These 10 ERs Sharply Reduced Opioid Use And Still Eased Pain

Ashley Copeland (right) talks to her mom Sue Iverson in the Swedish Medical Center emergency department, near Denver. Copeland got a nerve-blocking anesthetic instead of opioids to ease her severe headache. At discharge she was advised to use over-the-counter painkillers, if necessary.
John Daley / CPR News
hide caption
toggle caption
John Daley / CPR News
One of the most common reasons patients head to an emergency room is pain. In response, doctors may try something simple at first, like ibuprofen or acetaminophen. And, at least up until recently, if that isn’t effective, the second line of attack has been the big guns.
“Percocet or Vicodin,” says Dr. Peter Bakes, an emergency medicine specialist at Swedish Medical Center in Englewood, Colo. “Medications that certainly have contributed to the rising opioid epidemic.”
Now though, physicians are looking for alternatives to help reduce opioid use and curtail potential abuse. Ten Colorado hospitals, including Swedish, participated in a six-month pilot project called the Colorado Opioid Safety Collaborative, aimed at cutting their use of the prescription painkillers. Launched by the Colorado Hospital Association, the project is believed to be the first in the nation to include this many hospitals in such an effort.
The collaborating ERs hoped to reduce their opioid use by 15 percent. Instead, Dr. Don Stader, an emergency physician at Swedish who helped develop and lead the study, says the institutions did much better — cutting their use of the drugs by 36 percent, on average.

Dr. Don Stader is associate medical director at Swedish Medical Center in Englewood, Colo., and a consultant on opioid use for the Colorado Hospital Association. “We all see the carnage that this opioid epidemic has brought,” he says. “And we know that we have to do something radically different.”
John Daley / CPR News
hide caption
toggle caption
John Daley / CPR News
“It’s really a revolution in how we approach patients and approach pain,” Stader says, “and I think it’s a revolution in pain management that’s going to help us end the opioid epidemic.”
The overall decrease amounted to 35,000 fewer opioid doses than were prescribed during the same period in 2016.
Their strategy calls for coordination across providers, pharmacies, clinical staff and administrators. And it introduces alternative procedures — using nonopioid patches for pain, for example. Another innovation, Stader says, is using ultrasound to help guide targeted injections of nonopioid pain medicines.
Rather than opioids, such as oxycodone, hydrocodone or fentanyl, Stader says, the doctors now try to use safer and less addictive alternative medicines, like ketamine and lidocaine, an anesthetic commonly used by dentists.
Lidocaine was by far the leading alternative; its use in the project’s ERs rose 451 percent. Ketamine use was up 144 percent.
Meanwhile, the use of methadone dropped by about 51 percent and oxycodone prescriptions dropped 43 percent. The use of codeine was cut 35 percent and fentanyl’s use dropped by roughly 11 percent.
“We all see the carnage that this opioid epidemic has brought,” Stader says. “We all see how dangerous it’s been for patients, and how damaging it’s been for our communities. And we know that we have to do something radically different.”
Claire Duncan, a clinical nurse coordinator in the ER at Swedish, says the new approach has required intensive training of health care providers. She says she was surprised by the pushback from patients.
“They say ‘only narcotics work for me, only narcotics work for me,’ ” says Duncan. “Because they haven’t had the experience of that multifaceted care, they don’t expect that ibuprofen is going to work, or that ibuprofen plus Tylenol, plus a heating pad plus stretching measures — they don’t expect that to work.”

Dr. Peter Bakes is an emergency medicine doctor at Swedish Medical Center. Rather than reaching first for opioids for their patients who have severe pain, doctors in his ER have been trained to turn more often now to safer and less addictive alternative medicines, like ketamine and lidocaine.
John Daley / CPR News
hide caption
toggle caption
John Daley / CPR News
The program requires a big culture change, Duncan says, encouraging staff to change the conversation from pain medication only, to ways to treat pain that help patients better understand and cope with it.
Emergency medical workers are all too familiar with the ravages of the opioid epidemic. They see patients struggling with the consequences every day. But Bakes, the ER doctor at Swedish, says this project has changed many minds, empowering health care professionals to combat an opioid crisis they unwittingly helped create.
“I think that any thinking person — or any thinking physician, or provider of patient care — really felt to some extent guilty, but powerless to enact meaningful change,” Bakes says.
The pilot project has proven so successful that Swedish and the other emergency departments involved will continue the new protocols and share what they’ve learned. Stader says the Colorado Hospital Association plans to help spread the word about opioid safety, too; he expects to see the new strategies adopted statewide by year’s end.
“And I think if we did put this into practice in Colorado, and showed our success,” he says, “this would spread like wildfire across the country.”
The 10 hospitals that took part in the Colorado collaboration were scattered all over the state — Boulder Community Health; Gunnison Valley Health; Sedgwick County Health Center; Sky Ridge Medical Center; Swedish Medical Center; UCHealth Greeley Emergency and Surgical Center; UCHealth Harmony Campus; UCHealth Medical Center of the Rockies; UCHealth Poudre Valley Hospital and UCHealth Yampa Valley Medical Center.
This story is part of NPR’s reporting partnership with Colorado Public Radio and Kaiser Health News. John Daley can be found on Twitter @CODaleyNews.
Does A Larger Role For Midwives Mean Better Care?

A new study offers a systematic look at what midwives can and can’t do in different states, offering evidence that empowering them could boost maternal and infant health.
Trina Dalziel/Getty Images/Ikon Images
hide caption
toggle caption
Trina Dalziel/Getty Images/Ikon Images
In Great Britain, midwives deliver half of all babies, including Kate Middleton’s first two children, Prince George and Princess Charlotte. In Sweden, Norway and France, midwives oversee most expectant and new mothers, enabling obstetricians to concentrate on high-risk births. In Canada and New Zealand, midwives are so highly valued that they’re brought in to manage complex cases that need special attention.
All of those countries have much lower rates of maternal and infant mortality than the U.S. Here, severe maternal complications have more than doubled in the past 20 years. Shortages of maternity care have reached critical levels: Nearly half of U.S. counties don’t have a single practicing obstetrician-gynecologist, and in rural areas, the number of hospitals offering obstetric services has fallen more than 16 percent since 2004. Nevertheless, thanks in part to opposition from doctors and hospitals, midwives are far less prevalent in the U.S. than in other affluent countries, delivering about 10 percent of babies, and the extent to which they can legally participate in patient care varies widely from one state to the next.
Now a new study, a systematic look at what midwives can and can’t do in the states where they practice, offers new evidence that empowering them could significantly boost maternal and infant health. The five-year effort by researchers in Canada and the U.S., published Wednesday, found that states that have done the most to integrate midwives into their health care systems, including Washington, New Mexico and Oregon, have some of the best outcomes for mothers and babies. Conversely, states with some of the most restrictive midwife laws and practices — including Alabama, Ohio and Mississippi — tend to do significantly worse on key indicators of maternal and neonatal well-being.
“We have been able to establish that midwifery care is strongly associated with lower interventions, cost-effectiveness and improved outcomes,” said lead researcher Saraswathi Vedam, an associate professor of midwifery who heads the Birth Place Lab at the University of British Columbia.
Many of the states characterized by poor health outcomes and hostility to midwives also have large African-American populations, raising the possibility that greater use of midwives could reduce racial disparities in maternity care. African-American mothers are three to four times more likely to die in pregnancy or childbirth than their white counterparts; black babies are 49 percent more likely to be born prematurely and twice as likely to perish before their first birthdays.
“In communities that are most at risk for adverse outcomes, increased access to midwives who can work as part of the health care system may improve both outcomes and the mothers’ experience,” Vedam said.
That’s because of the midwifery model, which emphasizes community-based care, close relationships between providers and patients, prenatal and postpartum wellness, and avoiding unnecessary interventions that can spiral into dangerous complications, said Jennie Joseph, a British-trained midwife who runs Commonsense Childbirth, a Florida birthing center and maternal care nonprofit. “It’s a model that somewhat mitigates the impact of any systemic racial bias. You listen. You’re compassionate. There’s such a depth of racism that’s intermingled with [medical] systems. If you’re practicing in [the midwifery] model you’re mitigating this without even realizing it.”
The study, published in the peer-reviewed journal PLOS ONE, analyzes hundreds of laws and regulations in 50 states and the District of Columbia — things like the settings where midwives are allowed to work, whether they can provide the full scope of pregnancy- and childbirth-related care, how much autonomy they have to make decisions without a doctor’s supervision, and whether they can prescribe medication, receive insurance reimbursement or obtain hospital privileges. Then researchers overlaid state data on nine maternal and infant health indicators, including rates of cesarean sections, premature births, breastfeeding and neonatal deaths. (Maternal deaths and severe complications were not included because data is unreliable).
The differences between state laws can be stark. In Washington, which has some of the highest rankings on measures such as C-sections, premature births, infant mortality and breastfeeding, midwives don’t need nursing degrees to be licensed. They often collaborate closely with ob/gyns, and can generally transfer care to hospitals smoothly when risks to the mother or baby emerge. They sit on the state’s perinatal advisory committee, are actively involved in shaping health policy, and receive Medicaid reimbursement even for home births.
At the other end of the spectrum, North Carolina not only requires midwives to be registered nurses, but it also requires them to have a physician sign off on their application to the state for approval to practice. North Carolina scores considerably worse than Washington on indices such as low-birthweight babies and neonatal deaths.
Neel Shah, an assistant professor at Harvard Medical School and a leader in the movement to reduce unnecessary C-sections, praised the study as “a remarkable paper — novel, ambitious, and provocative.” He said licensed midwives could be used to solve shortages of maternity care that disproportionately affect rural and low-income mothers, many of them women of color. “Growing our workforce, including both midwives and obstetricians, and then ensuring we have a regulatory environment that facilitates integrated, team-based care are key parts of the solution,” he said.
To be sure, many other factors influence maternal and infant outcomes in the states, including access to preventive care and Medicaid; rates of chronic disease such as diabetes and high blood pressure; and prevalence of opioid addiction. And the study doesn’t conclude that more access to midwives directly leads to better outcomes, or vice versa. Indeed, South Dakota, which ranks third from the bottom in terms of midwife-friendliness, scores well on such key indicators as C-sections and preterm births. Even North Carolina is average on C-section rates, breastfeeding, and prematurity.
The findings are unlikely to quell the controversies over home births, which are almost always handled by midwives and comprise a tiny but growing percentage of deliveries in the U.S., or fears among doctors and hospitals that closer collaborations with midwives will raise malpractice insurance rates. In fact, said Ann Geisler, who runs the Florida-based Southern Cross Insurance Solutions, which specializes in insuring midwives, her clients’ premiums tend to be just one-tenth of premiums for an ob/gyn because their model of care eschews unnecessary interventions or technology. Far from being medical renegades, the vast majority of midwives want to be integrated into the medical system, she said.
Generally, licensed midwives only treat low-risk women, Geisler said. If the patients become higher risk, midwives are supposed to transfer them to a doctor’s care. Since many ob/gyns only see midwife patients when a problem emerges, she said, they may develop negative views of midwives’ skills.
You can read a full report from our partner, ProPublica, here.
Synergy Between Nurses And Automation Could Be Key To Finding Sepsis Early

Rosemary Grant is a registered nurse and helps coordinate sepsis care at Harborview Medical Center in Seattle. The center’s goal, she says, is to get a patient who might be developing sepsis antibiotics within three hours.
Ian C. Bates for NPR
hide caption
toggle caption
Ian C. Bates for NPR
A quarter of a million Americans die every year from sepsis, which is the body’s reaction to overwhelming infection. This cascade of organ failure can be nipped in the bud if health care workers know it’s ramping up, but that’s often not easy to do.
“Sepsis is a really frustrating disease,” says Dr. David Carlbom, a critical care pulmonologist, and medical director of the sepsis program at the Harborview Medical Center in Seattle. “There’s no blood test for sepsis,” he says. “There’s nothing you can look at under the microscope and say ‘this is sepsis.’ “
So a few years ago, Carlbom set out to devise a system that uses more subtle clues from a patient’s day-to-day electronic health records to send up warning flags of impending sepsis.
The automated system looks for patterns in symptoms like high temperature, low temperature, low blood pressure, fast breathing and high white-blood-cell counts. No single symptom signals sepsis, but certain patterns suggest this condition could be emerging.
Rosemary Grant, a registered nurse who coordinates sepsis care at Harborview, explains how it works as we stand at a nursing station in the hospital.
The previous day, a red box appeared on a computer screen next to the name of a patient who had been hospitalized for several weeks following a motorcycle accident. The computer prompted the nurse responsible for that patient to assess whether his constellation of symptoms was an early sign of sepsis.
“If the nurse says yes, then the provider is automatically paged, out of the computer system,” Grant says.
The doctor is supposed to respond within half an hour, she says, and the overall goal is to get a patient who might be developing sepsis antibiotics within three hours.
But faster breathing might also be due to a walk down the corridor, and having an elevated number of white blood cells is not a reliable sepsis indicator in someone with cancer. Given the general nature of these symptoms, most of the time the nurse will report that the alert is just a false alarm.
Once one alarm is triggered, nurses aren’t notified again for 12 hours, Grant adds — and that helps reduce the number of annoying false alarms the hospital staff must handle.
If the nurse says it’s not sepsis, Grant says, “then the computer system just asks ‘why do you think the patient has these abnormal vital signs?’ “
The nurse may type in that the patient’s heart rate was up because he was exercising, or has a high pulse because she’s in pain. It’s a partnership between the automation and the human being. And while systems like this are increasingly common in hospitals, the synergy between nurses and computers is a hallmark of the Seattle program.
“Just having the nurses really being in tune with their patients is really what makes the system work,” Grant says. And it is working, she says. Since the system was installed in 2011 — and updated in 2017 — hospital mortality has fallen.
We head over to the room of the injured 34-year-old motorcyclist to see how he’s doing. Matthew Clark says his world changed on Jan. 15, when he had an unfortunate encounter with a car.
“I was just on the way to make some chicken chili for my girlfriend,” he says, “and a young distracted driver who wasn’t looking kind of plowed into me.” Two big bones in his left leg were broken, requiring a series of operations to set right.
But nine days after the accident, Clark got a clue his recovery was taking a turn for the worse when a friend came into his hospital room and he had trouble waving to her.
“I noticed my hands were shaking,” he says, “and my blood started to leave my hands and feet. I just looked at her and said ‘I need some help.’ “
The hospital’s internal 911 system responded with a team that, among other things, provided intravenous antibiotics to prevent his apparent infection from raging out of control and becoming septic shock.
“My temperature dropped incredibly,” he says. “I’d never been so cold or shook so hard in my life.”
And 24 hours later, he says, he was back to his old self.
In this case, the patient’s alert actually popped up on the computer screen long after the medical team had stepped in.

Dr. David Carlbom, a critical care pulmonologist at UW Medicine’s Harborview Medical Center, says sepsis has long frustrated clinicians. “There’s no blood test,” he says. “There’s nothing you can look at under the microscope and say ‘this is sepsis.’ ”
Ian C. Bates for NPR
hide caption
toggle caption
Ian C. Bates for NPR
“I think his case is a great example of action happening before the computer catches up,” Carlbom says. “The vital signs are measured and dealt with at the bedside before they’re entered into the computer.”
In fact, that need to enter vital signs manually into the electronic medical record is a shortcoming of this system. The computer may be ever vigilant for signs of infection, but it only gets new data to crunch a few times a day.
This isn’t simply an issue for the system at Harborview — it’s a shortcoming for automated sepsis-detection programs elsewhere. Medical researchers are actively working to close that gap, says Dr. Matthew Churpek at the University of Chicago.
“We’re partnering now with a company that has a device that goes under a patient’s mattress and can continuously calculate their heart rate and respiratory rate in real time,” Churpek says.
His team and others are also working on more accurate computer algorithms, to reduce the number of false alarms that are a problem both in Seattle and in similar systems around the country.
Doctors have struggled to find a good treatment for sepsis. For example, last year Dr. Paul Marik announced that a protocol involving intravenous vitamin C, thiamine and steroids dramatically reduced the number of sepsis deaths in his hospital’s intensive care unit in Norfolk, Va. That unproven treatment has just begun to be studied in a series of careful clinical trials.
Carlbom uses that experimental therapy sometimes, but says it would be much better to prevent the condition.
“We use all these therapies in the ICU as a rescue tool when people are very sick dying of septic shock,” he says, “but I think early discovery will probably affect mortality more.”
You can contact Richard Harris via email: rharris@npr.org.
Europe Saw 4-Fold Increase In Measles Cases In 2017

A measles vaccine, such as the one shown here from a Los Angeles clinic, is highly effective in preventing the spread of measles.
Lucy Nicholson/Reuters
hide caption
toggle caption
Lucy Nicholson/Reuters
Measles is highly contagious, but easily preventable with a vaccine.
However, the numbers of measles cases sharply jumped up in Europe in 2017, according to new data released by the World Health Organization.
In 2017, the disease affected 21,315 people, compared to 5,273 in 2016. Last year, 35 people died in Europe because of measles.
“Every new person affected by measles in Europe reminds us that unvaccinated children and adults, regardless of where they live, remain at risk of catching the disease and spreading it to others who may not be able to get vaccinated,” said Zsuzsanna Jakab, WHO’s Regional Director for Europe. She describes the loss of lives as a “tragedy we simply cannot accept.”
The WHO says that 15 countries in Europe saw outbreaks of 100 or more cases. Romania had the most, with 5,562, followed by Italy, with 5,006, and Ukraine, with 4,767.
“These countries have experienced a range of challenges in recent years, such as declines in overall routine immunization coverage, consistently low coverage among some marginalized groups, interruptions in vaccine supply or underperforming disease surveillance system,” the WHO report stated.
According to the BBC, Romania has a shortage of the vaccine. “It is also thought that the country’s large Roma population, who often live in severe poverty, are at particular risk of contracting and spreading the virus,” the broadcaster added.
In response to the burgeoning outbreak in Italy last year, the country made vaccines mandatory for measles and a number of other diseases for school children.
“Kids up to 6 years old won’t be accepted into nursery schools without them,” reporter Christopher Livesay told NPR. “And parents sending their children to school after that age without vaccinating them first will now face fines of up to $8,380.”
That was controversial and sparked protest. Like many other countries, some politicians in Italy have argued against the policy by referencing widely discredited research that suggests a link between vaccines and autism.
The WHO says other European countries that saw large outbreaks in 2017 are:
“Greece (967), Germany (927), Serbia (702), Tajikistan (649), France (520), the Russian Federation (408), Belgium (369), the United Kingdom (282), Bulgaria (167), Spain (152), Czechia (146) and Switzerland (105).”
As NPR’s Michaeleen Doucleff has reported, measles cases have generally seen a dramatic drop worldwide since the 1980s, from more than 4 million cases annually to less than 500,000. However, she adds that health workers have struggled to push vaccination rates past 78 percent, though they say rates of 90 to 95 percent are needed to stop outbreaks.
Poor countries such as Guinea, Mongolia and Nigeria are seeing a high number of cases, she adds. As NPR’s Jason Beaubien reports, Rohingya camps in Bangladesh have also seen recent outbreaks.
There have also been several recent outbreaks in the U.S., primarily impacting people who were never vaccinated for measles. The U.S. saw 118 cases of measles in 2017, according to the CDC. A 2015 outbreak across multiple states is believed to have originated with a traveler who visited Disneyland.
An outbreak hit Minnesota in 2017, sickening at least 79 people. A large number of those impacted are members of the Somali-American community in Minneapolis, many of whom are wary of vaccines.
Patients with measles have symptoms such as fever, cough and runny nose at the onset, according to the CDC. After about 3 days, a rash of “flat red spots” appears on the infected person’s body.
ER Reduces Opioid Use By More Than Half With Dry Needles, Laughing Gas

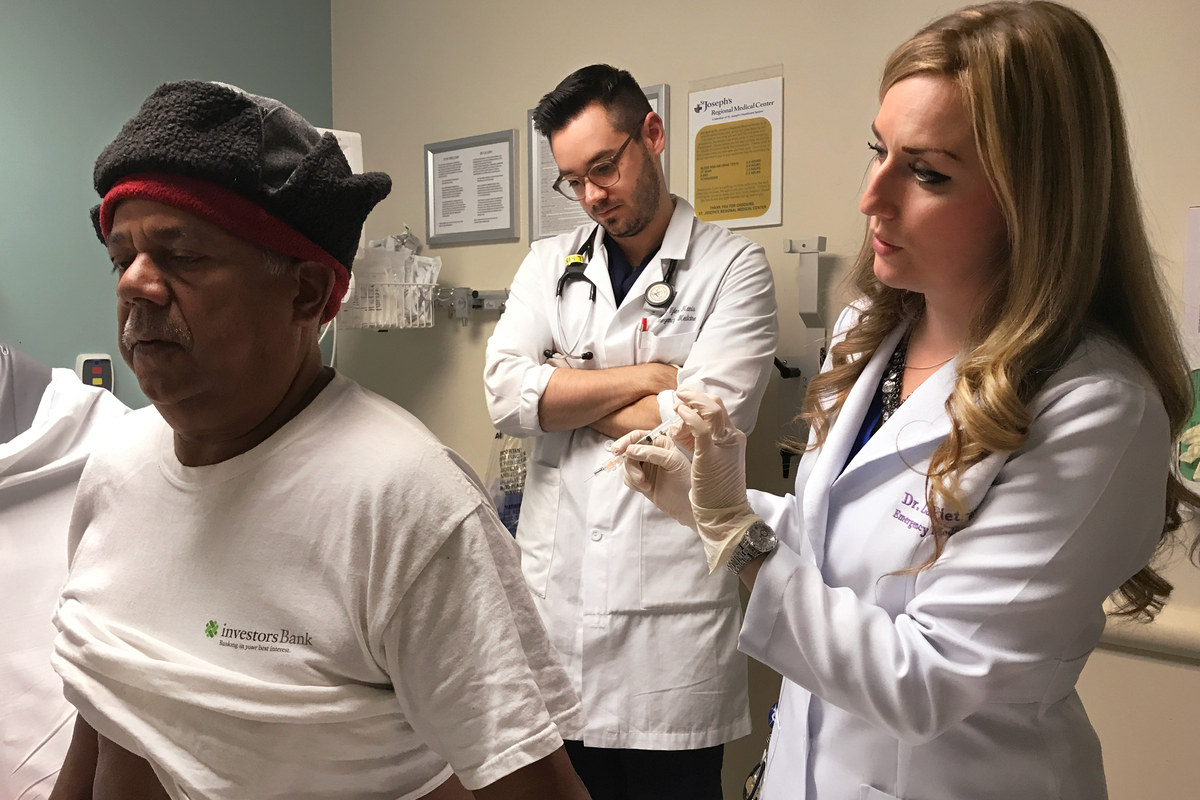
Francisco Hidalgo prepares to receive a trigger point injection from Dr. Alexis LaPietra (right) at St. Joseph’s University Medical Center in Paterson, N.J., while Dr. Tyler Manis observes. An alternative to opioids, the trigger point injection involves dry needling to stop pain from a muscle spasm and a shot of local anesthetic for the soreness from the needle.
Hansi Lo Wang/NPR
hide caption
toggle caption
Hansi Lo Wang/NPR
NPR’s “Take A Number” series is exploring problems around the world — and solutions — through the lens of a single number.
One of the places many people are first prescribed opioids is a hospital emergency room. But in one of the busiest ERs in the U.S., doctors are relying less than they used to on oxycodone, Percocet, Vicodin and other opioids to ease patients’ pain.
In an unusual program designed to help stem the opioid epidemic, the emergency department at St. Joseph’s University Medical Center in Paterson, N.J., has been exploring alternative painkillers and methods. That strategy has led to a 58 percent drop in the ER’s opioid prescriptions in the program’s first year, according to numbers provided by St. Joseph’s Healthcare System’s chair of emergency medicine, Dr. Mark Rosenberg.
“There is a complete change in philosophy, a complete change in culture in the department,” says Rosenberg, who launched the Alternatives to Opiates program in 2016 with Dr. Alexis LaPietra, the medical director of pain management in the emergency department.
Last year, the program was highlighted during a visit to the hospital by the chair of President Trump’s commission to study the national opioid crisis, former New Jersey Gov. Chris Christie.
Patients are experiencing the shift in care for painful symptoms related to various diagnoses, including kidney stones, broken bones and muscle spasms.
It was a muscle spasm and a deep bruise from a subsequent fall that brought Jonathan Milton, a 43-year-old forklift driver from Jersey City, N.J., hobbling into St. Joseph’s ER one morning in January.

Jonathan Milton (right) receives instructions from a St. Joseph’s physician, Dr. Jessica Lim, on how to treat pain from muscle tension at home using drugstore pain relievers — ibuprofen or acetaminophen — and a warm compress.
Hansi Lo Wang/NPR
hide caption
toggle caption
Hansi Lo Wang/NPR
A couple nights earlier, Milton was at home, lying on the floor and watching TV. He accidentally fell asleep on his left side. When he woke up the next morning, he could barely get up. From his left hip down to his leg, he says, the spasm left him feeling “like somebody just came into that room, just kicked me and kept moving.” Later at work, when he tried to get up into the forklift, he fell.
“I was so much in pain — tears were coming out my eyes,” he said as he waited in a hospital chair for more instructions from his doctors.
Milton has come into this ER in pain before.
“I did see from your visit you were here for that shoulder sprain,” said LaPietra, after checking the hospital’s records about Milton’s 2011 visit. “You did get opioids. You got Percocet.”
Back then, opioid painkillers were part of the emergency department’s first line of offense against pain. Today, opioids are not banned, but LaPietra says sometimes the best way to reduce the pain from a muscle spasm, for example, is dry needling of a trigger point, not a pill.
“Because it’s so contained, it’s hard for that medication to actually get into the spasm,” she explains, adding that the dry needle can break up the muscle tissue and mechanically stop the spasm and the pain — with no medication needed. The dry needling is followed with a small injection of a local anesthetic for the soreness caused by the needle.
The ER team at St. Joseph’s employs a number of other pain-relieving strategies, too: using patches of lidocaine (a non-opioid painkiller); ultrasound to find nerves so they can inject numbing agents; laughing gas for patients to breathe in through a mask, and even a harpist to roam the halls to soothe patients, who are then often sent home with instructions to use ibuprofen, acetaminophen or a warm compress rather than opioids.
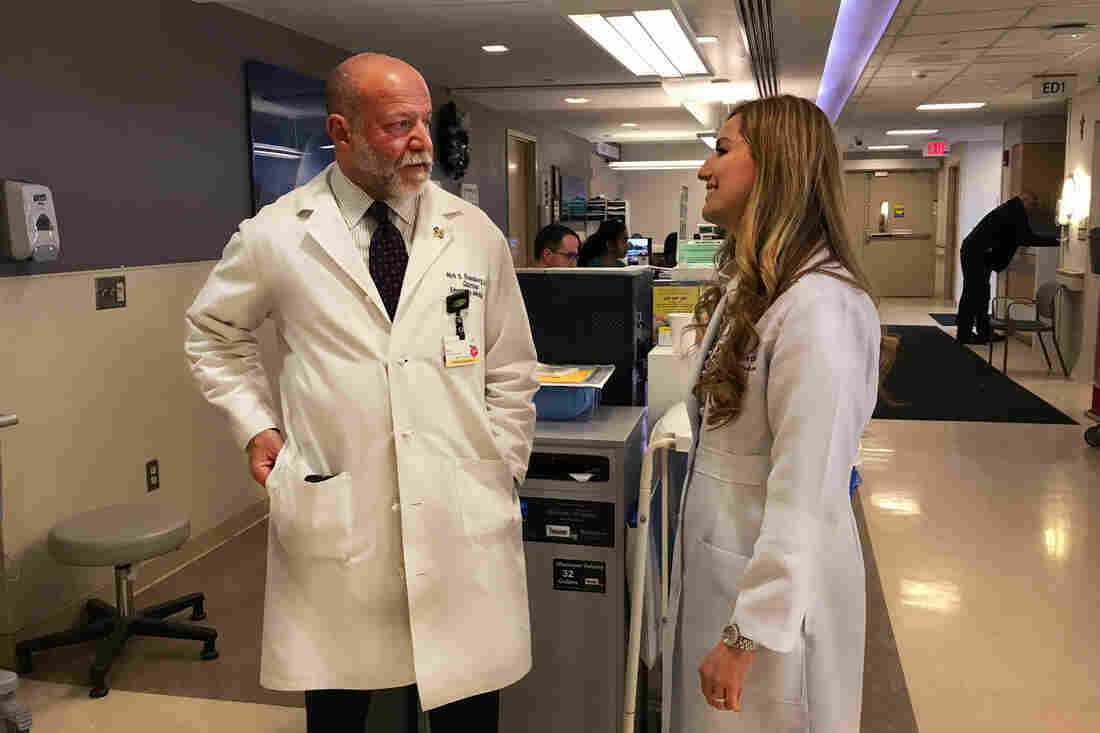
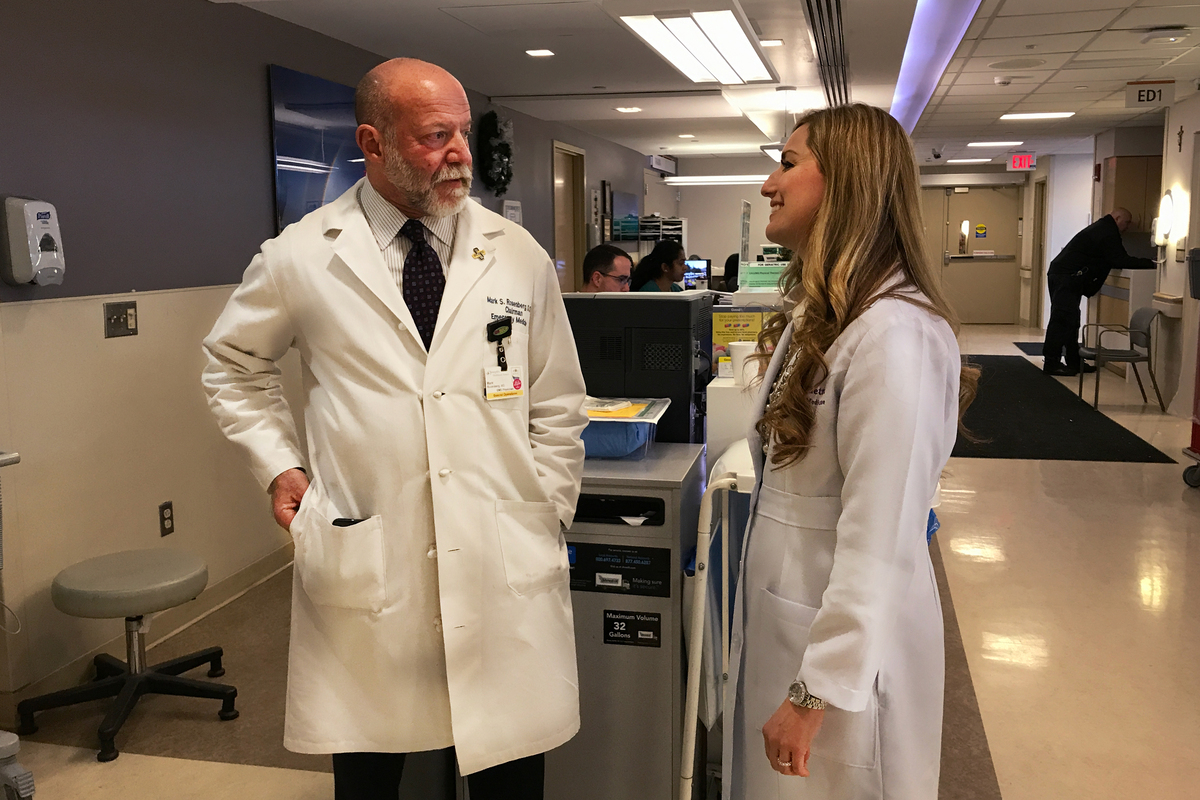
Dr. Mark Rosenberg (left) and LaPietra led the shift away from using opioids as the first line of offense against pain in the emergency room at St. Joseph’s.
Hansi Lo Wang/NPR
hide caption
toggle caption
Hansi Lo Wang/NPR
“We have to go back to times when things were a little more simple,” LaPietra says. “Those easy, at-home techniques — good patient education, really — they help a lot with some of that pain that patients have to deal with when they go home.”
But what may sound like common sense now — in light of the increased awareness of how addictive opioids can be — still requires a major culture shift among ER doctors who have prescribed these pills for years.
“It took a little bit of getting used to,” says Dr. Ninad Shroff, an attending physician in St. Joseph’s ER. “I’ve been doing this for about 20 years, so for me, it was a big change.”
Two years into the alternatives-to-opioids program, however, Shroff says during some shifts in the ER, where he mainly treats bumps, bruises and other musculoskeletal injuries, he doesn’t prescribe a single opioid. He still finds that “unbelievable,” he says.
Rosenberg, who runs the ER, says doctors at other hospitals nearby are noticing the shift at St. Joseph’s. He says he’s been asked, “Why are all the drug users from your area coming to my emergency department?”
“It’s because they’re not going to get opioids at our emergency department unless they’re absolutely needed,” Rosenberg says.
One challenge his program has had to work through is the cost of using alternatives to opioids. A few times, doctors had to work with pharmacists to find more affordable alternatives to the alternatives. For example, instead of prescribing lidocaine patches for patients to put on at home, doctors have switched to lidocaine ointment or cream, which is often covered by insurers.
“The insurance companies don’t embrace all the alternative treatments and instead would rather frequently have us prescribe opioids because they tend to be inexpensive and readily available,” he says.
Other emergency departments have rolled out alternatives to opioids at a smaller scale. But the model that St. Joseph’s has developed is now being copied at other facilities, including some in the UCHealth system in Colorado.

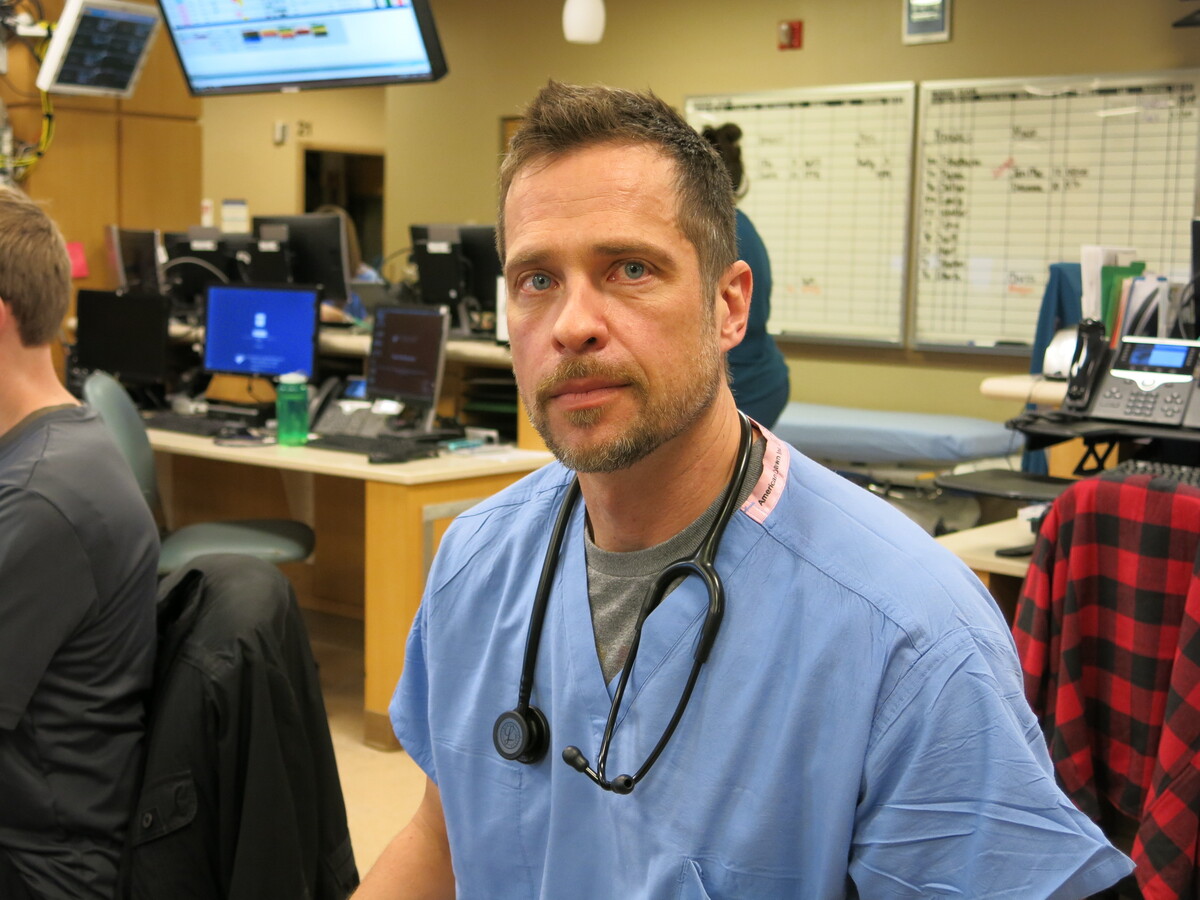
Dr. Thomas Brabson, chairman of emergency services at AtlantiCare Regional Medical Center in Atlantic City, N.J., has started an alternatives-to-opioids program in his hospital’s ER that’s modeled after St. Joseph’s University Medical Center’s program.
Hansi Lo Wang/NPR
hide caption
toggle caption
Hansi Lo Wang/NPR
“A lot of people now are very sensitive to the opioid epidemic,” says Dr. Thomas Brabson, chairman of emergency services at AtlantiCare Regional Medical Center in Atlantic City, N.J., where he launched a similar opioid-alternative program in 2016.
“The pleasant feeling of the opioids was something that people presumed was what the patients wanted, and that would help with your customer service scores,” Brabson explains, adding that now more patients are asking physicians not to prescribe any opioids.
It’s a change in expectations about the painkillers that you also hear from patients.
“Don’t give me that,” says Milton, the forklift driver with a muscle spasm. “I’d rather just keep dealing with the Motrin or the Advil.”
For his shoulder sprain back in 2011, doctors at St. Joseph’s gave Milton a dose of Percocet in the ER and more pills to take home. But during his recent visit, Dr. Jessica Lim put a patch of lidocaine on his left side and told him to take Motrin and Tylenol and to stretch at home.
“We were considering giving you a muscle relaxer,” Lim explained to Milton, “and I know you don’t like that feeling. So we’re not going to give it to you. This is even more on you to do the work yourself at home, and I know a lot of patients don’t like hearing that.”
But Milton was OK with her advice — and glad to leave the ER with no opioids.
Anthem Says Eye Surgeons Should Monitor Cataract Anesthesia Themselves

Royal Australian Navy Lt. Elizabeth Livingstone and Singapore Army Maj. Paul Zhao perform cataract surgery aboard the hospital ship USNS Mercy during a visit to Quy Nhon, Vietnam in 2010.
Mass Communication Specialist 2nd Class Eddie Harrison/U.S. Navy
hide caption
toggle caption
Mass Communication Specialist 2nd Class Eddie Harrison/U.S. Navy
If you need cataract surgery, your eye surgeon may have to do double duty as your anesthetist under a new policy by health insurer Anthem. In a clinical guideline released this month, the company says it’s not medically necessary to have an anesthesiologist or nurse anesthetist on hand to administer and monitor sedation in most cases.
Some ophthalmologists and anesthesiologists say the policy jeopardizes patient safety, and they are calling on Anthem to rescind it.
“The presence of anesthesia personnel is one of the key ingredients in the patient safety and effectiveness of cataract surgery today,” says Dr. David Glasser, an ophthalmologist in Columbia, Md., who is secretary for federal affairs at the American Academy of Ophthalmology, a professional group for eye physicians and surgeons. “An ophthalmologist cannot administer conscious sedation and monitor the patient and do cataract surgery at the same time.”
Anthem, which offers commercial insurance plans in 14 states, says anesthesia needs vary and so should coverage. According to a statement from the company:
“Anthem’s Medical Policy and Technology Assessment Committee, a majority of whom are external physicians, reviewed the available evidence addressing the use of general anesthesia and monitored anesthesia care for cataract surgery. According to the literature reviewed, there is no one definitive approach regarding the use of anesthesia for cataract surgery and patient-specific needs should be taken into consideration as well as potential risk of harm to individuals who are sedated during surgical procedures.”
Medicare, the health care program for people age 65 and older, covers cataract surgery, including anesthesia services.
A cataract, typically related to aging, is caused by clumps of protein that cloud the lens of the eye and can distort vision. During a cataract operation, the surgeon makes an incision in the surface of the eye with a laser or blade and then uses a tool to break up the clouded lens, pull it out and replace it with an artificial one.
Cataract surgery is common. More than half of Americans have either had a cataract or had cataract surgery by the time they reach age 80, according to the National Eye Institute.
Surgery is typically performed on an outpatient basis and takes less than an hour. Though drowsy while sedated, patients are generally conscious during the procedure and can hear what’s said to them and speak if necessary.
Eye surgeons often have an anesthesiologist or a nurse anesthetist present to administer intravenous drugs to help keep the patient relaxed and ensure they don’t move during the operation as well as monitor their vital signs and adjust medication as necessary.
Anthem’s new policy states that this type of monitored anesthesia care is medically necessary only if the patient is under 18 years old, or is unable to cooperate or communicate because of dementia or other medical conditions, can’t lie flat, has known problems with anesthesia, or if a complex surgery is anticipated.
But some ophthalmologists and anesthesiologists disagree.
“I wouldn’t even consider doing a cataract surgery without an anesthesiologist or nurse anesthetist in the room,” says Dr. David Aizuss, an eye surgeon who is president-elect of the California Medical Association. “If you’re working inside the eye it’s a very confined space, and if the patient gets agitated and starts moving around you have to get the equipment out of the eye very quickly.”
Although Anthem posted the new policy online, providers are seeking clarification from the company about the timing of its implementation in their states, physicians said.
Until then, some practices are taking no chances. At the Freedom Vision Surgery Center in Encino, Calif., where Aizuss practices, Anthem patients who come in for cataract surgery are asked to pay $400 out-of-pocket upfront for anesthesia services.
Professional groups representing California eye physicians and anesthesiologists have written to Anthem requesting the policy be rescinded. In addition, the California Medical Association has lodged complaints with state regulators.
This isn’t the first time Anthem has come under scrutiny for changes to its clinical guidelines that some have charged help the company’s bottom line at patients’ expense. Last year, the company said it would no longer pay for emergency department visits it later determined were not emergencies. Then in September it said it would no longer pay for imaging tests like MRIs in many cases if patients got them at hospital-owned centers rather than independent imaging centers.
Last week, Modern Healthcarereported that the company says it was modifying its ER rule so that certain types of visits would always be paid for, including those by patients who are directed to the emergency department by their provider or have recently had surgery.
Some safety experts say they were concerned about Anthem’s new policy, even for routine cataract surgeries.
“If you’re putting a knife in my eye, that’s not routine for me,” says Leah Binder, president and CEO of the Leapfrog Group, a nonprofit organization that advocates for improved safety and quality at hospitals. Noting that anesthesiologists and nurse anesthetists were pioneers in the patient safety movement, she says there are better ways for Anthem to save money than shutting them out of the operating room.
“How about identifying the surgeons who have the highest complication rates, and letting patients know about them?” she suggested.
Kaiser Health News is an editorially independent news service that is part of the nonpartisan Henry J. Kaiser Family Foundation. Michelle Andrews is on Twitter @mandrews110.
An Out-Of-Network Lab, An Elaborate Urine Test And Then A Surprise Bill

Urine testing to diagnose illness or to detect the presence of drugs is generally routine. But a woman who gave her doctor a urine sample months after back surgery got socked with a huge bill.
SPL/Science Source
hide caption
toggle caption
After Elizabeth Moreno had back surgery in late 2015, her surgeon prescribed an opioid painkiller and a follow-up drug test that seemed routine — until the lab slapped her with a bill for $17,850.
A Houston lab had tested her urine sample for a constellation of legal and illicit drugs, many of which Moreno says she had never heard of, let alone taken.
“I was totally confused. I didn’t know how I was going to pay this,” said Moreno, 30, who is finishing a degree in education at Texas State University in San Marcos, and is pregnant with twins.
Her bill shows that Sunset Labs LLC charged $4,675 to check her urine for a slew of different types of opioids: $2,975 for benzodiazepines, a class of drugs for treating anxiety, and $1,700 more for amphetamines. Tests to detect cocaine, marijuana and phencyclidine, an illegal hallucinogenic drug also known as PCP or angel dust, added $1,275 more.
The lab also billed $850 to test for buprenorphine, a drug used to treat opioid addiction, and tacked on an $850 fee for two tests to verify that nobody had tampered with her urine specimen.
Total bill: $17,850 for lab tests that her insurer, Blue Cross and Blue Shield of Texas, refused to cover, apparently because the lab was not in her insurance network. The insurer sent Moreno an “explanation of benefits” that says it would have valued the work at just $100.92.
Moreno’s father, in a complaint to the Texas attorney general’s office about the bill, identified the Houston surgeon who ordered the costly test as Dr. Stephen Esses. His office told Kaiser Health News the surgeon would have no comment.
Sunset Labs is part of a network of pain clinics and other medical businesses founded by Houston anesthesiologist Phillip C. Phan, according to Texas secretary of state filings and court records. Court records say Phan’s companies also own the facility where Moreno had her operation.
Three experts contacted by KHN said the lab grossly overcharged; they also doubted the need for the test.
“This just blows my mind,” said Jennifer Bolen, a former federal prosecutor and lab and pain management consultant. “It’s very high and incredibly out of the norm.”
Dan Bowerman, a medical fraud expert, called the lab bill “outrageous” and “unconscionable” and said it should have prompted an investigation.
“Sounds real fishy,” added Charles Root, a veteran industry adviser. He wondered if the lab had “misplaced the decimal point,” because such a test should cost a few hundred dollars, tops.
The lab disagrees.
Sunset’s billings “are in line with the charges of competing out-of-network labs in the geographical area,” lab attorney Justo Mendez said in an emailed statement.
Mendez said pain doctors agree that extensive urine testing is “the best course of action” and that a lab “is not in the position” to question tests ordered by a doctor.
Testing Booms As Opioid Epidemic Rages
Urine testing for patients with chronic pain has grown explosively over the past decade amid a rising death toll from opioid abuse. Pain doctors say drug testing helps them make sure patients are taking the drugs as prescribed and not mixing them with illegal substances.
Yet the testing boom costs billions of dollars annually and has raised concerns that some labs and doctors run urine tests needlessly — or charge exorbitant rates — to boost profits.
Some insurers have refused to pay, which can leave patients like Moreno threatened with ruinously high bills they had no idea they had incurred.
“Surprise bills larded with unexpected expenses and little explanation inflict sticker shock on vulnerable patients,” said James Quiggle, communications director of the Coalition Against Insurance Fraud, whose members include insurers, consumer groups and government agencies. Quiggle said many “puffed-up bills straddle a fine line between abuse and outright fraud.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Liz Moreno thought she was done paying for her back surgery in 2015 until a $17,800 bill for a urine drug test showed up nine months later. Her father, Paul Davis, a retired doctor from Ohio, settled the bill with the company for $5,000 to protect Liz’s credit rating.
Julia Robinson for KHN
hide caption
toggle caption
Julia Robinson for KHN
Moreno said her insurance covered the disc removal surgery in December 2015. She said the operation went well and she weaned herself off the hydrocodone pain pills. To her surprise, during a second appointment return about a month later, the surgeon’s office asked her to leave a urine sample.
“I didn’t think anything of it,” Moreno said of the test. “I said fine, whatever.”
More than a year later, she said, the lab phoned while she was driving and asked her to pay the $17,850 bill. The lab then sent her an invoice, dated March 10, 2017, which states: “based upon information from your health plan, you owe the amount shown.”
Luckily, her father, Dr. Paul Davis, was visiting her in Texas at the time. Davis, 66, is a retired family practice doctor from Findlay, Ohio.
Davis doubted the need for the test, not to mention what he thought was a sky-high price. He said the University of Findlay, where he helped train physician assistants, gave applicants a basic drug test at a cost of $174, while the local juvenile courts in Ohio paid $10 for a simple drug screen.
Fearing the bill would ruin his daughter’s credit scores, Davis said, he called Sunset and settled it in April 2017 by paying $5,000, which he said he now regrets. The lab sent Moreno a receipt that said it discounted her bill because of “financial need/hardship.”
Asked for comment, Blue Cross spokesman James Campbell said he couldn’t discuss a specific case but noted:
“We are disappointed as well as concerned about transparency whenever [any] member is surprised by an excessive charge for a seemingly routine service or received services that may not have been medically necessary.”
Campbell also said the lab was out-of-network and “we do not control how much they charge for services rendered.” The insurer encourages patients to confirm that all medical care they seek comes from medical providers in the Blue Cross network, he added.
Prices for urine tests can vary widely depending upon complexity and the technology used. Some doctors’ offices use a simple cup test, which can detect several classes of drugs on the spot. These tests rarely cost more than $200, and typically much less.
Bills climb higher when labs check for levels of multiple drugs and bill for each one, a practice insurers argue is seldom medically justified. But even labs sued by insurers alleging wildly excessive testing typically have billed $9,000 or less, court records show. One insurer sued a lab for charging $1,845 for a drug test, for instance.
Davis said Sunset Labs ignored his requests for a full explanation of the charges. In May, he filed a written complaint about the bill with the Texas attorney general’s office that included a copy of the bill and accused the lab of “price gouging of staggering proportions.”
“Young people just starting out, such as my daughter, may not have the ability to pay and this could result in damaged credit ratings or even bankruptcy,” he wrote.
Davis got a letter back from Attorney General Ken Paxton, who said the office would “review the information.” A spokesperson for Paxton told KHN: “We have received complaints about that business, but we can’t comment on anything else.” Sunset attorney Mendez said the lab is “not aware” of any such complaints.
In an interview, Davis also questioned the need for his daughter’s urine test because she received opioids only for a short period and the results would have had no impact on her treatment. In his complaint to the attorney general, Davis said the surgeon told him he ordered the tests because he feared possible retribution from the state medical licensing board for not testing patients who had been prescribed an opioid. The Texas Medical Board doesn’t require urine tests for patients receiving opioids for short-term pain, said spokesman Jarrett Schneider. That’s a “question of independent medical judgment as to whether the physician believes a drug test should be required,” he said.
Negative Reviews
Sunset Labs has an “F” rating with the Houston Better Business Bureau, which on its website posts an August 2017 complaint from a patient charged $16,150 for a urine test.
“This is not covered under my health insurance so I am expected to pay this excessive bill,” the complaint reads.
A second website that publishes government billing numbers of doctors and medical businesses includes a comment section with more than a dozen negative “reviews,” mostly complaints that the lab slammed patients with thousands of dollars in fees their insurers balked at paying.
In a pair of lawsuits filed in 2015, three doctors seeking to quit working at pain clinics operated by Phan accused the facilities of improper billing practices, including unnecessary urine testing. The doctors said they feared losing their medical licenses unless they severed their ties.
In one suit, Drs. Purvi Patel and Lance LaFleur also alleged that the pain clinics “pressured” doctors to overprescribe medical gear and genetic tests to insured patients “regardless of medical necessity.” The case did not go forward because the doctors did not pursue it. Neither doctor would comment.
In the second legal case, pain specialist Dr. Baominh Vinh said he resigned in April 2015 “based on certain questionable business practices … that are inconsistent with my ethical boundaries.” Vinh also alleged urine testing was overused. In a countersuit against Vinh, the pain clinics called his allegations a “falsehood” to justify violation of his employment contract.
The parties settled in March of last year. Terms are confidential, but a lawyer for the pain clinics said Vinh paid money to the company “and not vice versa.”
This is the debut of a monthly feature from Kaiser Health News and NPR that will dissect and explain real medical bills in order to shed light on prices in U.S. health care and to help patients learn how to be more active in managing costs. Do you have a medical bill that you’d like us to see and scrutinize? Submit it here and tell us the storybehind it.
How A Urine Test After Back Surgery Triggered A $17,800 Bill

{kind=link}
Liz Moreno thought she was done paying for her back surgery in 2015. But a $17,800 bill for a urine test showed up nine months later. Her father, Paul Davis, a retired doctor from Ohio, settled with the lab company for $5,000 in order to protect his daughter’s credit history.
Julia Robinson for KHN
hide caption
toggle caption
Julia Robinson for KHN
In her late 20s and attending college in Texas, Elizabeth Moreno suffered from debilitating back pain caused by a spinal abnormality. “I just could not live with the pain,” she says. “I couldn’t get dressed by myself, I couldn’t walk across my house, let alone to class, and nothing, no drug that had been prescribed to me, even dulled the pain.”
Moreno says she also tried chiropractic medicine and acupuncture, but they didn’t make the pain go away. Finally, a doctor at the student health center referred her to an orthopedic specialist who performed tests and concluded a disc was blocking nerves down her legs and needed to be removed. Moreno’s father, a retired Ohio doctor who had seen many failed back surgeries over his career, agreed it was the best course.
In late 2015, Moreno had the operation in Houston, which she described as “a complete success.” She gave it little thought when the surgical office asked her to leave a urine sample for a drug test.
Then the bill came.
Patient: Elizabeth Moreno, then 28, a student at Texas State University in San Marcos.
Total bill: $17,850 for a urine test in January 2016
Service provider: Sunset Labs LLC of Houston
Medical treatment: Moreno had a disc removed from her back in December 2015. Her surgeon prescribed an opioid painkiller, hydrocodone. At a follow-up office visit in mid-January 2016, the staff asked her to leave a urine sample, which she figured was routine. In March 2017, the lab sent her a bill for $17,850 for testing her urine for a slew of drugs, including cocaine, methadone, anti-anxiety drugs and several other drugs she had never heard of.
What gives: Urine drug testing has exploded over the past decade amid alarm over rising opioid overdose deaths. Many doctors who prescribe the pills rely on the urine tests to help reduce drug abuse and keep patients with chronic pain safe. Yet the tests have become a cash cow for a burgeoning testing industry, and critics charge that unneeded and often expensive ones are sometimes ordered for profit rather than patient care. Doctors can decide whether to test patients who take opioids for short periods, such as after an operation. Moreno’s surgeon would not discuss her urine test — why he ordered it and why the sample was tested for so many substances.
Three experts contacted by Kaiser Health News questioned the need for such extensive testing and were shocked to hear of the lab’s prices. They said these tests rarely cost more than $200, and typically much less, depending on the complexity and the technology used. Some doctors’ offices use a simple cup test, which can detect several classes of drugs on the spot and could be purchased for about $10. Bills can climb higher when labs run tests to detect the quantity of specific drugs and bill for each one, as the lab did here.
The experts said that the lab’s prices for individual tests were excessive, such as charging $1,700 to check for amphetamines or $425 to identify phencyclidine, an illegal hallucinogenic drug also known as PCP. They also criticized a charge of $850 for two tests to verify that her urine sample had not been adulterated or tampered with.
Moreno’s insurer, Blue Cross and Blue Shield of Texas, refused to pay any of the bill, arguing that the lab was out-of-network and thus not covered. Had it chipped in, it would have covered the service at $100.92, according to an explanation of benefits the insurance company sent to Moreno.
Sunset Labs says its list prices were “in line” with its competitors in the area. It also said doctors treating pain agree extensive urine testing is “the best course of action” and that a lab “is not in the position” to question tests ordered by a doctor.
Resolution: Fearing damage to his daughter’s credit rating, Moreno’s father, Dr. Paul Davis, paid the lab $5,000 to settle the bill in April 2017. A retired doctor, he also has filed a formal complaint about the bill with the Texas attorney general’s office, accusing the lab of “price gouging of staggering proportions.” The lab’s attorney said he was not aware of the complaint. A Texas attorney general’s spokesperson confirmed to KHN that the office had received complaints about the lab, but declined further comment.
The takeaway: When a physician asks for a urine or blood sample, always ask what it’s for. Insist that it be sent to a lab in your insurance network.
Source: Texas Attorney General complaint; interviews
This is the debut of a monthly feature from Kaiser Health News and NPR that will dissect and explain real medical bills to shed light on prices in U.S. health care and to help patients learn how to be more active in managing costs. Do you have a medical bill that you’d like us to see and scrutinize? Submit it here and tell us the story behind it.
Share Your Medical Bill With Us

{kind=link}
Kameleon007/Getty Images
NPR and Kaiser Health News are undertaking a project to investigate and dissect real-life medical bills.
We expect that examining the bills will shed light on the often surprising prices for health care in the U.S.
Along the way, we’re hoping to help people learn how to be more active and successful in managing the costs of their care.
Do you have a medical bill or explanation of benefits that you’d like us to see and scrutinize? Submit it here and tell us the story behind it.
We may use it, with your permission, in one of our monthly features.
If possible, insert the following lines into your .
–><!– Insert everything below in the . –>This form requires JavaScript to complete.
Powered by Screendoor.
Idaho Insurer Moves Ahead With Health Plans That Flout Federal Rules

{kind=link}
Health and Human Services Secretary Alex Azar faced questions Wednesday from the House Ways and Means Committee about Idaho’s move.
Jacquelyn Martin/AP
hide caption
toggle caption
Jacquelyn Martin/AP
It’s barely been two weeks since Idaho regulators said they would allow the sale of health insurance that doesn’t meet all of the Affordable Care Act’s requirements — a controversial step some experts said would likely draw legal scrutiny and, potentially, federal fines for any insurer that jumped in.
And on Wednesday, Blue Cross of Idaho unveiled a menu of new health plans that break with federal health law rules in several ways, including setting premiums based on applicants’ health.
“We’re trying to offer a choice that allows the middle class to get back into insurance coverage,” said Dave Jeppesen, the insurer’s executive vice president for consumer health care.
The insurer filed five plans to the state for approval and hopes to start selling them as soon as next month.
The Blue Cross decision ups the ante for Alex Azar, the Trump administration’s new Health and Human Services secretary. Will he use his authority under federal law to compel Idaho to follow the ACA and reject the Blues plans? Or will he allow state regulators to move forward, perhaps prompting other states to take more sweeping actions?
At a congressional hearing Wednesday, even as Blue Cross rolled out its plans, Azar faced such questions. “There are rules,” Azar said. “There is a rule of law that we need to enforce.”
However, he didn’t specifically indicate whether the federal government would step in.
Robert Laszewski, a consultant and former insurance industry executive, says it should. “If Idaho is able to do this, it will mean other … states will do the same thing,” he said. “If a state can ignore federal law on this, it can ignore federal law on everything.”
Idaho’s move stirs up more issues about the stability of individual insurance markets.
Policy analysts say that allowing lower-cost plans that don’t meet the ACA’s standards to become more widespread will pull younger and healthier people out of Obamacare, raising prices for those who remain. Supporters say that is already happening, so the lower-cost plans provide more choices for people who earn too much to qualify for subsidies to help them purchase ACA coverage.
Idaho’s move to allow such plans, announced in January, drew harsh and swift criticism.
“Crazypants illegal,” tweeted Nicholas Bagley, a law professor at the University of Michigan and former attorney with the civil division of the U.S. Department of Justice, who said that states can’t pick and choose which parts of federal law to follow. Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms, pointed out that health insurers could be liable for sharp fines if they are found to be in violation of the ACA.
But both Idaho regulators and Blue Cross officials say they aren’t worried.
Jeppesen said the ACA gives states regulatory authority “to make sure the market works and is stable,” and the insurer is simply “following what the state has given us guidance” to do.
Other insurers in Idaho are taking a much more cautious approach, telling The Wall Street Journal they aren’t stepping up immediately to offer their own plans.
Laszewski said they are likely waiting to see what legal challenges develop. “If I were running an insurance company, there’s no way I would stick my neck out until the high court has ruled in favor of this — and they’re not going to,” he said.
Jeppesen said his company has consulted with legal experts and is moving ahead with confidence. The aim is to bring people back into the market, particularly the young, the healthy and those who don’t get a tax credit subsidy and can’t afford an ACA plan.
For some people — especially younger or healthier applicants — the new plans, which the insurer has named Freedom Blue, cost less per month than policies that meet all ACA rules.
They accomplish that by limiting coverage. If they are allowed to be sold, consumers will need to weigh the lower premiums against some of the coverage restrictions and variable premiums and deductibles, policy experts say.
The plans, for example, will include a “waiting period” of up to 12 months for any pre-existing conditions if the applicant has been without coverage for more than 63 days, Jeppesen said.
Additionally, they cap total medical care coverage at $1 million annually. And premiums are based, in part, on a person’s health: The healthiest consumers get rates 50 percent below standard levels, while those deemed unhealthy would be charged 50 percent more.
All those conditions violate ACA rules, which forbid insurers from rejecting coverage of preexisting conditions or setting dollar caps on benefits or higher premiums for people with health problems.
But the rates may prove attractive to some.
Premiums for a healthy 45-year-old, for example, could be as low as $195 a month, according to a comparison issued by the insurer, while a 45-year-old with health problems could be charged $526. In that case, the 45-year old would find a lower price tag — $343 a month — for an ACA-compliant bronze plan.
While Freedom Blues plans cover many of the “essential health benefits” required under the ACA, such as hospitalization, emergency care and mental health treatment, they do not include pediatric dental or vision coverage. One of the five plans doesn’t include maternity coverage.
When compared with one of the Blues’ ACA-compliant plans — called the Bronze 5500 — the new standard Freedom Blue plan’s annual deductibles are a mixed bag.
That’s because it has two separate deductibles — one for medical care and one for drugs. If a consumer took only generic drugs, the new plan would be less expensive, according to details provided by the plan. But with a $4,000 deductible for brand-name drugs, the Freedom Blue plan requires more upfront money before full coverage kicks in than the ACA-compliant plan it was compared with.
Jeppesen said the insurer hopes to attract many of the “110,000 uninsured state residents who cannot afford [ACA] coverage.”
That’s the total number of uninsured people who earn more than 100 percent of the federal poverty level in the state, he said.
Sarah Lueck, senior policy analyst for the Center on Budget and Policy Priorities, cautioned that some of those residents might actually be eligible for subsidies under the ACA, which are available to people earning up to four times as much.
“Many … could be getting subsidies for more comprehensive coverage through the [ACA-compliant state exchange] and would be better off,” Lueck said.
Kaiser Health Newsis a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.