complicated love for the game. Still. He says it gave him the disease. But it also taught him so many life lessons growing up. It allowed him to vent anger and violence in an acceptable way.
“I’m not indicting football or the NFL,” he says.
He passed on his love – his two oldest sons played football. His 12-year-old, Ty, plays now. And it has split the close-knit Greens. Illyssa doesn’t like it. Tim says he wants Ty to play if he wants to.
Troy Green helps his father on the computer. Tim can’t type, so he has a sensor on his glasses that highlights letters. Then he clicks a mouse with his right hand, and the letters show up on his laptop screen.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
Tim and Troy say the game now is different than it was. It’s much safer with less contact in practice. Both of them coached Ty’s junior team.
“We trained [so in] every tackling drill your head’s out of the play,” says Troy. “In practice we would penalize our players if they had their head in the drill. We really just encouraged the modern day football, not the 1980’s edition.”
Still, football is inherently dangerous, and so far Ty wants to play.
“I don’t want to wrap him up in a bubble,” says Tim, “because where do you stop?”
But there’s a deeper, more complex reason behind Tim’s support. Troy says his dad doesn’t want the illness to be a burden on anyone. So Tim doesn’t want Ty not to play, just because the game hurt him.
Translating science into treatment
“I do want to point out that most people who play football don’t develop ALS.”
So says Dr. Merit Cudkowicz, who treats Tim’s disease. Cudkowicz has researched ALS for nearly 25 years. She thinks football probably is a factor that led to his illness, but not the only one. The studies so far haven’t established a direct cause and effect.
“And that’s why we think there’s something else,” Cudkowicz says. “It’s a combination perhaps in someone’s immune system or something in their genetics that makes it more likely that if you also hit your head repetitively that you might come down with the disease.”
Green works out at his home gym. Studies of ALS patients suggest people who do stretching and toning function much better. There’s a concern if a patient does too much and tries to bulk up, he or she could tear the muscles. Green’s doctor advises more low weight, repetition, toning types of exercise.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
Cudkowicz directs the Healey Center for ALS at Massachusetts General Hospital in Boston. She says Tim’s and other prominent people’s involvement and publicity present a great opportunity, as a follow up to the viral ice bucket challenges that raised money for ALS a few years ago.
“Absolutely I think this is a huge next step,” Cudkowicz says. “The ice bucket challenge came at the right time. The science was exploding but there were no resources for it. And suddenly there’s this $220 million resource for ALS and it fed this great science and drew in all these new people and new companies for the field.”
“But there’s still a [funding] gap in getting that great science to patients. And that’s where Tim’s Tackle ALS initiative and the Healey Center are going to partner and hopefully with many other groups, translate that great science into treatment for people.”
“If you have a good life, it’s never long enough”
Later, on the day I visited, Tim sat down at a desk in a large wood-paneled den, indulging his other passion in life — writing.
He can’t type, so he has a sensor on his glasses that highlights letters. Then he clicks a mouse and the letters show up on his laptop screen. He’s working on a kid’s baseball book. It’s a third collaboration with former New York Yankees star Derek Jeter and Tim says they both provide specific areas of expertise. Jeter brings baseball realism to the book; Tim draws on his many years of being surrounded by young people. Disgusting young people, he laughs.
Green writes by clicking this mouse after a sensor on his eyeglasses has located letters. He clicks one letter at a time.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
“These are kids 10 to 14 years old. Tweens,” he says. “They think vomit is funny. [So] somebody has to throw up [in the book], and it’s best when they throw up on someone.”
“Writing [these scenes] is easy. It’s convincing Derek to keep them is where I earn my money.”
On cue, Troy looks up from his phone and makes an announcement.
“Just got an email that Jeter, and [his] Turn 2 Foundation donated $10,000 [to Tackle ALS]. His ears are ringing,” Troy says, laughing. “He heard about the vomit scenes!”
Tim says the fundraising is a chance to help others. He says he’s one of the lucky people with the disease. It’s relatively slow moving.
Green hugs his 12-year-old son, Ty. Green coaches Ty in football and insists his son is playing a much safer game than his father did in the 1980s and 90s. Still, Green and his wife disagree about Ty’s participation. Illyssa Green doesn’t want her son playing; Tim supports it as long as Ty wants to play.
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
I ask Tim what keeps him positive through this time. He answers by recounting a period 12 years ago, when Illyssa was diagnosed with cancer.
“She was out of her mind,” Tim says, “and I remember saying to her, you’ve got great doctors, we’re gonna beat this and do everything we can. But in the meantime, I don’t want you to wallow in fear and anxiety and misery. I said, because we have a very good life and if you have a good life … and a lot of people do, maybe they don’t realize it, but they do… but if you have a good life, it’s never long enough. We all know it’s finite.”
“So whenever the end point is, I ask to be strong enough to maintain that positive attitude no matter what the challenges are.”
Today, Illyssa is cancer free. And it’s Tim trying to live by his own advice.
As I leave, I stop to look at two large sculptures outside their house. One is of five kids, playing. The other is a lone figure. A helmeted football player, running and catching a pass over the shoulder. Tim says it’s an homage to the game, that let him “buy this amazing property and build a comfortable home.”
A home, and family, that now mean even more than they have all along.
A statue of a helmeted football player, running and catching a pass over the shoulder. Tim says it’s an homage to the game, that let him “buy this amazing property and build a comfortable home.”
Heather Ainsworth for NPR
hide caption
toggle caption
Heather Ainsworth for NPR
Let’s block ads! (Why?)




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}