Immigrants Who Staff Home Health Care In the U.S. Worry About Deportation

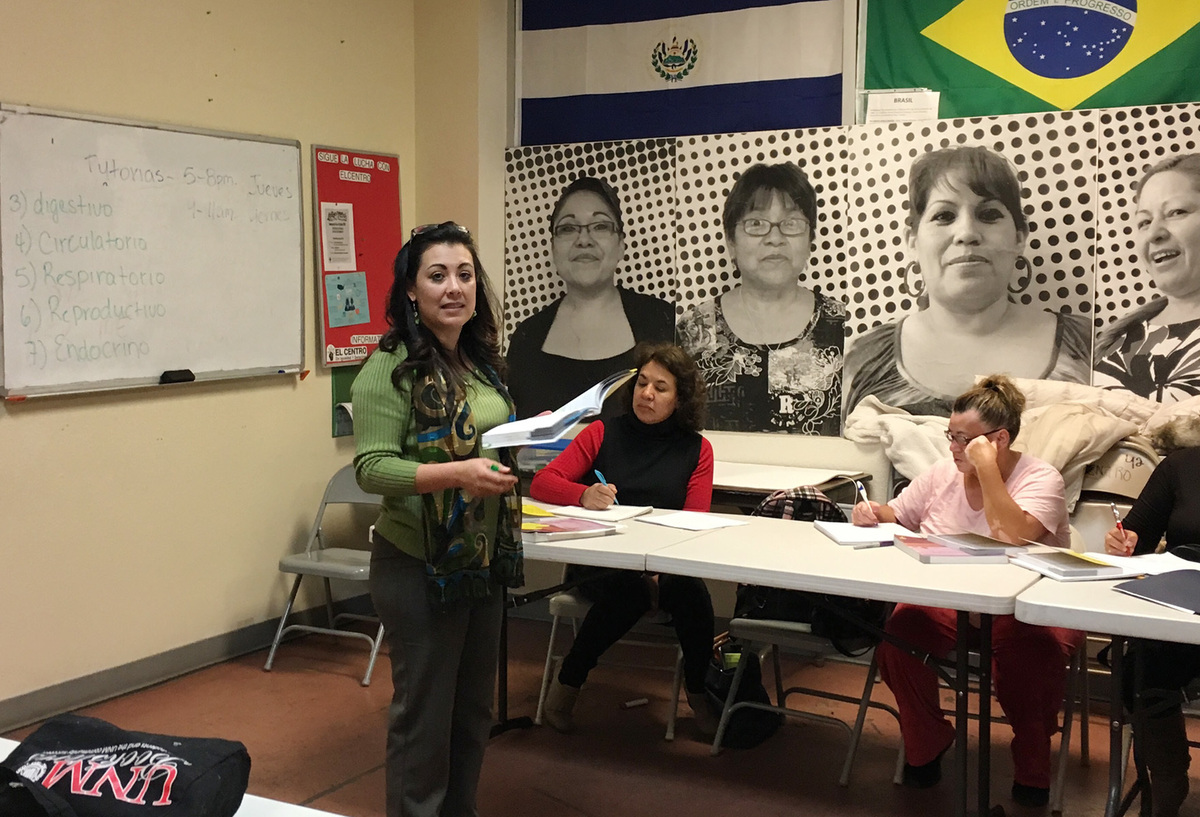
Liliana Reyes instructs a home health aide class on human biology at Encuentro, an immigrant education center in Albuquerque. State-certified graduates of the program help elderly and disabled clients with activities like bathing, dressing, and taking medication on time.
Ina Jaffe/NPR
hide caption
toggle caption
Ina Jaffe/NPR
On a rare rainy night in Albuquerque, two dozen students are learning the proper way to care for older people. Teacher Liliana Reyes is reviewing the systems of the body — circulatory, respiratory and so on — to prepare them for an upcoming exam.
These students are seeking to join a workforce of about 3 million people who help older adults remain in their homes. They assist these clients with things like bathing, dressing, and taking medication on time.
About a quarter of these workers are immigrants. But as Congress and the White House consider changes to immigration policy, some people in the home care industry worry that there won’t be enough people to care for the nation’s growing number of elders.
What makes the Albuquerque class unusual is that it’s taught entirely in Spanish. All of the students are immigrants, mostly from Mexico. The course is a joint project of Central New Mexico Community College and a community education center for immigrants called Encuentro. Everyone who passes the course becomes a state-certified home health aide.
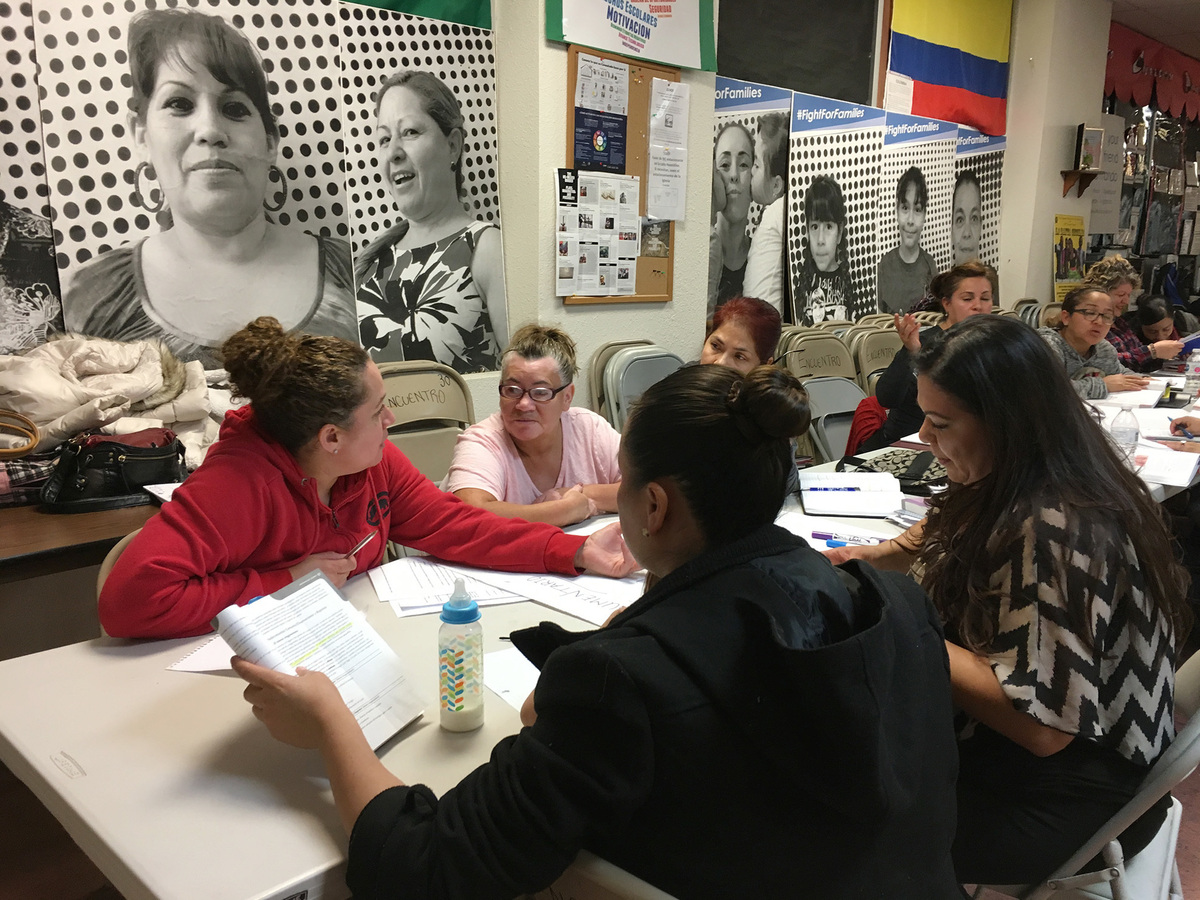
But some of these students already care for older adults, even though they’ve lacked training. Zoila Gutierrez says the first job she had in this field paid $6 an hour for a shift that lasted from 7 at night to 7 in the morning.
“This course is going to open a lot of doors for me in terms of being able to get better work,” she says. “But most importantly, I want to know about all the rules that I must follow to provide good care.”

Zoila Gutierrez (left) is a student in the Encuentro home health aide class in Albequerque. Though her youngest daughter is a citizen and two older kids are registered under DACA, Gutierrez doesn’t have papers, and knows she may have to leave her job and return to Mexico.
Ina Jaffe/NPR
hide caption
toggle caption
Ina Jaffe/NPR
Gutierrez has a complicated life. She’s 42 years old and came to Albuquerque from Mexico in 2004. She doesn’t have papers. Her youngest child is a citizen. Her two older kids are both registered under DACA, the Deferred Action for Childhood Arrivals policy. So, at the same time she’s studying to improve her prospects in the United States, she and her children also discuss the possibility of going back to Mexico.
“We must have a Plan B,” she says. “We don’t want to give up our dreams, but we must think in the ‘What if?’ So, no, we don’t want to leave. But it’s an option.”
WhileGutierrez worries about the Trump administration’s crackdown on illegal immigration, others working in home care worry about the administration’s proposals for restricting legal immigrants.
President Trump wants to focus on highly skilled, well-educated workers. But the policy change that would hurt the home care industry the most would be limiting family reunification, sometimes called chain migration. That’s according to Robyn Stone, the Senior Vice President for research at Leading Age, which represents the nonprofit side of long-term care.
“This immigrant population primarily came to the United States through family reunification,” says Stone. “If we shift in our policy [on] immigration, the pipeline for this workforce could be substantially affected.”
That’s not just a theoretical concern for Sherwin Sheik. He’s the founder and CEO of a company called CARELINX, which he describes as a cross between Uber and Match.com for connecting home care workers with clients.
“It takes a very special person to want to do these jobs,” Sheik says. “They tend to be immigrants. If we have tighter policies, it’s going to impact the industry, without a doubt.”
The nation’s rapidly aging population has made personal care assistants and home health aides (who have more specialized training around health issues) the fastest growing low-skilled occupations in the U.S.
But Steven Camerota isn’t worried about a shortage in home care workers. He’s the director of research at the Center for Immigration Studies, which advocates for restrictions on immigration. He points out that, despite the growing immigrant workforce, three quarters of the people currently providing home care were born in the U.S.
There’s no mystery to what it would take to increase that percentage, says Camerota. “Raise wages. Treat workers better.”
Home care workers sometimes make as little as $10 an hour. At the same time, he says, “we have an enormous supply of less-educated [American citizens] currently not working who could easily fill these jobs if employers treat them reasonably well.”
But this work isn’t just a matter of money for Zoila Guttierrez. She finds meaning in taking care of older people.
“I like to care for them and make sure they’re doing well — that they’re OK,” she says.
It will take at least a million more people who feel the same way to meet the needs of older adults over the next decade, whether those workers are immigrants or American-born.
Time Running Short For Congress To Stabilize Individual Insurance Market

Sen. Patty Murray, D-Wash., the ranking member, and Sen. Lamar Alexander, R-Tenn., chairman of the Senate Health, Education, Labor, and Pensions Committee, meet before the start of a hearing on Capitol Hill in Washington, Wednesday, Oct. 18, 2017, the morning after they reached a deal to resume federal payments to health insurers that President Donald Trump had halted.
J. Scott Applewhite/AP
hide caption
toggle caption
J. Scott Applewhite/AP
A bipartisan group of senators and House members has been working since last summer toward measures to keep prices from rising out of control and undermining the individual market—the market that serves people who don’t get insurance through work or through the government. Members hope to attach a package of fixes to what should be the year’s final temporary spending bill, due late this month.
The lawmakers are up against both a legislative clock and the insurance companies’ timeline. Insurers have until summer to decide if they want to continue to sell policies on the ACA marketplaces, but many start making preliminary decisions as early as April. Without action, insurers say premiums will go up in 2019 due to the uncertainty. Consumers and the government would share those costs.
It is by no means clear whether any package could gain the votes needed in the House and Senate. Most Republicans are loath to be seen “fixing” Obamacare, although opinion polls clearly show they will be blamed for problems with the law going forward.
Pressure to improve the situation is being felt beyond Capitol Hill. Last week five governors (three Democrats, one Republican and one Independent) released a blueprint for a health system overhaul that includes several of the stabilization ideas under consideration in Congress.
Lawmakers in D.C. are looking at two primary fixes, although they could be combined.
Reinsurance
One, pushed by Sens. Susan Collins (R-Maine) and Bill Nelson (D-Fla.), is called reinsurance. This is a fund that would help insurers pay for the sickest patients and would guarantee the insurance companies do not face large losses. The idea is that if insurers don’t have to worry about covering the expenses for their highest-cost patients, they can keep premiums lower for everyone.
The ACA had a temporary reinsurance program from 2014 to 2016. It was intended to help insurers get started in a market where sick people were able to buy their own insurance for the first time. Prior to the law, most insurers did not cover many people with preexisting health conditions. If they did, it was at an extremely high cost.
Since the federal program ended, several states, including Minnesota and Alaska, have adopted, with some success, their own reinsurance programs in an attempt to hold premiums down.
The subsidy fix
The other proposal, negotiated by Sens. Lamar Alexander (R-Tenn.) and Patty Murray (D-Wash.), would guarantee insurers would get money that the Trump administration cut off in October. The senators are advocating reinstating federal reimbursement for so-called cost-sharing reduction subsidies—discounts that the ACA requires insurers to provide to their lower-income enrollees to help reduce their deductibles and other out-of-pocket costs.
Senate Majority Leader Mitch McConnell (R-Ky.) pledged to Collins, in exchange for her vote on the GOP tax plan in December, that he would support bringing both bills to the floor for debate.
That has not happened. Although, in a statement, Collins said she is “continuing to have productive discussions” with Senate and House leaders about both bills.
Meanwhile, a lot has changed, including new questions about whether the fixes would work.
Would the fixes help?
State insurance regulators managed to find a workaround for Trump’s sudden cancellation of the federal cost-sharing payments.
The cancellation made some premiums higher but the subsidies the federal government gave to consumers also increased to cover those higher prices. That’s because most states allowed insurers to offset the loss of these funds by attaching the premium increases to the plans that determine how much in subsidies enrollees get to pay those premiums. The result is that most people who get government help pay the same (or, in some cases, less), while insurers are effectively being paid back.
That means, however, if the cost-sharing reduction payments were reinstated for 2018, as the original legislation called for, insurers would have to give the excess money back to the government.
Analysts agree that would only add to the confusion.
Restoring the federal payments for this year, says Joseph Antos of the conservative American Enterprise Institute, “does not lower premiums this year, so it does absolutely no good to the average person.”
Some advocates have suggested that Congress should guarantee the payments for 2019 and 2020. But Antos says that “also makes no sense because the insurers would then think ‘Are we going to go through this again?’ ” They might raise premiums even further to make up for the uncertainty.
Antos — and many other analysts — agree that instead, restoring or creating a new reinsurance program would likely do more to control premium increases.
Reinsurance “will protect premiums for the people who are actually most subject to them,” says Sherry Glied, a former Obama administration health official now at New York University. She was referring to those in the individual market who do not get government help and have been footing large premium increases for the past several years. That’s because having protection against the largest bills would allow insurers to lower premiums across the board.
Potential partisan roadblocks
Then there are the political considerations.
Many Republicans in Congress have called the cost-sharing reduction payments, in particular, a “bailout” to the insurance industry and are resistant to reinstate the payments.
Instead, they seem more amenable to the idea of reinsurance, because they consider it a type of “high-risk pool,” which they have been pushing for years. House Speaker Paul Ryan said at an event in Wisconsin in January that “I think there might be a bipartisan opportunity there to get risk pools, risk mechanisms.”
But Republicans have made clear they want something in return for what could be considered a “fix” to the health law they despise.
Health and Human Services Secretary Alex Azar was careful to say in a meeting with reporters last week that the Trump administration has no formal position yet on the stabilization efforts. But, he said, “I think it would need to be part of an entire set of reforms there that we would want to see.” That would likely include more flexibility for states to opt out of some of the health law’s coverage requirements.
The delay has made Democrats more demanding, too. The repeal of the ACA’s penalties next year for people who don’t have insurance has changed the situation dramatically, says Sen. Murray.
“As I have made clear, the bipartisan bill I originally agreed on with Chairman Alexander will not make up for this latest round of Republican health care sabotage,” she said in a statement. “In fact, there are changes that now need to be made to our bill to ensure it meets its intended goals of keeping premiums down and stabilizing markets.”
What’s at stake
But while Congress decides if it will take action, insurers are warning that doing nothing will lead to still higher premiums.
Premium rates for a “benchmark” silver plan could rise by 27 percent in 2019, the Blue Cross Blue Shield Association said earlier this month.
Congressional action on reinsurance and cost-sharing, the association predicted, would help push premium rates 17 percent below this year’s levels.
“Health plans are looking for certainty in the market,” said Justine Handelman, senior vice president in the association’s policy arm.
Ideally, Congress would include the funding in measures adopted this month, said Handelman, who spoke with reporters during a briefing at the association’s Washington, D.C., headquarters: “Most plans are filing premium rates by April.”
Kaiser Health Newsis a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
KHN senior correspondent Julie Appleby contributed to this story.
Senators Push For Leadership At Indian Health Service

Sens. Jon Tester, left, and Steve Daines, speaking together in Jardine, Mont., in August 2017. Both said recently they want the Indian Health Service to have new, strong leadership soon.
Matthew Brown/AP Photo/Matthew Brown
hide caption
toggle caption
Matthew Brown/AP Photo/Matthew Brown
The insurance broker President Trump nominated to lead the Indian Health Service, Robert Weaver, is firing back at the White House and the media after his nomination was withdrawn last week.
“The allegations raised against me in the media are baseless, irrelevant, and in the most important cases simply incorrect,” Weaver said in a press release Tuesday.
In January, The Wall Street Journalquoted a former colleagues of Weaver alleging that he had exaggerated his prior work experience.
More recently, there were reports that he voluntarily withdrew his nomination to head the IHS. But Weaver said in a letter to tribal leaders and supporters published Feb. 22 that the characterization was inaccurate.
“Regardless of what the press reports may say, I was forced out,” Weaver wrote. “I was involuntarily withdrawn.”
In his letter he said he “received a call giving me two minutes this past Friday afternoon at 4:30pm, on a three day holiday weekend, to decide to withdraw or face the public humiliation of having the White House withdraw my nomination, as demanded by a staff person from HHS.”
Weaver hasn’t replied to an interview request from NPR.
The Trump administration hasn’t named a new nominee to lead IHS, which has been without a permanent leader since 2015.
Democrats and Republicans on the Senate Committee on Indian Affairs are both urging the White House to name a new nominee quickly.
“I’m expecting better, and I hope the administration will send us a highly qualified candidate,” said Montana Republican Sen. Steve Daines. He said he didn’t get a favorable impression of Weaver when they met after he was nominated.
Sen. Jon Tester, a Democrat from Montana who is also on the Indian Affairs Committee, said Senate “due diligence” revealed problems with Weaver’s statements about his education and work history.
But Tester said he doesn’t fault the Trump administration for sending them a candidate who was not properly vetted.
“I think this can happen,” Tester said. “What I think is really important moving forward is that they get us somebody much sooner than later. So we can get them confirmed. … If they dilly-dally on this, and this position’s left open it’s a major problem for Indian Health Service and not good for our Native American folks that are depending upon Indian Health Service for their health care.”
An estimated 3.7 million American Indians and Alaska Natives eligible to receive care from the IHS. In treaties, Tribes were promised health care in return for giving up nearly all of their ancestral lands to the federal government.
This month the National Indian Health Board told Congress that the current IHS budget of $4.8 billion dollars will meet less than 47 percent of the need for Native American health care nationwide. But that group of tribal leaders says that bigger picture, the agency needs far more funding. A report it published last year says the real health care needs in Indian Country require a $32 billion infusion the IHS, phased in over 12 years.
Daines isn’t convinced money is the problem, and wouldn’t commit to whether he thinks IHS can function properly on its current budget. “Throwing more money at it isn’t going to solve the fundamental problem of lack of accountability and lack of leadership,” he said.
“You need to prioritize and look at where we spend the money,” Daines said. “One of the areas we need to address is to insure that the compensation structure for the health professionals that serve, the folks that are right there on the front line, delivering health care in Indian Country, that the wages they’re provided are competitive, so that we can attract and retain good health care professionals. That is an area that needs to be addressed, and that’s what we need to prioritize.”
For his part, Tester said, “It’s well documented that IHS has been underfunded now for decades, and you can’t get blood out of a turnip, you can’t get health care out of an agency that doesn’t have enough money to be able to do the job that they’re required to do.
“Congress also needs to do its job and make sure IHS has the dollars it needs, no more, no less, to do the job that’s required, and that’s to take care of the Indian people,” he said.
This story is part of a reporting partnership with NPR, Montana Public Radio and Kaiser Health News.
Planned Parenthood Plans Major Political Effort In Key States For 2018 Midterms

Supporters of Planned Parenthood dressed as characters from The Handmaid’s Tale protest last June outside the Capitol against Senate Republicans’ health care bill.
AFP Contributor/AFP/Getty Images
hide caption
toggle caption
AFP Contributor/AFP/Getty Images
Add Planned Parenthood to the list of organizations looking to take advantage of President Trump’s low approval ratings in the 2018 midterm elections.
The organization is not new to the rough-and-tumble of electoral politics — and has often itself become a top issue for Republicans looking to slash federal funding for the organization — but this year Planned Parenthood Votes and Planned Parenthood Action Fund will launch their biggest-ever push to try to tip the balance in Congress and in key states.
Planned Parenthood sees the Trump administration as a threat and, with a Republican-controlled Congress, sees the danger to abortion rights as great as it has been in decades. But the upside for progressive groups is that Trump has also inspired a newly energized movement in protest of his policies. The best example of this so far is the massive Women’s March on Washington, D.C., a year ago, a day after Trump’s inauguration, and the hundreds of smaller marches across the country on that day and since.
Deirdre Schifeling, executive director of Planned Parenthood Votes, which along with Planned Parenthood Action Fund constitutes Planned Parenthood’s political operation, says the group has committed an initial investment of $20 million to be used mostly on Senate and gubernatorial contests in eight states.
“We will be supporting candidates who support reproductive rights,” Schifeling says, adding that such rights are “really at stake in the country, especially this year.” She says “we support candidates who support access to Planned Parenthood and who support women and all people making their own health care decisions without interference from politicians.”
Federal funding for Planned Parenthood — which is not an actual line item in the budget, but rather reimbursement for health care services provided to patients — has become a perpetual political battle in Washington. Republicans in Congress have long made ending any federal dollars for the organization a campaign issue. But so far, the funding survives.
Planned Parenthood’s target list of states includes Michigan, Ohio, Pennsylvania and Wisconsin, all of which were instrumental in Trump’s 2016 victory. The others where Planned Parenthood will pour in money and resources are Arizona, Florida, Minnesota and Nevada — each of which has hotly contested races.
Notably, states so far not on the Planned Parenthood target list are two of the more conservative states, each of which has an incumbent Democratic senator on the ballot this year: Missouri and North Dakota. Both are states Trump won easily and where protecting abortion rights is a more difficult case to make with a more conservative populace.
This year’s Planned Parenthood spending will mostly fund a network of grass-roots volunteers to reach out to voters where health care and the right to an abortion are considered important. That likely means a focus on suburbs and female voters. Schifeling says there will be a “robust door-to-door canvassing operation,” but she adds that “we will also be investing in paid digital and some paid TV [advertising] in key races.”
Voter turnout will be the key. The money being committed this year is already $5 million greater than the $15 million Planned Parenthood spent on the 2014 midterm elections.
Meanwhile, groups that oppose abortion rights are also expected to be active in many of the same states. The Susan B. Anthony List is one such organization. It has not released a dollar amount for its 2018 political operations, but it too will fund an aggressive door-to-door campaign in key states including Ohio, Florida and Missouri. Part of the argument these groups will use is that Trump has been their friend, that he named a solid conservative, Justice Neil Gorsuch, to the Supreme Court and that such gains need to be protected.
For Planned Parenthood, a lesson of 2017 — when voter discontent over the Trump presidency helped fuel a swing of 16 seats in the Virginia House of Delegates from Republicans to Democrats and a near Democratic takeover — is that there are opportunities.
WH Opioid Commission Member Weighs In On Progress Made In Addressing Crisis

At the beginning of November, the six-member White House opioid commission delivered 56 recommendations to President Trump, for reigning in the nation’s opioid crisis. On Thursday, the White House hosted a summit on opioids. Commission member Bertha Madras speaks with NPR’s Ari Shapiro about the progress she sees happening, or not, toward those 56 recommendations.
States Seek More Federal Funding For Opioid Treatment, Not More Promises

Colorado State Rep. Brittany Pettersen (right) is advocating for more treatment money for opioid addiction, in part because of the substance abuse struggles of her mother, Stacy (left).
Nathaniel Minor/CPR News
hide caption
toggle caption
Nathaniel Minor/CPR News
Opioids are on the White House agenda Thursday — President Trump plans to talk with members of his administration about the crisis. Meanwhile, all around the United States, state legislators, treatment providers, families and many others will be listening.
The administration’s other opioid efforts have, so far, yielded no new money. Congress authorized funds in its recent budget deal— but those dollars aren’t flowing yet, and states say they are struggling.
The Oklahoma agency in charge of substance abuse has been told by the state’s legislature to cut more than $2 million from this fiscal year’s budget. And that has the providers of opioid addiction treatment on edge.
“Treatment dollars are scarce,” says Randy Tate, president of the Oklahoma Behavioral Health Association, which represents addiction treatment providers.
It’s like dominoes, Tate says. When you cut funding for treatment, other safety net programs feel the strain.
“Any cuts to our overall contract,” he says, “really diminish our ability to provide the case management necessary to advocate for homes, food, shelter, clothing, primary health care and all the other things that someone needs to really be successful at tackling their addiction.”
In just three years, Oklahoma’s agency in charge of funding opioid treatment has seen more than $27 million dollars chipped away from its budget — thanks to legislative gridlock, slashed state taxes and a drop in oil prices (with the additional loss in state tax revenue that resulted).
Jeff Dismukes, a spokesman for Oklahoma’s Department of Mental Health and Substance Abuse Services, says the already lean agency has few cost-cutting options left.
“We always cut first to administration,” he says, “but there’s a point where you just can’t cut anymore.”
The agency may end up putting off payments to treatment providers until July — the next fiscal year. Tate says that could be devastating.
“Very thinly financed, small rural providers are probably at risk of going out of business entirely — up to and including rural hospitals,” he says.
Getting treatment providers to open up shop in rural areas is really hard, even in good times, and more financial uncertainty could make that problem worse. In the meantime, according to an Oklahoma state commission’s opioid report,just 10 percent of Oklahomans who need addiction treatment are getting it.
That statistic is similar in Colorado. And as 2018 began, Colorado’s escalating opioid crisis got worse, when the state’s largest drug and alcohol treatment provider, Arapahoe House, shut its doors.

Autumn Haggard-Wolfe, now in recovery and shown here with her son Dustin, is a Denver resident and former Arapahoe House patient. She worries Arapahoe’s closing will have dire consequences, especially for people who need inpatient care, as she did.
John Daley/CPR News
hide caption
toggle caption
John Daley/CPR News
The facility provided recovery treatment to 5,000 people a year. Denise Vincioni, who directs another treatment center, the Denver Recovery Group, says other facilities have scrambled to pick up the patients.
Most of Arapahoe’s clients were on Medicaid. Autumn Haggard-Wolfe, a two-time Arapahoe House client who is now in recovery, worries the facility’s closing will have dire consequences, especially for people who need inpatient care, as she did.
“I feel like the only other option right now in therapy would be jail for people,” she says, “and people die in there from withdrawing.”
Arapahoe House’s CEO blamed its closure on the high cost of care and poor government reimbursement for services.
The mother of Colorado state lawmaker Brittany Pettersen struggled with addiction, and was treated at Arapahoe House. Pettersen says treatment centers rely on a crazy quilt of funding sources and are chronically underfunded — often leaving people with no treatment options.
“We have a huge gap in Colorado,” Pettersen says, “and that was before Arapahoe House closed.”
She is pushing legislation in the state to increase funding for treatment. But to get tens of millions of dollars in federal matching funds, Colorado lawmakers need to approve at least $34 million a year in new state spending.
That price tag may simply be too high for some lawmakers. But either way, she adds, “It’s going to take a lot to climb out of where we are.”
Colorado did get new federal funds to fight the opioid crisis through the 21st Century Cures Act, passed in December of 2016, but it was just $7.8 million a year for two years — divvied up among a long list of programs.
This story is part of NPR’s reporting partnership with StateImpact Oklahoma, Colorado Public Radio and Kaiser Health News.
Rethinking Rural Health Solutions To Save Patients And Communities

Getting health care to rural areas may involve tough decisions about the role of hospitals.
hmproudlove/Getty Images
hide caption
toggle caption
hmproudlove/Getty Images
Heidi Schultz grew up traveling from one end of South Dakota to the other, tagging along as her sister saw doctors and specialists in the “big cities” to treat her diabetes.
Schultz thought she knew rural America well when she took a position as a rural health care program officer for the Helmsley Charitable Trust in Wyoming and Montana.
But even she has been surprised by how she can drive hours on country highways seeing few cars and just “a handful of gravel driveways going somewhere you can’t see.”
“It’s almost scary,” Schultz says. “You’re thinking, ‘If something happened to me here on this road now, how long would it take for someone to get to me? An ambulance? And where would they take me for care?’ “
Now part of her job is to help organizations apply for grants to provide care in rural areas. She understands that people living in these places must come up with creative solutions to deal with their health care needs — whether it’s getting help in an emergency, receiving treatment for ongoing illnesses or softening the natural consequences of old age.
It’s a quickly changing landscape as more rural hospitals close, and some health policy analysts say it’s time communities made some hard decisions — starting with completely changing the health care structure in small towns.
For example, says a recent report by the Bipartisan Policy Center, instead of making sure each rural resident can easily get to a full-service hospital, some communities should consider what kind of primary care and more specialized care they could offer at a facility instead — short of having a full-service hospital.
Hospitals tend to be cornerstone institutions in rural communities. They provide jobs and contribute to a town’s economy. For many citizens in small-town America, losing the local hospital would threaten the livelihood of the town and its people, says Patrick Roche, chief operating officer at Faith Regional Health Services based in Norfolk, Neb.
“There are two things they don’t want to lose. The first one is their school, the second one is their hospital,” says Roche.
But there are big challenges to keeping these hospitals open. They cost money and it’s difficult to find a qualified workforce.
There are other concerns, including limited funding, regulatory restrictions, problems with transportation, broadband internet accessibility and the unique characteristics of the population, according to Dr. Anand Parekh, chief medical advisor with the Bipartisan Policy Center and one of the report’s authors.
“Rural America,” Parekh says, “is a little bit older, a little bit sicker, a little bit poorer.”
In 2016, the Census Bureau reported that 19.3 percent of the U.S. population lived in rural areas, which cover 97 percent of the country. Up to this point, the medical needs of that group have been addressed by a system that has medical facilities, many of which do receive some federal support, including about 1,300 small hospitals known as critical access hospitals.
A hospital is designated as critical access by the Centers for Medicare and Medicaid Services if has 25 beds or fewer, is more than 35 miles from another hospital and provides 24-hour emergency services.
The National Rural Health Association says 673 rural hospitals are at risk to close, and 210 of those are at “extreme risk”— 60 rural hospitals closed between 2010 and February 2016.
One of the main reasons for the significant rural hospital closures is that the average number of in-patients is low, says Schultz.
“Running a full hospital is very expensive — the overhead, 24/7 staffing, the facilities,” she says. “Think of a 25-bed hospital, and you’re only using four of your beds and how expensive that is.”
Residents of Tilden, Neb. — a town of less than 1,000 — know what happens when the town hospital can’t make ends meet. They lost their critical access hospital in 2014 and had to find a different solution for their medical care.
Roche explains that Faith Regional Health Services in Norfolk, just 22 miles away from Tilden, worked out an agreement to lease the hospital and clinic from the little town; Faith Regional then provided the medical operations—staffing, providers and equipment.
“The operations are, in effect, owned by Faith Regional and are operated just like any other clinic that is owned and operated by our system,” Roche says. But the facility in Tilden is no longer a full hospital.
“There’s been a fear in the air and you read a lot, and you hear a lot about hospitals closing,” says Schultz, who travels often to rural communities. “And that’s rightfully so. But if you look at the communities that are losing their hospitals, you need to look at, ‘What do they still have?’ “
The Bipartisan Policy Center and Helmsley Charitable Trust partnered to propose a possible solution for communities struggling to keep facilities afloat and provide quality care miles away from city and suburban hospitals and clinics.
Their January 2018 report, which surveyed health care professionals in seven states in the upper Midwest, says that the whole rural health care system needs to be addressed. Each community should determine the best health care structure, the report suggests, not the other way around. And that difficult analysis may lead to closing a small town hospital.
Darrold Bertsch, chief executive officer of Sakakawea Medical Center in Hazen, N.D., says he agrees with the idea of catering health care facilities to the population — whether it’s with an outpatient clinic, urgent care center, a hospital or something else.
“If communities had a little bit more flexibility,” he says, “then they could adapt a health care delivery system in their area that is more relevant to the needs that they have, rather than trying to make a hospital fit in a community where it might not be able to be supported anymore.”
The critical access hospital in Cody, Wyo., has stayed open — partially because of this idea of flexibility, says Jeanine Brus, who works as the laboratory director for the hospital.
Cody sits outside the eastern edge of Yellowstone National Park and is a town of about 10,000 people. Cody Regional Health, which includes the hospital and other health care facilities, such as a surgical center, a cancer center and a dialysis center, serves the town and the farms and ranches in a 200-mile radius, as well as tourists from the park.
Brus says that the key to adapting has been collaboration between the different facilities. And that’s been good for the health care workers, as well as the community, she says.
Bertsch from the North Dakota hospital says federal regulations and the way hospitals are reimbursed mean there’s no one-size-fits-all fix for every community.
Still, Parekh underscores his hope for the possibilities that can come when communities are open to new kinds of solutions.
“You know, you don’t have to close your hospital,” he says. “You can transform the hospital to meet your community needs, improve health and still continue to improve your local economy. Rural America can thrive as health care transforms.”
This story is part of NPR’s reporting partnership with Kaiser Health News.
Too Late To Operate? Surgery Near End Of Life Is Common, Costly

Maxine Stanich celebrated her 90th birthday with friends and family in 2010, more than two years after her implanted defibrillator was deactivated by Dr. Rita Redberg to comply with Stanich’s “do not resuscitate” directive.
Courtesy of Susan Giaquinto/Kaiser Health News
hide caption
toggle caption
Courtesy of Susan Giaquinto/Kaiser Health News
At 87, Maxine Stanich cared more about improving the quality of her life than prolonging it.
She suffered from a long list of health problems, including heart failure and chronic lung disease that could leave her gasping for breath.
When her time came she wanted to die a natural death, Stanich told her daughter, and she signed a “do not resuscitate” directive, or DNR, ordering doctors not to revive her should her heart stop.
Yet a trip to a San Francisco emergency room for shortness of breath in 2008 led Stanich to get a defibrillator implanted in her chest — a medical device to keep her alive by delivering a powerful shock to her heart if it started beating irregularly.
At the time, Stanich didn’t fully grasp what she had agreed to, even though she signed a document granting permission for the procedure, said her daughter, Susan Giaquinto.
That clarity came only during a subsequent visit to a different hospital, when a surprised ER doctor saw the defibrillator protruding from Stanich’s thin chest. It was the first time a doctor clearly explained what the defibrillator would mean for Stanich, said Giaquinto, who accompanied her mother on both hospital trips.
To Stanich’s horror, the ER doctor explained that the device wouldn’t allow Stanich to slip away painlessly. Instead, the defibrillator would give her a jolt “so strong that it will knock her across the room,” Giaquinto said.
Surgery like Stanich’s defibrillator implantation has become all too common among those near the end of life, experts say. Nearly 1 in 3 Medicare patients undergoes an operation in the year before death, even though the evidence shows that many are more likely to be harmed than to benefit from it.

Dr. Rita Redberg, director of women’s cardiovascular services at the University of California, San Francisco’s cardiology division, tends to her mother, Mae Redberg, in Mae’s apartment in New York City.
Yana Paskova for Kaiser Health News
hide caption
toggle caption
Yana Paskova for Kaiser Health News
The practice is driven by financial incentives that reward doctors for doing procedures, as well as a medical culture in which patients and doctors are reluctant to talk about how surgical interventions should be prescribed more judiciously, said Dr. Rita Redberg, a cardiologist who treated Stanich when she sought care at the second hospital a week after her defibrillator was implanted.
“We have a culture that believes in very aggressive care,” said Redberg, who specializes in heart disease in women at the University of California, San Francisco. “We are often not considering the chance of benefit and chance of harm, and how that changes when you get older. We also fail to have conversations about what patients value most.”
While surgery can be lifesaving for younger people, operating on frail, older patients rarely helps them live longer or returns the quality of life they once enjoyed, according to a 2016 paper in Annals of Surgery.
The cost of these surgeries — typically paid for by Medicare, the government health insurance program for people over 65 — involve more than money, said Dr. Amber Barnato, a professor at the Dartmouth Institute for Health Policy and Clinical Practice. Older patients who undergo surgery within a year of death spent 50 percent more time in the hospital than others, and nearly twice as many days in intensive care.
And while some robust octogenarians have many years ahead of them, studies show that surgery is also common among those who are far more frail.
Eighteen percent of Medicare patients have surgery in their final month of life and 8 percent in their final week, according to a 2011 study in The Lancet.
More than 12 percent of defibrillators were implanted in people older than 80, according to a 2015 study. Doctors implant about 158,000 of the devices each year, according to the American College of Cardiology. The total cost of the procedure runs about $60,000.
Procedures performed in the elderly range from major operations that require lengthy recoveries to relatively minor surgery performed in a doctor’s office, such as the removal of nonfatal skin cancers that would likely never cause any problems.
Research led by Dr. Eleni Linos has shown that people with limited life expectancies are treated for nonfatal skin cancers as aggressively as younger patients. Among patients with a nonfatal skin cancer and a limited time to live, 70 percent underwent surgery, according to her 2013 study in JAMA Internal Medicine.
When less is more
Surgery poses serious risks for older people, who weather anesthesia poorly and whose skin takes longer to heal. Among seniors who undergo urgent or emergency abdominal surgery, 20 percent die within 30 days, studies show.
With diminished mental acuity and an old-fashioned respect for the medical profession, some aging patients are vulnerable to unwanted interventions. Stanich agreed to a pacemaker defibrillator simply because her doctor suggested it, Giaquinto said. Many people of Stanich’s generation “thought doctors were God … They never questioned doctors — ever.”
According to the University of Michigan’s National Poll on Healthy Aging, published Wednesday, more than half of adults ages 50 to 80 said doctors often recommend unnecessary tests, medications or procedures. Yet half of those who’d been told they needed an X-ray or other test – but weren’t sure they needed it – went on to have the procedure anyway.
Dr. Margaret Schwarze, a surgeon and associate professor at the University of Wisconsin School of Medicine and Public Health, said that older patients often don’t feel the financial pain of surgery because insurance pays most of the cost.
When a surgeon offers to “fix” the heart valve in a person with multiple diseases, for example, the patient may assume that surgery will fix all of her medical problems, Schwarze said. “With older patients with lots of chronic illnesses, we’re not really fixing anything.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dr. Rita Redberg (left) struggles to stop other doctors from performing unnecessary procedures on her mother, Mae, (seated). Redberg’s daughter, Anna Larson, looks on.
Yana Paskova for Kaiser Health News
hide caption
toggle caption
Yana Paskova for Kaiser Health News
Even as a doctor, Redberg said, she struggles to prevent other doctors from performing too many procedures on her 92-year-old mother, Mae, who lives in New York City.
Redberg said doctors recently treated her mother for melanoma — the most serious type of skin cancer. After the cancer was removed from her leg, Redberg’s mother was urged by a doctor to undergo an additional surgery to cut away more tissue and nearby lymph nodes, which can harbor cancerous cells.
“Every time she went in, the dermatologist wanted to refer her to a surgeon,” Redberg said. “Medicare would have been happy to pay for it.”
But her mother often has problems with wound healing, she said, and recovery would likely have taken three months. When Redberg pressed a surgeon about the benefits, he said the procedure could reduce the chances of cancer coming back within three to five years.
Redberg said her mother laughed and said, “I’m not interested in doing something that will help me in three to five years. I doubt I’ll be here.”
Finding solutions
The momentum of hospital care can make people feel as if they’re on a moving train and can’t jump off.
The rush of medical decisions “doesn’t allow time to deliberate or consider the patients’ overall health or what their goals and values might be,” said Dr. Jacqueline Kruser, an instructor in pulmonary and critical care medicine and medical social sciences at the Northwestern University Feinberg School of Medicine.
Many hospitals and health systems are developing “decision aids,” easy-to-understand written materials and videos to help patients make more informed medical choices, giving them time to develop more realistic expectations.
After Kaiser Permanente Washington introduced the tools relating to joint replacement, the number of patients choosing to have hip replacement surgery fell 26 percent, while knee replacements declined 38 percent, according to a 2012 study in the journal Health Affairs. (Kaiser Permanente isn’t affiliated with Kaiser Health News, which is an editorially independent program of the Kaiser Family Foundation.)
In research findings published last year in JAMA Surgery and the Journal of Pain and Symptom Management, Schwarze, Kruser and colleagues suggested creating narratives to illustrate surgical risks, rather than relying on statistics.
Instead of telling patients that surgery carries a 20 percent risk of stroke, for example, doctors should lay out the best, worst and most likely outcomes.
In the best-case scenario, a patient might spend weeks in the hospital after surgery, living the rest of her life in a nursing home. In the worst case, the same patient dies after several weeks in intensive care. In the most likely scenario, the patient survives just two to three months after surgery.
“If someone says they can’t tolerate the best-case scenario — which involves them being in a nursing home — then maybe we shouldn’t be doing this,” Schwarze said.
Maxine Stanich died in 2010, just after her 90th birthday. Although Redberg had deactivated the defibrillator at Stanich’s request, it remained in her chest.
Kaiser Health News is a nonprofit news service covering health issues. You can follow Liz Szabo on Twitter: @LizSzabo.
Your 2018 Health Plan Must Comply With ACA Rules Or You Risk Tax Penalties

{kind=link}
Confused about whether your health plan is ACA-compliant? To be sure you’re using your state’s official marketplace, start with HealthCare.gov, and click on “see if I can change.”
Hero Images/Getty Images
hide caption
toggle caption
Hero Images/Getty Images
Health plans that don’t meet the standards of the Affordable Care Act. Work requirements for Medicaid coverage. Changes to Medicare’s approved drug lists. As the ground continues to shift on health care coverage, I’m answering readers’ queries this week about these three different types of plans:
I lost my job last year and my employer coverage ended in January. I bought a new plan through the marketplace that went into effect last month. I just received policy information, and it states that because the plan does not cover major medical services, I may have to pay additional taxes to the government. I was told that the plan didn’t cover major medical, but wasn’t told about any taxes. Will I be fined next year?
It sounds like you bought a plan that doesn’t comply with the Affordable Care Act’s requirements, and if that’s the case you may indeed have to pay a penalty for not having comprehensive coverage when you file your taxes next year.
The tax reform law repealed the individual penalty for not having health insurance, but that provision doesn’t take effect until 2019. So, for 2018, you may be charged the greater of $695 or 2.5 percent of your household income.
The federal- and state-run marketplaces established by the ACA sell only comprehensive plans that cover 10 essential health benefits, including “major medical” services like hospitalization and prescription drugs.
But some insurance broker websites call themselves marketplaces too, says Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. And that can be confusing. These companies may sell other insurance products — like short-term or accident coverage — alongside comprehensive plans that comply with the law.
Ever since the health law was passed, “There have been opportunistic companies trying to take advantage of consumer confusion to make money,” Corlette says.
If you aren’t happy with your plan, you may still be able to switch. Losing your employer coverage qualifies you for a 60-day special enrollment period to pick a new plan. Since it appears you’re still in that window, you may be able to choose a comprehensive plan.
To ensure you’re using your state’s official marketplace, go to healthcare.gov and click on “see if I can change.” That will take you to your state marketplace, even if you live in one of the dozen or so states that run their own exchanges.
I’m in a state that is looking into work requirements for Medicaid. At sign-up time, can I simply tell the exchange that I intend to be ineligible for Medicaid by refusing to work and get the premium tax credit to buy a private plan on the insurance marketplace?
Federal health law regulations don’t clearly address the situation you describe, but the short answer is probably not, according to policy analysts.
In general, people who are eligible for employer coverage or Medicaid — the federal-state health program for people with little income — can’t qualify for federal tax credits that help pay for premiums on plans sold on the health insurance exchanges.
This year, Kentucky and Indiana became the first states to receive federal approval to require some Medicaid recipients to put in 80 hours each month at a paid job, school or volunteer work (among other activities), to receive benefits. Nearly a dozen other states have made similar requests.
If you refuse to work, does that make you ineligible for Medicaid? The rules aren’t clear, says Judith Solomon, vice president for health policy at the Center on Budget and Policy Priorities.
States might argue that someone in your situation is eligible for Medicaid — you just have to fulfill the work requirements, says Timothy Jost, an emeritus professor of law at Washington and Lee University in Virginia, who is an expert on the health law.
There are other actions people could take — or fail to take — where this issue might come up. “You could argue that someone is not eligible because they haven’t completed the Medicaid application or provided the required documentation,” Jost says. “There are any number of requirements, but I can’t imagine someone saying they didn’t do those things and so they’re not eligible for Medicaid.”
Whatever the rules, it’s unlikely that many people will be in a position to consider taking this stance. To qualify for premium tax credits, your income must be between 100 and 400 percent of the federal poverty level (about $12,000 to $48,500 for an individual in 2018). But you’d also have to be eligible for Medicaid, generally with an income limit of 138 percent of poverty (about $16,750) in states that expanded coverage to adults. In addition, the Medicaid work requirements in your state would have to apply to you.
I picked a Medicare Part D drug plan that covered all the drugs I take. But as soon as I got my first Novolin R prescription filled, they notified me that they don’t cover it anymore. Can they just switch it like that?
Medicare drug plans can change their list of covered drugs, called formularies. If they’re doing so at the start of the new calendar year, as appears to have happened in your case, the plan may notify you of the change when you fill the prescription for the first time in the new year. At that time, the plan would typically give you a 30-day transition refill so you can switch to another drug that’s on the formulary or start the appeals process to continue taking your current insulin drug, Novolin R.
If you and your doctor think it’s important that you have Novolin R and not another drug that is similar, you can ask your plan to make an exception to allow you to continue to take the drug.
To go that route, you would need to get your doctor to “make the case for why that formulary drug is not the right drug” for you, says Casey Schwarz, senior counsel for education and federal policy at the Medicare Rights Center, an advocacy group.
Experts Say There's Little Connection Between Mental Health And Mass Shootings
President Trump has raised mental health as a key factor in mass shootings, including a call Thursday to create more mental hospitals. But experts say there’s little connection between a person’s mental illness and the likelihood of a mass shooting.